










 Inglés
Inglés




 Permalink
PermalinkRSBO (Online)
ISSN 1984-5685
RSBO (Online) vol.10 no.2 Joinville abr./jun. 2013
CASE REPORT ARTICLE
Hidden caries' challenge diagnosis: case report
Fernanda Mara de Paiva BertoliI; Bruno Marques da SilvaI; Mariana DalledoneI; Estela Maris LossoI
I School of Dentistry, Positivo University – Curitiba – PR – Brazil.
ABSTRACT
Introduction: Hidden caries is a term used to describe occlusal dentine caries that is missed on a visual examination, but is large and demineralised enough to be detected by another exam for example, radiographs.
Case report: This article reports a case of large dentine caries, which presented as to be a small pit-and-fissure carious lesion on the occlusal surface of the right mandibular permanent first molar in a 10-year-old girl. The treatment included root canal treatment and the sealing of the cavity with composite resin.
Conclusion: Careful visual examination, with cleaning and drying of teeth, associated to bitewing radiographs may improve occlusal caries detection. Dentists should examine bitewing radiographs carefully for proximal caries and occlusal demineralization. Radiographs are an effective method of caries diagnosis that can avoid large destruction and allows less invasive treatment.
Keywords: dental caries; bitewing radiograph; diagnosis.
Introduction
Hidden (or occult) caries is a term used to describe a carious lesion seen in dentine through bitewing radiograph that clinically, the occlusal enamel appears healthy or slightly demineralized 3,10,11. They are found in pit or fissure lesions that develop through tiny enamel defects, progressing under seemingly intact tooth structure. The etiology of hidden caries is still unknown, although some authors believed to be related to the massive use of fluorides, which act in the re-mineralization of occlusal enamel lesions, masking their evolution3,4,9.13,15,17. However, Hashizume et al. 6 determined the prevalence of clinically undetected occlusal dentine caries (hidden caries) in a group of 8-10 year-old children before and after public water supply and dentifrice fluoridation and the results indicated that fluoride is not responsible for the increase in hidden occlusal caries 6. Many dental practitioners find hidden caries when they start to intervene operatively into what they suspect is a small carious lesion, revealing instead an extended carious lesion that is well into dentin 4.
Dental caries management demands detection of carious lesions at an early stage. In the last 30 years the diagnosis of occlusal caries became more complex and many authors believe that it is possibly due to the increase in the use of fluoride 3,14. It has been widely reported that the prevalence of occlusal caries is significantly underestimated by clinical examination alone 6, and there is no "gold standard" in the caries detection 12. Besides that, complex occlusal fissure morphology, lesion extension and nature of the lesion can lead to misdiagnosis, and frequently dentine lesions are detected on bitewing radiographs 9. Nevertheless this type of examination is not totally effective and recent studies have been done and other methods, beyond the traditional (visual inspection aided by compressed air, tactile examination with a dental explorer and radiographic examination) in caries detection have been developed. The most current methods and devices are: alternating current impedance spectroscopy technique (ACIST), computer-aided radiography (CAR), dental digital radiography (DDR), digital imaging fiber-optic transillumination (DIFOTI), DIAGNOdent, diagora image plate system (DIPS), diode laser fluorescence (DLF), electrical conductance fixed frequency (ECFF), endoscope filtered fluorescence (EFI), qualitative light-induced laser fluorescence (QLF), visualix high-definition imager and intra-oral sensor technology 1,14,17. However, dentists seem to be resistant in adopting these new caries detection and treatment modalities 18.
Case report
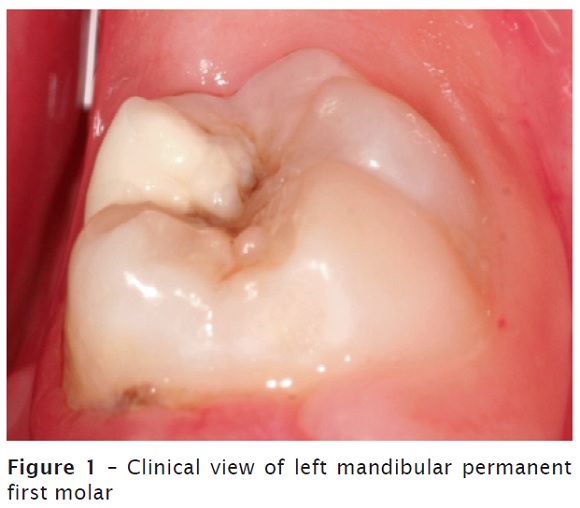
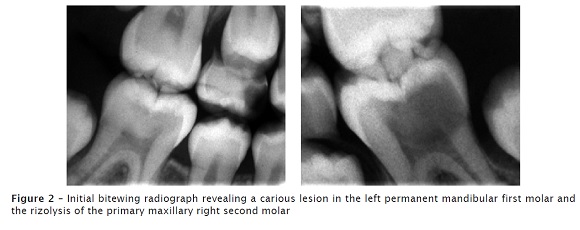
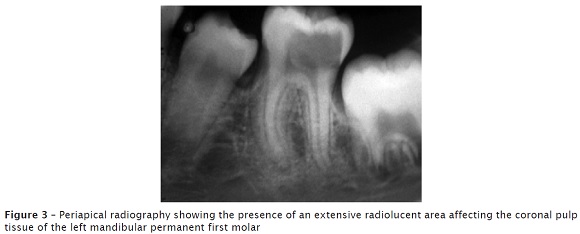
A 10-year-old girl was referred to pediatric dentistry clinic at Positivo University with complaint of toothache. No relevant medical history was reported during the anamnesis. After tooth prophylaxis, the clinical examination showed that she was at mixed dentition with caries cavities in the teeth #55 and #65. A large pit and demineralization in the occlusal surface was observed in teeth #36 and #46, although these teeth appeared healthy (figure 1). Bitewing radiograph revealed rizolysis of teeth #55 and #65 and a large radiolucent area in the coronal dentin of the tooth #36 affecting the pulp tissue (figures 2 and 3).
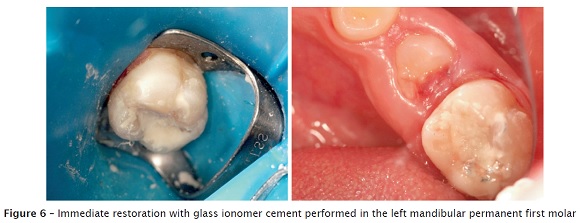
First of all, the patient was anesthetized, and rubber dam isolation was performed. Access to the carious lesion was made using a diamond bur in a high-speed with water irrigation. Dentine caries removal was completed by hand and rotary instruments and the pulp tissue was exposed and removed (figure 4). The root canals were cleaned, dried and filled (figure 5). The coronal cavity was restored with glass ionomer cement (figure 6).


Discussion
According to the National Institutes of Health, Consensus Development Conference Statement 2001, dental caries is now defined as ‘‘an infectious, communicable disease resulting in the destruction of tooth structure by acid-forming bacteria found in dental plaque, an intraoral biofilm, in the presence of sugar" 5. The most cariogenic organisms are adherent streptococci such as Streptococcus mutans that starts the process, S. sobrinus, and the bacillus Lactobacillus 10, among other factors as changes in salivary components and exposure to fluorides.
In the case reported, the tooth affected was the mandibular permanent first molar, that according to DeJean et al. 3 is the most common tooth affected by hidden caries, because is the first permanent tooth to erupt and it has many pit and fissures 3.
Therefore, one may conclude that adopting the implementation of bitewing radiographs in clinical practice is an important auxiliary tool for diagnosing hidden caries, even in "caries-free" patients 3,7,9. Because of the low attenuation of radiation in the demineralized zone, the typical radiographic appearance of caries is a radiolucent area; however, 40% to 60% of tooth decalcification is required to produce the radiographic image. An initial or incipient lesion may not be seen radiographically 16.
Although the incidence of caries is decreasing, mainly in developed countries, occlusal pit and fissure is still present and it is well accepted that bitewing radiograph has additional benefit in the detection of non-cavitated and small cavitated lesions 7,11,14.
It has been postulated that the incidence of hidden caries is increasing due to the use of fluoride, which reduces or makes absent the demineralization characteristic of the carious lesion of enamel, hidding the caries progression into dentine 3,4,14. The detection rate of such lesions will depend upon the prevalence of caries in the population and the frequency with which bitewing radiographic examinations are performed.
In the present case, radiographs were properly used for the diagnosis of hidden caries, which seemed clinically like a slight enamel demineralization around de occlusal pit, as related by Candido et al. 2.
Early and accurate diagnosis of occlusal caries enables successful prevention and minimal restorative techniques intervention, ending the common evolution from occlusal restorations to cusp restorations, crowns, and Endodontics or even tooth loss 2.
References
1. Barnes CM. Dental hygiene participation in managing incipiente and hidden caries. Dent Clin N Am. 2005 Oct;49(4):795-813. [ Links ]
2. Candido LA, Oliveira TM, Sakai VT, Silva SMB, Abdo RCC, Machado MAAM. The importance of radiographic diagnosis of incipiente occlusal caries – case report. Odontologia Clín Científ. 2008 Jan/Mar;7(1):87-91.
3. DeJean KS, Caldas LD, Gois DN, Souza CS. Hidden dental caries: a study of diagnosis and prevalence. ClipeOdonto – UNITAU. 2009 Dec;1(1):7-13.
4. Dennison JB, Hamilton JC. Treatment decisions and conservation of tooth structure. Dent Clin N Am. 2005 Oct;49(4):825-45. [ Links ]
5. Diagnosis and Management of Dental Caries Throughout Life. NIH Consensus Statement Online. 2001;18(1):1-24.
6. Hashizume LN, Mathias TC, Cibils DM, Maltz M. Effect of the widespread use of fluorides on the occurrence of hidden caries in children. Int J Paediatr Dent. 2012 Feb;20:1-5. [ Links ]
7. Hopcraft MS, Morgan MV. Comparison of radiographic and clinical diagnosis of approximal and occlusal dental caries in young adult population. Community Dent Oral Epidemiol. 2005 Jun;33(3):212-8. [ Links ]
8. Latta MA, Naughton WT. Bonding and curing considerations for incipient and hidden caries. Dent Clin N Am. 2005 Oct;49(4):889-904. [ Links ]
9. Mestriner SF, Pardini LC, Mestriner WJ. Impact of the bitewing radiography exam inclusion on the prevalence of dental caries in 12-year-old students in the city of Franca, São Paulo, Brazil. J Appl Oral Sci. 2006 Jun;14(3):167-71. [ Links ]
10. Mount JH. Defining, classifying, and placing incipient caries lesions in perspective. Dent Clin N Am. 2005 Oct;49(4):701-23. [ Links ]
11. Newman B, Seow WK, Kazoullis S, Ford D, Holcombe T. Clinical detection of caries in the primary dentition with and without bitewing radiography. Australian Dental Journal. 2009 Mar;54(1):23-30. [ Links ]
12. Nyvad B. Diagnosis versus detection of caries. Caries Res. 2004 May-Jun;38(3):192-8. [ Links ]
13. Pereira RF, Gomes RH, Volpato LE. Occult caries lesion: restoration using the occlusal matrix technique. Rev INPEO de Odontologia. 2008 Jul;2(1):1-76. [ Links ]
14. Strassler HE, Porter J, Serio CL. Contemporary treatment of incipient caries and the rationale for conservative operative techniques. Dent Clin N Am. 2005 Oct;49(4):867-87. [ Links ]
15. Thompson VP, Kaim JM. Nonsurgical treatment of incipient and hidden caries. Dent Clin N Am. 2005 Oct;49(4):905-21. [ Links ]
16. Yang J, Dutra V. Utility of radiology, laser fluorescence, and transillumination. Dent Clin N Am. 2005 Oct;49(4):739-52. [ Links ]
17. Zanardo A, Rego MA. Occlusal caries diagnosis in permanent teeth: an in vitro study. Ciênc Odontol Bras. 2003 Jul-Sep;6(3):50-7. [ Links ]
18. Zandoná AF, Zero DT. Diagnostic tools for early caries detection. JADA. 2006 Dec;137(12):1675-84. [ Links ]
 Corresponding author:
Corresponding author:
Estela Maris Losso
Rua Professor Pedro Viriato Parigot de Souza, n. 5.300 – Campo Comprido
CEP 81280-330 – Curitiba – PR – Brasil
E-mail: lossoem@gmail.com
Received for publication: December 1, 2012
Accepted for publication: December 20, 2012
