










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.40 Canoas Jan./Jun. 2015
Turner syndrome case report: A multidisciplinary approach
Relato de caso de síndrome de Turner: uma abordagem multidisciplinar
Guilherme ThiesenI; Mariana Cezar IlhaII; Tássia Silvana BorgesI; Maria Perpétua Mota FreitasIII
I are doctoral student of Dentistry at Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II is MSc student of Dentistry at ULBRA, Canoas, RS, Brazil
III is professor at the Graduate Program in Dentistry, ULBRA, Canoas, RS, Brazil
ABSTRACT
Turner syndrome (TS) was first reported in the literature in 1938 by Laurel Thatcher Ulrich and Henry Turner. This chromosomal alteration only affects female individuals, who have monosomy of the X chromosome. Only one X chromosome is functional, while the other sexual chromosome is either absent or abnormal. The main oral characteristics are transverse deficiency of the maxilla, mandibular retrognathism, anterior open bite, cleft palate, premature dental eruption, and alterations in the shape, size and thickness of teeth, with an increased number of roots on the first and second premolars. The objective of this study was to describe the clinical case of a patient with TS undergoing orthodontic treatment, and to emphasize the importance of a multidisciplinary approach to patients with TS.
Keywords: Turner Syndrome; Corrective Orthodontics; Genetics.
RESUMO
A síndrome de Turner (ST) foi relatada pela primeira vez na literatura em 1938, por Laurel Thatcher Ulrich e Henry Turner. Esta alteração cromossômica afeta somente pacientes do gênero feminino, apresentando uma monossomia do cromossomo X. Isso significa que apenas um cromossomo X é funcional, sendo o outro cromossomo sexual inexistente ou anormal. As principais características orais observadas são deficiência transversal da maxila, retrognatismo mandibular, mordida aberta anterior, fissuras palatinas, erupções dentárias precoces, alterações na forma, tamanho e espessura dos dentes, com aumento do número de raízes nos primeiros e segundos pré-molares. O objetivo deste trabalho foi descrever um caso clínico de uma paciente com ST submetida a tratamento ortodôntico e ressaltar a importância de uma abordagem multidisciplinar para estes pacientes.
Palavras-chave: Síndrome de Turner; Ortodontia Corretiva; Genética.
INTRODUCTION
Turner syndrome (TS) was first described by Henry Turner and Laurel Thatcher Ulrich in 1938 and is also known as monosomy X or Bonnevie-Ulrich syndrome. It is a condition characterized by monosomy of the X chromosome and complete or partial absence of the second sex chromosome 1. It only occurs in females and is the most common sex chromosome abnormality in females. The estimated prevalence rate is one case in 2,500 live female births 2,3.
Women affected by this syndrome develop a specific model of skeletal and dental features. This includes abnormal craniofacial growth, reduction of the transverse dimensions of the maxilla, mandibular sagittal deficiency, high palatal arch, cleft palate, malocclusion, premature dental eruption and changes in tooth shape and size 4-6. The posterior cranial base is shortened, and the angle of the base of the skull is flattened, leading to a retrognathic position of the mandible. The result is a small and wide mandible combined with a narrow maxillary arch 4. These deviations usually correspond to Angle Class II malocclusion, anterior open bite, and posterior crossbite 7.
These patients have dentition characterized by premature dental development, although the sequence of tooth eruption does not differ from the general population. By means of radiography, it is possible to observe anomalies of root morphology, such as length reduction and abnormal shape. The most frequently observed radiographic changes are two roots on the mandibular first and second premolars, with complete development of mesial and distal roots. There are also cases of agenesis of incisors, canines and premolars reported in the literature 5.
These features can lead to disorders of dental occlusion and this study reports on the clinical case of a patient with TS and the orthodontic treatment received. The article also serves to emphasizes the importance of a multidisciplinary approach to TS patients.
CASE REPORT
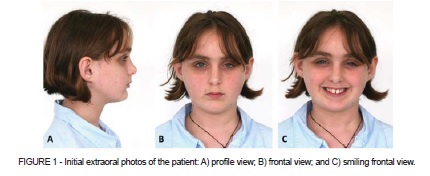
A Caucasian girl was referred at the age of 11 years and 1 month to a private office for an orthodontic consultation. The primary complaint was protrusion of maxillary incisors. The patient reported that she had TS and that she had been on endocrine treatment for approximately 3 years, taking growth hormones (HGH, also known as somatropin) to stimulate her skeletal growth potential to its limit. She had a 45,X/46,XX mosaic karyotype and streak ovaries.
Extraoral examination revealed a relatively symmetrical face, normal lower anterior facial height, convex profile with mandibular deficiency, interlabial gap, nasobuccal airflow, and a habit of lip sucking (Figure 1).
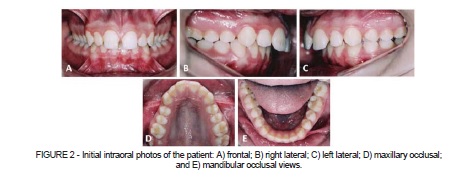
The permanent dentition was analyzed by intraoral examination, finding central incisors exhibiting a typical cervico-incisal convergence of the proximal surfaces, with a biconvex "barrel" shape. There were also whitish spots of enamel hypoplasia on the incisal and occlusal edges of some dental elements, particularly on maxillary elements. The patient also exhibited 8 mm overjet and 80% overbite, maxillary atresia with ogival palate and Class II, Division 1 malocclusion, with maxillary diastemas and no midline deviation (Figure 2).
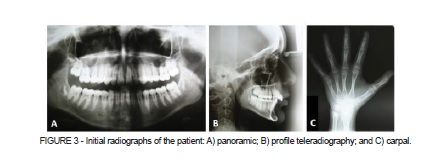
Radiology did not reveal abnormal root morphology. Cephalometric analysis using profile teleradiography showed skeletal Class II with mandibular retrusion and proclined maxillary incisors and mandibular incisors, well positioned in the jawbones. Carpal radiography revealed that the patient had entered the surge growth phase of puberty and so immediate facial orthopedic treatment was indicated (Figure 3).
Since the maxillary atresia would become more evident as a result of sagittal correction treatment, orthodontic planning included fitting a Hyrax appliance to the upper arch. This appliance was also used to anchor a Herbst appliance for mandibular advancement (Figure 4). Interception with the Herbst appliance took 9 months and was followed by corrective orthodontic treatment lasting 16 months.

During periodic consultations for orthodontic maintenance, the patient was given guidance and supervision with regard to oral hygiene habits, such as proper use of toothbrush and fluoride toothpaste and using dental floss for plaque control.
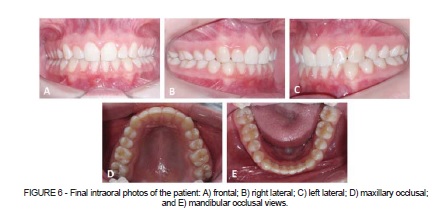
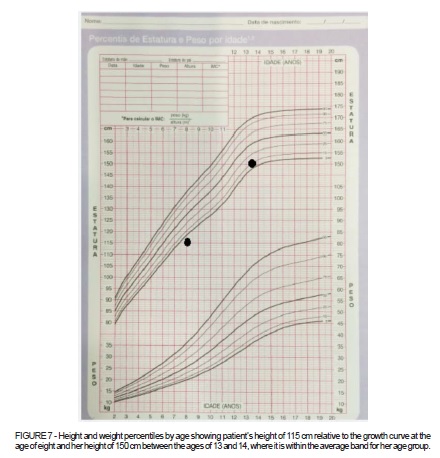
After completion of the treatment, satisfactory results were observed with regard to dentofacial components (Figure 5 and 6). At the conclusion of orthodontic and endocrine therapy, the patient exhibited a positive somatic growth pattern, within the median curve on the growth chart (Figure 7).

DISCUSSION
It is extremely important that the treating health professional knows the natural history of TS, since ongoing management of the condition is basically centered on treating clinical manifestations. One of the strategies is hormonal treatment, which significantly improves these patients' quality of life. Nowadays this is the most recommended therapeutic approach 8,9. Although most patients do not exhibit hormone deficiencies, treatment with HGH can help to normalize skeletal growth when properly administered 9,10. In this patient's case, the hormone replacement therapy administered resulted in a satisfactory outcome, since the initial estimation had been a final height far below the average population if she did not receive this treatment (Figure 7). This was of significant relevance to treatment of the patient's facial skeletal disharmony, since growth in body height is closely related to growth of the craniofacial structures 11.
Over the last 50 years, HGH has been widely used to treat growth disorders. Usage has been increasing since 1960, when biosynthesis was achieved. Somatropin is the biosynthetic form of growth hormone and it significantly increases patients' growth speed and final height 12,13.
The main predictive factor for the best possible response to growth hormone is the age of the patient when she starts treatment. Results are best when treatment is started early, at approximately 9 months of age. Patients who receive treatment early exhibit better results in terms of final height 10,14-16. Studies that have assessed the long-term impact of HGH treatment show that patients have normal health status 17,18. In this case, the patient began hormonal replacement therapy at around the age of eight and, although it was started late, this treatment achieved a significant improvement in the patient's skeletal growth. If the therapy had been started earlier, the patient could possibly have exhibited even better results.
Only 10 to 12% of girls with TS secrete enough hormones to provoke spontaneous sexual development. Therefore, at the right time, replacement of estrogen to induce puberty is recommended for the majority of patients 19. Estrogen replacement therapy reduces the biological response to growth hormone, which is why the start of this therapy should be correctly timed in order to avoid drug interactions 20,21. Estrogen therapy is usually started when the girl is between 12 and 13 years old. The objective of treatment is development of secondary sexual characteristics and increase and maintenance of bone mass. Patients who do not receive replacement of these hormones may suffer from osteoporotic fractures 17,22. In this patient's case, orthodontic treatment was concluded without the need for sexual hormone replacement, which may have contributed to the positive skeletal growth results achieved with orthopedic treatment. Nevertheless, endocrinological follow-up is a constant necessity, since a hormone insufficiency may arise at any point during the course of the patient's life.
There are no reports in the current literature of cases in which growth hormone has affected dental development and its influence is restricted to skeletal development 14.
Dental morphology studies show that the teeth of patients with TS exhibit reduced vestibule-palatal and mesiodistal dimensions. Incisors may display cervico-incisal convergence of proximal surfaces and have sharp edges, while canines can have sharp lingual cusps of regular size. Moreover, there are often atypical cusps and enamel tubercles on premolars and molars 23,24. Not all of these characteristics were observed in the case described here. Only the modified morphology of maxillary incisors was seen, with the typical cervico-incisal convergence of proximal surfaces. Nonetheless, the skeletal pattern was as described in several reports found in the literature.
Enamel hypoplasia is frequently observed in TS patients. This can be defined as an abnormality of the structure of the teeth causing quantitative and qualitative defects in which incomplete formation of the organic matrix of the teeth is the result of damage to ameloblasts (enamel-forming cells). In some of the cases reported in the literature there was total or partial absence of enamel, which was related to genetic influences on dental formation 24-26. In this clinical case, the patient exhibited hypoplasia, particularly of maxillary teeth, although this abnormality was not particularly severe.
There are reports of cases of hyperplastic gingivitis, periodontal pockets, and dental mobility among adult patients 27. Gingival problems may be affected by hormone treatment, because an increase in systemic sexual hormones combined with dental plaque may result in periodontal diseases. This increase in levels of sexual hormones has been related to a strong gingival response to inflammation, causing abnormal capillary permeability and greater accumulation of fluid in gingival tissues, which results in edema, bleeding, and gingivitis when combined with dental plaque. Bleeding may occur during brushing and mastication 28. Due to such factors, the patient was encouraged to develop good oral hygiene habits, which were regularly supervised during monthly consultations, in order to avoid complications such as those described. Regular preventive maintenance should go beyond orthodontic follow-up, since both should happen simultaneously to prevent complications and promote oral health.
It is imperative that girls and women with TS be treated by a multidisciplinary team that, in addition to the dental surgeon, includes a cardiologist, an endocrinologist, a geneticist and a professional to provide psychotherapeutic guidance 29.
The abnormalities of the buccal cavity that manifest with TS mean that the dental surgeon is one of the professionals whose work can improve TS patients' quality of life. These patients require dental follow-up throughout their entire lives.
FINAL CONSIDERATIONS
The dental surgeon is one of the professionals whose work can improve the quality of life of patients with TS. Orthodontic and pediatric dental follow-up is fundamental to anticipate, prevent, and treat the most common oral complications. It can be concluded that when treated early by a multidisciplinary team, patients with TS may be able to live free from further complications and enjoy good quality of life.
REFERENCES
1. Lopez ME, Bazan C, Lorca IA, Chervonagura A. Oral and clinical characteristics of a group of patients with Turner syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:196-204. [ Links ]
2. Batch J. Turner syndrome in childhood and adolescence. Best Pract Res Clin Endocrinol Metab. 2002;16:465-82.
3. Stochholm K, Juul S, Juel K, Naeraa RW, Gravholt CH. Prevalence, incidence, diagnostic delay and mortality in Turner Syndrome. J Clin Endocrinol Metab. 2006;91:3897-902.
4. Gravholt CH, Naeraa RW. Reference values for body proportions and body composition in adult women with Ullrich-Turner syndrome. Am J Med Genet. 1997;72:403-8.
5. Kusiak A, Sadlak NJ, Limon J, Kochanska B. Root morphology of mandibular premolars in 40 patients with Turner syndrome. Int Endod J. 2005;38:822-6.
6. Dumancic J, Kaic Z, Varga ML, Lauc T, Dumic M, Milosevic SA, et al. Characteristics of the craniofacial complex in Turner syndrome. Arch Oral Biol. 2010;55:81-8.
7. Rusell KA. Orthodontic treatment for patients with Turner syndrome. Am J Orthod Dentofacial Orthop. 2001;120:314-22.
8. Egias SM. La mujer adulta con síndrome de Turner. In: 9º Curso de Formación de Posgrado; 2003; Zaragoza, España.
9. Davenport ML, Crowe BJ, Travers SH, Rubin K, Ross JL, Fechner PY, et al. Growth hormone treatment of early growth failure in toddlers with Turner syndrome: a randomized, controlled, multicenter trial. J Clin Endocrinol Metab. 2007;92:3406-1.
10. Soriano-Guillen L, Coste J, Ecosse E, Léger J, Tauber M, Cabrol S, et al. Adult height and pubertal growth in Turner syndrome after treatment with recombinant growth hormone. J Clin Endocrinol Metab. 2005;90:5197-204.
11. Thiesen G, Rego MVNN, Lima EMS. Estudo longitudinal da relação entre o crescimento mandibular e o crescimento estatural em indivíduos com Classe II esquelética. Rev Dent Press Ortodon Ortop Facial. 2004;9:28-40.
12. Chernausek SD, Attie KM, Cara JF, Rosenfeld RG, Frane J. Growth hormone therapy of Turner syndrome: the impact of age of estrogen replacement on final height. J Clin Endocrinol Metab. 2000;85:2439-45.
13. Saenger P. Transition in Turner's syndrome. Growth Horm IGF Res. 2004;14:72-6.
14. Perkiomaki MR, Kyrkanides S, Niinimaa A, Alvesalo L. The relationship of distinct craniofacial features between Turner syndrome females and their parents. Eur J Orthod. 2005;27:48-52.
15. Rosenfeld RG, Attie KM, Frane J, Brasel JA, Burstein S, Cara JF, et al. Growth hormone therapy of Turner's syndrome: beneficial effect on adult height. J Pediatr. 1998;132:319-24.
16. Guedes AD, Bianco B, Callou EQ, Gomes AL, Lipay MVN, Verreschi ITN. O hormônio de crescimento na síndrome de Turner: dados e reflexões. Arq Bras Endrocrinol Metab. 2008;52:757-64.
17. Sas TC, de Muinck SMK, Stijnen T, van Teunenbroek A, van Leeuwen WJ, AsarfiA, et al. Bone mineral density assessed by phalangeal radiographic absorptiometry before and during long-term growth hormone treatment in girls with Turner's syndrome participating in a randomized dose-response study. Pediatr Res. 2001;50:417:22.
18. Goodman LS, Gilman A. As bases farmacológicas da terapêutica. 11ª ed. Rio de Janeiro: MacGraw-Hill; 2006. p. 1344-52.
19. Piippos S, Lenko H, Kainulainen P, Sipila I. Use of percutaneous estrogen gel for induction of puberty in girls with Turner Syndrome. J Clin Endocrinol Metab. 2004;89:3241-7.
20. Silverman BL, Friedlander JR. Is growth hormone good for the heart? J Pediatr. 1997;131:70-4.
21. Anderson-Wallgren G, Ohlsson AC, Albertsson-Wikland K. Growth promoting treatment normalizes speech frequency in Turner syndrome. Laryngoscope. 2008;118:1125-30.
22. Kiess W, Kratzch J, Pfaeffle R. The growth hormone (GH) and insulin-like growth factor (IGF) system in girls and women with Turner syndrome. Int Congr Ser. 2006;1298:63-70.
23. Hass AD, Simmons KE, Devenport ML, Proffit WR. The effect of growth hormone on craniofacial growth and dental maturation in Turner syndrome. Angle Orthod. 2001;71:50-9.
24. Golçalvez AF, Ferreiras LM. Defeitos hipoplásicos do esmalte dentário (revisão literatura). Revis Odontol Univ Santo Amaro. 2000;5:13-20.
25. Medina AAJ, Moro NRL. Amelogênese imperfeita, suas implicações, relato de caso clínico. J Bras Ortodon Ortop Facial. 2001;31:21-4.
26. Oliveira AFB, Rosenblatt A. Defeitos do esmalte. Rev ABO Nac. 2002;10:274-7.
27. Selow MLC, Vieira I, Figueiredo AM, Miyaki A. Síndrome de Turner e a odontologia. Rev Dens. 2006;14:13-20.
28. Stamm JW. Epidemiology of gingivitis. J Clin Periodontol. 1986;13:360-70. 29. Suzigan LZC, Silva RBP, Maciel-Guerra AT. Aspectos psicossociais da síndrome de Turner. Arq Bras Endocrinol Metabol. 2005;49:157-64.
 Correspondence:
Correspondence:
Guilherme Thiesen
Av. Madre Benvenuta, 1285, Santa Mônica
Florianópolis, SC, Brasil
e-mail: thiesen.guilherme@gmail.com
