















 Permalink
PermalinkRSBO (Online)
ISSN 1984-5685
Case Report Article
Periodontal plastic surgery for treatment of gummy smile with cosmetic restauration treatment
Keith Jimmy Gonçalves I; Gabrielle Gobbo Agnoletto II; Leonardo Fernandes da Cunha III; Carmen Mueller Storrer III; Tatiana Miranda Deliberador III
I Dentistry Course, Paranaense University – Francisco Beltrão – PR – Brazil
II Program of Post-Graduation in Dentistry, Positive University – Curitiba – PR –Brazil
III Dentistry Course, Positive University – Curitiba – PR – Brazil
ABSTRACT
Introduction: Today, the appreciation of aesthetic dentistry by society brought to the search for materials and techniques that improve the appearance of smile, which is essential in maintaining physical and mental health of the patient. Objective: This study aimed to report a case of gummy smile involving Periodontics and Restorative Dentistry. Case report: This case, despite other possible alternatives, was solved through periodontal surgery (clinical crown augmentation associated with osteotomy) and indirect restorations with porcelain crowns. Conclusion: In our experience this procedure is safe, predictable, with minimal risks or side effects, and it is a treatment option for these cases.
Keywords: gummy smile; periodontal plastic surgery; short clinical crown.
Introduction
In an extremely competitive society in which we are inserted, the aesthetic appearance exerts great importance in the acceptance and self-stem of individuals 10. In this question, a pleasant smile is considered a symbol of beauty and well-being in the modern society. Other authors 3 claim that the shape, the position of the teeth and the gum tissue levels can influence on the aesthetics of the smile. The smi le is the only universal human expression, transcending language, culture, race, gender, time and socioeconomic differences. In addition, it communicates love, joy, attraction, vitality, health, friendship, compassion, acceptance and security 12.
The smile has always served as a way of fast and effectively nonverbal communication to make contact.
Some authors 3,5,9,15 cite the characteristics of a perfect smile. Da Silva 5 states that the perfect smile is characterized by exposure of the total length of the upper anterior teeth up to the premolars, showing the incisal curve of these teeth parallel to inner curvature of the lower lip, and slightly touching or leaving a minimum space with the lower lip.
The appearance of gingival tissue also has an important role in the overall aesthetic structure, especially in patients with a medium or high smile line. Harmony of color, texture, shape and architecture of the gingival tissue is extremely important in the aesthetic appearance of the smile. Ideally, the outline of the gingival margin would be parallel to the incisal line and follow the guidance of horizontal reference lines 4. In addition, it shall provide a suitable scalloped design, with presence of interdental papillae. This ideal contour tends inevitably to change in cases where there is loss of periodontal support.
The dentist should balance the aesthetic needs of the patient with the functional requirements, while harmonically matching the unique characteristics of each individual with the face 14. A frequent complaint of patients seeking cosmetic dentistry resources relates to dissatisfaction with gum excess exposed during the smile, so-called gingival or gummy smile 11. The gummy smile is that showing more than 3 mm of gingiva while the "normal" smile shows 2 mm when the upper lip moves apically 17.
The etiology of gummy smile is related to several factors: changed passive eruption, increased gingival volume due to plaque accumulation or use of drugs and vertical excess of maxilla 1.
Based on the correct diagnosis, the treatment options are: orthognathic, orthopedic, and/or surgical therapy, depending on the etiology, severity of gingival exposure and the age of the patient 13. Surgical therapy includes the increase of clinical crown to reduce the amount of gums exposed, increasing the height of the anterior teeth, aiming to follow the contour of the upper lip; requiring, in most cases, a biological space to reestablish osteotomy 9,15. The gingivectomy/gingivoplasty can also be used to change the contour of the teeth and their proportions 8. In association with these therapeutic options, the restorative dentistry contributes by returning the proportion and harmony of the crowns of the teeth, through direct or indirect methods 2. Understanding the etiology and the treatment options is crucial in the process of treatment of the patient with gummy smile 20.
This study aimed to present a surgical restorative protocol, including periodontal surgery of gingival recontouring with osteotomy and rehabilitation with porcelain crowns to improve esthetics and function in a patient with over-exposed gingival smile and short clinical crowns.
Case report
Patient R.J.B., female, aged 29 years was referred to the Clinics of Periodontics of Positive University, by the Clinics of Restorative Dentistry, complaining about short teeth and with extreme gingival exposure during smiling (figure 1).
The patient examination comprised: periodontal probing of all teeth, photographs, radiographic examination, impression of the maxilla and mandible, waxing-up diagnosis. All treatment plan and the likely outcome of the treatment was showed to patient.
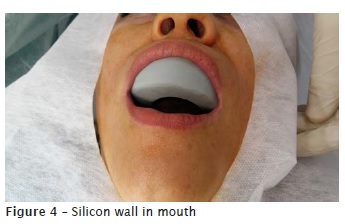
A silicon wall was constructed (figure 2), filled with bisacrylic resin (figure 3) and taken to the mouth of the patient (figure 4), thus obtaining the size of the teeth that had been previously waxed (figure 5). Before the surgical procedure, extraoral antisepsis was performed with PVPI, and intraorally with 0.12% chlorhexidine digluconate.
The patient was anesthetized with 2% mepivacaine vasoconstrictor. The bisacrylic resin mockup was used as a surgical template. An inner bevel incision was performed (figure 6) following the gingival margins of the surgical template, from the left to the right maxillary premolars. The template was removed, and a second intrasulcular incision (figure 7) was performed on these teeth to allow the removal of the gingival tissue. A full-thickness no-relaxing flap was raised, exposing the local bone tissue (figure 8). The surgical guide was placed on the position again to evaluate the distance between its end and the marginal bone tissue.
Next, the osteotomy and osteoplasty was executed with the aid of a spherical diamond bur at high speed (under irrigation with saline) and Ochsenbein micro chisels, aiming to restore the biological distances between the bone and the end of the future prosthetic preparation, according to the surgical template. After osteotomy and osteoplasty (figure 9), copious irrigation with saline was performed and a continuous suture was executed with nylon 5-0 (figure 10).
The patient received post-operative instructions and the following medications were prescribed: antibiotic (Amoxillin – 500 mg) every 8 hours for 7 days, analgesic and anti-inflammatory (Ibuprofen-600 mg) every 12 hours for 4 days, and mouthwashes with 0.12% chlorhexidine digluconate every 12 hours for 14 days. The suture was removed after 10 days. Elapsed 4 months, the patient was released to start the prosthetic treatment. After the end of treatment, the patient was followed-up for 1 year, without changes in the restorative and periodontal outcome.










Discussion
Currently, health is no longer characterized only as the absence of disease, but also as a state of mind; and that state of mind of the person can be evaluated by facial expression, identified mainly by the brightness of the eyes and the smile 10. In this context, the teeth, especially the anterior teeth, can be considered essential to the beauty of the individual, providing freedom to smile, favoring a good social conviviality and thus promoting health at the widest aspect.
For health promotion, the teeth need to be within the current adopted standards of beauty, that is, well-positioned and aligned clear teeth with defined shape as equal as the contralateral teeth. And with a great relationship with the group of teeth to which they belong. Similarly, the anterior teeth must present an excellent relationship with the lips, smile and face. The integration of restoration with the gums, lips, smile and face of the patient is paramount in the success of esthetic restorative procedure.
The proportionality between the teeth depends on the height and the width, with great application in extensive reconstructions, aiming to obtain the harmony between the smile and face. A nice and essential feature of the maxillary anterior teeth is the length proportionately greater than the width. The labial surface of these teeth must have, whenever possible, grooves at the horizontal direction, to "reduce", and vertical grooves, to "increase" the length of the tooth. Also, the upper lip line determines the height of the gingival margin, which must be parallel to the contour of the upper lip. The lower lip line may have various forms and its curvature should be more or less pronounced, determining the length of the upper teeth. The incisal edge is formed by the line of the upper teeth and should be parallel to the contour of the lower lip. All these parameters are important for the dental recontouring, allowing the total balance between the analyzed structures and the teeth, making the esthetic treatment successful.
The gingival contour's zenith, as clinical parameter to restore the dental and gingival esthetics at the anterior region of the maxilla, is a key factor 18. It is suggested to locate the gingival contour of canines at similar level or slightly apically than at central incisors, while a more coronal gingival contour is suggested for the lateral incisors.
Various methods have been documented including gingivectomy, flap surgery bone contour, apically repositioned flap surgery, orthodontic therapy 16. Excessive gingival exposure is sometimes caused by vertical maxillary excess and the middle third of the long face. Surgical crown augmentation is not sufficient in these cases and the maxilla must be treated surgically with orthognathic surgery. The risk-benefit ratio must be carefully evaluated in such cases. An interdisciplinary approach is vital in such cases when the patient is unwilling to undergo major surgery.
In this case report, the patient had gummy smile caused by excessive vertical maxillary growth, disharmony of width/height proportion and of the gingival zenith contour of the maxillary anterior teeth. For psychological and financial issues, the proposed treatment plan for the patient was an association of periodontal plastic surgery with osteoplasty and osteotomy, with subsequent indirect esthetic restoration with porcelain.
The restorative therapy should be planned in cases of excessive gingival exposure in the following situations: (1) short clinical crowns because of the loss of tooth structure; (2) existing defective restoration, or patient's esthetic complaint; and (3) cases of root exposure, because of periodontal therapy causing hypersensitivity of teeth and esthetic disabilities.
In this case report, care was taken regarding the preservation of a healthy periodontium, because this is a critical point for the long-term success of the restored tooth 7. The Dentists must constantly balance the restorative and esthetic needs of the patients with the periodontal health. A factor of particular importance is the potential that results in the periodontium damage when the margins are subgingivally. The crown margins positioned subgingivally were associated with gingival inflammation, leading to the invasion of the biological space, while the crown margins located supragingivally were associated with a lower gingival inflammation 19. Supragingival placement of the restoration margins allows ease of impression, cleaning and secondary caries detection and is associated with the maintenance of probing depths. Subgingival restorations can have harmful effects on neighboring hard and soft tissues, especially when they invade the junctional epithelium and the connective tissue above the bone crest. These restorations subgingivally placed have been associated with gingival inflammation, loss of connective tissue insertion and bone resorption. We agree with Simon et al. 21 by saying that one of the goals of restorative dentistry is to create an esthetic ideal for the patient's smile. Advances in dental materials and laboratory techniques have led to excellent mimicking of natural dentition with crowns, veneers and composite resin restorations. However, some patients with gingival and skeletal deformities may require a more complex esthetic rehabilitation. For these challenging patients, a multidisciplinary approach may be beneficial to improve the balance and harmony between all three components of the smile: lips, teeth and gums. From the dentist's point of view, we agree with Deliberador et al. 6, who claims that it is important to keep in mind that the gingival excess may be the result of various etiological factors; and when the cause of this condition is identified and a precise diagnosis is obtained, a well formulated plan will produce aesthetic and functional results, a statement also claimed by Mezzalira 14.
Conclusion
Understanding the etiology and the treatment options is crucial in the treatment process of the patient with gummy smile. The use of silicone template establishes a predictability about the size and shape of the teeth, promoting faster work. The interaction between Periodontics and Restorative Dentistry demonstrated a potential and advantageous interactivity between the areas. Periodontal plastic intervention targeted to the supporting and covering tissues demonstrated adequate gingival recontouring, while restorative procedures enabled effectively reconstruction and cosmetic of the area rehabilitated. Therefore, the multidisciplinary actions allowed providing the functional and esthetic rehabilitation, raising the patient's self-esteem and well-being.
References
1. Araújo M, Kina S, Brugera A. Manejo do sorriso gengivoso. Revista Dental Press de Periodontia e Implantologia. 2007;1(1):68-75. [ Links ]
2. Biniraj KR, Janardhanan M, Sunil MM, Sagir M, Hariprasad A, Paul TP et al. A combined periodontal – prosthetic treatment approach to manage unusual gingival visibility in resting lip position and inversely inclined upper anterior teeth: a case report with discussion. Journal International Oral Health. 2015;7(3):64-7.
3. Cairo F, Graziani F, Franchi L, Defraia E, Prato GPP. Periodontal plastic surgery to improve aesthetics in patients with altered passive eruption/gummy smile: a case series study. International Journal of Dentistry. 2012;1-6.
4. Caroli A, Moretto SG, Nagase DY, Nobrega AA, Oda M, Vieira GF. Avaliação do contorno gengival na estética do sorriso. Revista Instituto Ciência Saúde. 2008;26(2):242-54.
5. Da Silva CVT. A estética do sorriso. Especialista. 2013;1-60.
6. Deliberador TM, Vieira JS, Lopes TR, Giovanini AF, Zielak JC, Brambilla CFF. Cirurgia plástica periodontal para correção de sorriso gengivoso. Revista PerioNews. 2013;7(3):281-6.
7. Ganji KK, Patil VA, John J. A comparative evaluation for biologicwidth following surgical crown lengthening using gingivectomy and ostectomy procedure. International Journal of Dentistry. 2012;1-9.
8. Garber DA, Salama MA. The aesthetic smile: diagnosis and treatment. Periodontology 2000. 1996;11(1):18-28.
9. Geron S, Atalia W. Influence of sex on the perception of oral and smile esthetics with different gingival display and incisal plane inclination. The Angle Orthodontist. 2005;75(5):778-84.
10. Holanda DBV, Simões DMS, Khalili JB. Recontorno cosmético em dentes anteriores superiores: relato de caso clínico. Revista Dental Press de Estética. 2006;3(1):49-58.
11. Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS et al. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. The Angle Orthodontist. 2009;79(1):70-7.
12. Itikawa DB, Oliveira MBRG, Cardoso PC, Lucca PCC. O impacto do aumento dos incisivos superiores na atratividade e rejuvenescimento do sorriso. Rev Odontol Bras Central. 2010;19(49).
13. Kaku M, Kojima S, Sumi H, Koseki H, Abedini S, Motokawa M et al. Gummy smile and facial profile correction using miniscrew anchorage. The Angle Orthodontist. 2012;82(1):170-7.
14. Mezzalira MF. Reabilitação estética com laminados de porcelana. Especialista. 2011;1-26.
15. Morris ML. Suturing techniques in periodontal surgery. Periodontics. 1965;3:84-9.
16. Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. Journal of Indian Society of Periodontology. 2011;15(4):421-4.
17. Pascotto RC, Moreira M. Integração da odontologia com a medicina estética: correção do sorriso gengival. Revista Gaúcha de Odontologia. 2005;53(3):171-5.
18. Rocha EP, Meireles GCS, Ramacciato JC. Avaliação da percepção de profissionais da implantodontia sobre estética. Ciência & Desenvolvimento. 2013;6(1):132-45.
19. Sharma A, Rahul GR, Poduval ST, Shetty K. Short clinical crowns (SCC) – treatment considerations and techniques. Journal Clinical and Experimental Dentistry. 2012;4(4):230-6.
20. Silberberg N, Goldstein M, Smidt A. Excessive gingival display – etiology, diagnosis, and treatment modalities. Quintessence International. 2009;40(10):809-18.
21. Simon Z, Rosenblatt A, Dorfman W. Eliminating a gummy smile with surgical lip repositioning. Journal of Cosmetic Dentistry. 2007;23(1):102-9.
22. Sousa SJB, Magalhães D, Silva GR, Soares CJ, Soares CJ, Soares PFB et al. Cirurgia plástica periodontal para correção de sorriso gengival associada a restaurações em resina composta: relato de caso clínico. Revista Odontológica do Brasil Central. 2010;19(51):362-6.
23. Zanetti GR, Brandão RCB, Zanetti LSS, De Castro GC, Borges Filho FF. Integração orto-perio-prótese para correção de assimetria gengival – relato de caso. Revista Dental Press de Estética. 2007;4(4):50-60.
 Corresponding author:
Corresponding author:
Keith Jimmy Gonçalves
Av. Julio Assis Cavalheiro, 1401
Edifício Leonardo da Vinci, apto 202
CEP 85601000 – Francisco Beltrão
Paraná – Brasil
E-mail: jimmy@prof.unipar.br
Received for publication: January 23, 2017
Accepted for publication: March 6, 2017
