










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.41 Canoas Jul./Dez. 2015
An unusual presentation of oral mucocele in a young pediatric patient
Uma apresentação incomum de mucocele oral em paciente pediátrico jovem
Simone Helena Ferreira I; Daiane Fin II; Paulo Floriani Kramer III; Mariana Cezar Ilha IV; Tássia Silvana BorgesV; Henrique Castilhos Ruschel III
I MSc in Public Health from and associate professor at School of Dentistry, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II DDS from School of Dentistry, ULBRA, Canoas, RS, Brazil
III Pediatric Dentistry from Universidade de São Paulo (USP), São Paulo, SP, Brazil, and associate professors at School of Dentistry, ULBRA, Canoas, RS, Brazil
IV MSc candidate in Pediatric Dentistry at School of Dentistry, ULBRA, Canoas, RS, Brazil
V MSc in Health Promotion from Universidade de Santa Cruz do Sul (UNISC), Santa Cruz do Sul, RS, Brazil, and PhD candidate in Pediatric Dentistry at School of Dentistry, ULBRA, Canoas, RS, Brazil
The authors have no conflicts of interest to declare concerning the publication of this manuscript
ABSTRACT
Mucocele is a common condition of the minor salivary glands that is generally found on the lower lip. Although etiology is uncertain, mucocele are usually caused by local trauma. Cases involving infants are rarely reported in the literature. The objective of this study is to report an unusual case of mucocele in the first year of life that was treated with surgical removal and postoperative follow-up. This report illustrates the main features of clinical interest and discuss classification, differential diagnosis and the treatment approaches described in the literature.
Keywords: Child; Pediatric Dentistry; Mucocele; Oral Mucosa.
RESUMO
Mucocele é uma alteração comum de glândulas salivares menores que acomete principalmente o lábio inferior. Embora a etiologia seja incerta, normalmente é causada por um trauma local. Casos envolvendo bebês são raramente relatados na literatura. O objetivo deste estudo é descrever um caso não usual de mucocele no primeiro ano de vida. O tratamento foi a remoção cirúrgica da mucocele e acompanhamento pós-operatório. Com o presente relato pretende-se ilustrar os principais aspectos de interesse clínico, discutindo a classificação e o diagnóstico diferencial, além das modalidades terapêuticas descritas na literatura.
Palavras-chave: Criança; Odontopediatria; Mucocele; Mucosa Bucal.
INTRODUCTION
The term mucocele is used to denote the clinical manifestations of two different phenomena that affect the minor salivary glands: mucus extravasation cyst and mucus retention cyst 1-3.
Extravasation of mucus into underlying connective tissue is the result of rupture of an excretory gland of a minor salivary gland, caused by trauma or laceration 4. An inflammatory reaction is induced in adjacent tissues, in which neutrophil and macrophage defense cells predominate, creating granulation tissue surrounding the pooled mucus, isolating the lesion and giving it the appearance of a pseudocyst 5,6. A recurrent characteristic is periodic reduction of the swelling due to rupture and partial release of fluid, soon followed by recurrent build up 5.
In turn, mucus retention cysts result from partial or complete obstruction of the excretory duct and are usually caused by a mucous tampon or a sialolith resulting in retention of glandular secretions and dilation of the duct 4,5. They are less prevalent than extravasation cysts. Retention cysts are more common among elderly patients, while mucoceles caused by mucus extravasation are more common in children and young adults 4-9.
Mucoceles do not exhibit preference for either sex and they can occur at any site in the oral cavity where there are minor salivary glands 5-9. Notwithstanding, the site most commonly affected is the lower lip, lateral of the midline (70-80%) 5. Less frequently, they may also occur in the jugal mucosa, the floor of mouth, the central surface of the tongue, the soft palate, or the upper lip 5.
The clinical appearance of mucoceles is vesicles or blisters full of fluid, circumscribed, fluctuant, and slightly blue or translucent in aspect; they also exhibit slow growth, and are asymptomatic 5-7. Differential diagnosis is important because mucoceles resemble other lesions such as focal fibrous hyperplasia, papilloma and lipoma, and even benign neoplasia should be considered 5.
The conventional treatment is surgical removal of the minor salivary gland responsible 10,11. Other treatment alternatives include laser, cryosurgery, and marsupialization 11-15. Prognosis is excellent, although some lesions may relapse depending on the treatment approach chosen.
This paper describes a clinical case of mucocele in a baby, emphasizing aspects related to diagnosis and treatment of the condition.
CASE REPORT
A ten-month-old, white-skinned, female patient was referred to the Pediatric Dental Clinic of the School of Dentistry at ULBRA-RS. According to the mother, they had sought medical attention because there was a "blister" on the inner part of the lower lip, which caused the child discomfort and occasionally grew in size.
During history-taking, the mother reported that when she was pregnant an ultrasonography had shown an image suggestive of the fetus sucking the back of its left hand. At the time of birth the child had a lesion on the inner part of the lower lip and ulceration on the back of the left hand with exposed connective tissue.
At the pediatric dental consultation, the mother reported using bottles and that the child had non-nutritional sucking habits with pacifiers. Extraoral physical examination revealed an area on the back of the patient's left hand with reduced pigmentation. According to the mother, this coincided with the area where the lesion had been observed at birth (Figure 1).

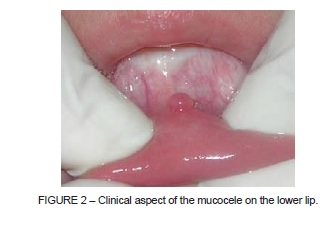
A lesion was observed during the intraoral examination on the inner part of the lower lip, in the midline area, that was exophytic, bullous, circumscribed, pinkish, and of soft consistency on palpation. This lesion was approximately five millimeters in diameter (Figure 2). Given these findings, the presumptive diagnosis was mucocele.
The treatment chosen was complete surgical removal of the lesion. Surgery was performed under local anesthesia. The procedure was initiated by administration of topical anesthesia (xylocaine 5%) to the area, followed by infiltration anesthesia (lidocaine 2%) next to the base of the lesion (Figure 3A). The lesion was clamped with the aid of mosquito forceps and the mucocele was enucleated with an incision at the base encompassing the minor glands involved (Figure 3B). The wound was sutured using absorbable thread and simple interrupted stitches (Figure 3C). Analgesic medication was prescribed and advice was given regarding postoperative care. The excised material was sent for histopathological analysis. Two fragments of soft tissue were collected, with round shape, firm consistency, pinkish color, smooth appearance, sessile base, and well-defined borders (Figure 3D).

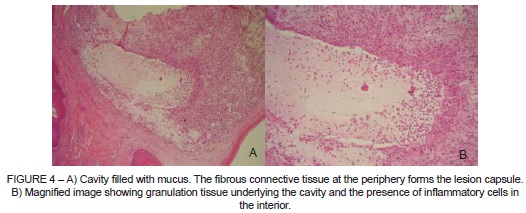
The histopathological examination confirmed the presumptive diagnosis of mucocele caused by mucus extravasation. The laboratory report described the lesion as a cavity containing mucus; with underlying granulation tissue and surrounded by a fibrous capsule. Areas of suppuration and fragments of oral mucosa epithelium were also observed (Figures 4A and 4B).
A postoperative evaluation was conducted after 14 days to verify the healing process of the lesion (Figure 5). After a six-month period, the patient returned for another evaluation. Eruption of the mandibular incisors was observed during intraoral examination. There were no signs of recurrence of the lesion.

DISCUSSION
Mucoceles are lesions involving minor salivary glands. There is consensus that the lower lip is the site of highest occurrence, because it is the area most susceptible to trauma 7-9,15,16. Mucoceles may be located superficially on the mucosa, presenting as a vesicle or blister full of fluid with a bluish color, or they may be located deep in the connective tissue, in the form of a fluctuant nodule covered by regular-colored mucosa 15.
In this clinical case, a mucocele was diagnosed in the lower lip of a ten-month-old infant. According to the mother, a lesion had already existed at birth. An ultrasonography examination conducted as part of prenatal care had been suggestive of sucking of the back of the hand and the presence of ulceration of the corresponding area after birth raised the possibility that breakage of glandular excretory ducts of the lower lip was a traumatic etiologic factor.
Abreu et al. 9 also reported presence of mucocele on the lower lip of an eightmonth- old baby. According to the parent, the child had had the lesion since birth. Since the lesion interfered with breastfeeding, the option was for surgical removal. Histopathological examination also identified an extravasation mucocele.
Crivellaro et al. 16 reported a case of mucocele in a two-year-old child. A lesion appeared after a fall in which the child traumatized the area. The lesion was located on the lower lip; it presented a bullous and circumscribed appearance, smooth surface and pinkish color. Surgical treatment of the lesion was performed and histopathological examination confirmed the diagnosis of extravasation mucocele.
With respect to treatment, the literature recommends complete surgical excision of the lesion together with the glandular component in order to prevent recurrence 7. Alternative treatment options depend on the age of the patient, general characteristics of the lesion (location, size, and depth), type of trauma, and emotional status of the patient 15. There are reports of cryotherapy techniques, marsupialization, surgical excision using Shira's technique, and treatment with argon laser 10-17.
Three different cryogenic agents can be used for cryotherapy: liquid nitrogen, carbon dioxide or nitrous oxide. The most commonly used is liquid nitrogen because it is more versatile and it is dry. The advantage of this technique is that it is well accepted by patients, since it does not require infiltration anesthesia or any other sedative agent, administration is easy, and it can be used in small children, reducing discomfort during the procedure. It can be applied directly or indirectly over the lesion. The lesion tends to disappear after the initial applications, and no recurrences were reported after follow-up periods of six months to five years 17,18.
Marsupialization superficially removes the mucosa covering the lesion and sutures the salivary duct epithelium to the oral epithelium. The purpose of the procedure is to maintain drainage and avoid scarring of the edges. It is more frequently indicated for cases of ranulas and it has a high recurrence rate, so it is not the recommended treatment for children 17,18. Another treatment is known as Shira's Technique, which consists of injecting casting material inside the lesion beforehand to prevent mucus extravasation at the moment of separation 17,18. Argon lasers can also be used to cause necrosis of the mucocele. The advantage of this technique over cryosurgery is reduced discomfort for the patient, less edema, and faster healing. On the other hand, it demands special equipment and it is expensive 17,18.
In the case reported here, surgical removal enabled complete healing of the area without recurrence of the lesion. It is relevant to mention the importance of early diagnosis to differentiate mucocele from other pathologies, to reduce parents' concerns and the child's discomfort.
FINAL REMARKS
Mucolece is a benign condition, commonly found in children, which may cause patients discomfort and their parents concern. Therefore, the professional must be capable of correctly identifying the lesion, making early differential diagnosis and providing immediate care in accordance to the best scientific evidence.
REFERENCES
1. Largura LZ, Grando LJ, Raul LH, Gil JN. Remoção cirúrgica de mucocele. Rev Assoc Paul Cir Dent. 1998;52:435-8. [ Links ]
2. Bentley JM, Barankin B, Guenther LC. A review of common pediatric lip lesions: herpes simplex/recurrent herpes labialis, impetigo, mucoceles, and hemangiomas. Clin Pediatr. 2003;42:457-82.
3. Baurmash HD. Mucoceles and ranulas. J Oral Maxillofac Surg. 2003;61:369-78.
4. Porter SR, Scully C, Kainth B, Ward-Booth P. Multiple salivary mucoceles in a young boy. Int J Paediatr Dent. 1998;8:149-51.
5. Laskaris, G. Atlas colorido de doenças bucais da infância e adolescência. São Paulo: Santos; 2000.
6. Silva A Jr, Nikitakis NG, Balciunas BA. Superficial mucocele of the labial mucosa: a case report and review of the literature. Gen Dent. 2004;52:427-8.
7. Regezi AJ, Ciubba JJ, Jordan RCK. Patologia oral: correlações clinicopatológicas. Rio de Janeiro: Elsevier; 2008.
8. Bermejo A, Aguirre JM, López P, Saez MR. Superficial mucocele: report of 4 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:469-72.
9. Abreu KCS, Glavez A, Carmen DP, Blessmann WJB, Silva SMB. Mucocele em bebê: relato de um caso clínico. Rev Fac Odontol Lins. 1998;11:42-5.
10. Twetman S, Isaksson S. Cryosurgical treatment of mucocele in children. Am J Dent. 1990;3:176-7.
11. Wu CW, Kao YH, Chen CM, Hsu HJ, Chen CM, et al. Mucoceles of the oral cavity in pediatric patients. Kaohsiung J Med Sci. 2011;27:276-9.
12. Kopp WK, St-Hilaire H. Mucosal preservation in the treatment of mucocele with CO2 laser. J Oral Maxillofac Surg. 2004;62:1559-61.
13. Fernandes AMM, Morosolli ARC, Farias LP, Niccoli-Filho W. Estudo clínico e comparativo entre cirurgia convencional e a radiação laser de CO2 em fenômeno de retenção de muco. Cienc Odontol Bras. 2006;9:54-61.
14. Bhargava N, Agarwal P, Sharma N, Agrawal M, Sidiq M, Narain P. An unusual presentation of oral mucocele in infant and its review. Case Rep Dent. 2014: 723130. http://dx.doi.org/10.1155/2014/723130
15. Câmara LP, Menezes VA, Neves HLS, Santos VIM. Mucocele: relato de caso clínico. J Bras Odontopedriatr Odontol Bebe. 2002;5:378-81.
16. Crivellaro JS, Ferreira SH, Pinto TAS, Ruschel HC. Mucocele labial: relato de caso em criança de 2 anos de idade. Stomatos. 2007;13:30-6.
17. Stuani AS, Stuani ASI, Silva FWGP, Stuani MBS, Valério RA, Queiroz AM. Mucoceles: lesões frequentes na cavidade bucal de crianças. Pediatria. 2010;32:288-92.
18. Santos TS, Martins Filho PRS, Menezes FS, Maia MC, Carvalho RWF, Araújo FAC. Tratamento cirúrgico de mucocele utilizando a técnica de Shira: relato de caso. UFES Rev Odontol. 2008;10:53-8.
 Correspondence:
Correspondence:
Tássia Silvana Borges
Rua Joana Machado, 103/302, Camobi
CEP 97105-180, Santa Maria
RS, Brazil
e-mail: tassia.s.borges@hotmail.com
