










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.1 Piracicaba Jan./Mar. 2012
ORIGINAL ARTICLE
Evaluation of proximal enamel thickness and crown measurements in maxillary first premolars
Leni Okamoto MunhozI; Flávio Vellini-FerreiraII; Flávio Augusto Cotrim-FerreiraIII; Rívea Inês FerreiraIII
IMSc in Orthodontics, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), Brazil
IIPhD, Professor and Chairman, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), Brazil
IIIPhD, Associate Professor, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), Brazil
ABSTRACT
Estimating enamel thickness and planning the resultant optimal morphology of premolars are substantial steps before interproximal stripping.
AIM: To analyze proximal enamel thickness and crown measurements in maxillary premolars.
METHODS: The mesiodistal, buccolingual and cervico-occlusal measurements of 40 human maxillary first premolars (20 right, 20 left) were registered with a digital caliper. The teeth were embedded in acrylic resin and sectioned mesiodistally at the level of the contact areas to obtain 1 mm-thick central sections. Enamel thickness on the proximal surfaces was measured using a perfilometer. Measurements were compared by the Student's t-test (α = 0.05).
RESULTS: The mean enamel thickness on the mesial surface was 1.22 mm for the right (± 0.17) and left (± 0.18) sides. On the distal surface, the corresponding values were 1.28 mm (± 0.19) on the right side and 1.39 mm (± 0.17) on the left side. Mean values, in millimeters, for the mesiodistal, buccolingual and cervico-occlusal measurements on both sides ranged from 7.03 (± 0.43) to 7.07 (± 0.48), 9.59 (± 0.48) to 9.65 (± 0.58) and 8.65 (± 0.66) to 8.85 (± 0.65), respectively. There were no significant differences between right and left teeth. However, enamel thickness was significantly greater (p<0.05) on the distal surface.
CONCLUSIONS: In maxillary first premolars, considering the greater thickness of distal enamel, interproximal stripping during orthodontic treatment may be more pronounced on this surface. The greatest mean value was observed for the buccolingual crown measurement, followed by the cervicoocclusal and mesiodistal dimensions.
Keywords: bicuspid, tooth crown, dental enamel, orthodontics.
Introduction
Currently, orthodontic patients are searching for esthetics combined to satisfactory functioning of the stomatognathic system in the dental offices. Treatments comprising tooth extraction and appliances that cause discomfort and social constraint are avoided and effectively overcome, for example, by interproximal stripping. Good occlusion and normal periodontal conditions, with intact gingival papillae between all teeth in the maxillary and mandibular arches, could be observed in follow-up examinations more than 3.5 years after orthodontic treatment1. Some authors2 mention that enamel reduction in premolars using rotary instruments and appropriate technique does not damage dental pulp in most cases, even if dentin is slightly exposed and polished. The use of fluoride after enamel stripping was indicated and patients did not complain of any symptoms.
Interproximal enamel stripping yields an alternative method to tooth extraction for solving mild to moderate crowding and has also been associated to short treatment duration1-6. Moreover, interproximal enamel stripping is not only useful for correcting tooth-arch discrepancies, but it also increases treatment stability7-9, and keeps the transverse dental arch dimensions and anterior inclinations constant1,6,10.
Although some authors mentioned that about fifty percent of proximal enamel can be safely removed11-12, all professionals who are willing to perform the striping procedure should be aware of the estimates relative to the proximal enamel thickness and crown measurements for avoiding damaging to the dental structures and achieving proper tooth recontouring. Thus, the aim of this experimental investigation was to accurately assess the mean values of the proximal enamel thickness, as well as the mesiodistal, cervico-occlusal and buccolingual crown measurements, in maxillary first premolars. The null hypotheses stated no differences between enamel thicknesses according to the side of the dental arch and proximal surface.
Material and methods
This experimental study was approved by the Institutional Review Board, under the protocol number 13260742/2007, and complies with the Brazilian resolution regulating research involving humans (Resolution 196/96).
Sample
Forty sound human maxillary first premolars (20 right and 20 left) were selected from two tooth banks. All donors were Brazilians, yet information on the gender, age and race was unavailable. Teeth were separated into two groups (right and left sides) and randomly numbered from 1 to 20.
Achievement of crown measurements
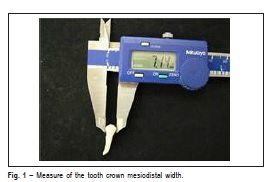
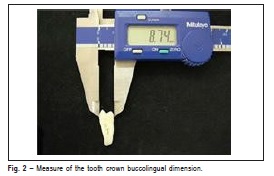
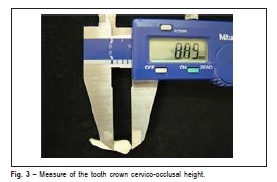
Mesiodistal (Figure 1), buccolingual (Figure 2) and cervico-occlusal (Figure 3) measurements were obtained with a digital caliper (Mitutoyo® Sul Americana Ltda., Suzano, SP, Brazil) accurate to 0.01 mm, by a well-trained examiner. The mesiodistal measurement was assumed as the distance from the most central point in the contact area on the distal surface to its counterpart on the mesial surface. The values obtained from the midpoint on the buccal surface to the midpoint on the lingual surface of crowns were registered as the buccolingual measurement. The distance between the occlusal edge of the buccal surface and the cementoenamel or dentinoenamel junction at the cervical region of the tooth corresponded to the cervico-occlusal measurement.
Enamel thickness assessment
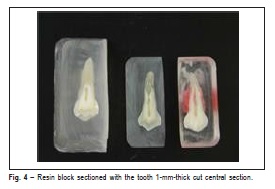
All teeth were kept in a fixed position in rectangular plastic flasks using utility wax and embedded in acrylic resin (ARAZYN 1.0 – Redelease®, São Paulo, SP, Brazil). Tooth sections were obtained using a diamond disc in a trimmer Lab Cut® 1010 (Extec® Corp., Enfield, CT, USA), undercooling to avoid specimen fracture. The mean speed of the disc was maintained at 350 rpm. The specimens were sectioned longitudinally through the proximal surfaces, parallel to the buccal surface, producing 1-mm-thick central sections (Figure 4). Each section corresponded to the most central part of the crown, on the proximal surfaces, because it encompassed the greatest mesiodistal dimension and, hence, the area where the proximal enamel is thicker.
Based on previous research13, the sections were placed in a perfilometer (Mitutoyo®, Profile Projector® PJ 300, Kawasaki, Japan) accurate to 0.001 mm, so as the tooth long axis coincided with the Cartesian axes of the device (X and Y), which were displaced in horizontal and vertical directions, respectively (Figure 5). Proximal enamel thickness was measured by displacement of the Cartesian axis in mesial and distal directions of the tooth section. Considering that the measurements were obtained on the projected images of the cut sections, all dimensions were measured three or six times until the values coincided three times.
Statistical analyses
Mean (and the standard deviation), minimum and maximum values and the coefficient of variation were calculated for the enamel thickness on the mesial and distal surfaces, as well as the mesiodistal, buccolingual and cervicoocclusal measurements. Comparisons between mean values registered for the right and left teeth, and enamel thickness on the mesial and distal surfaces were carried out using the Student's t-test (α = 0.05).

Results
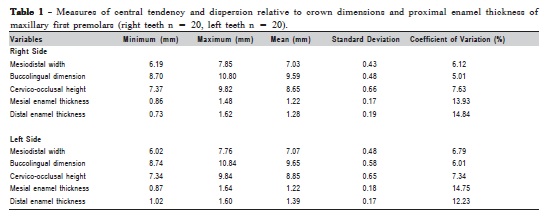
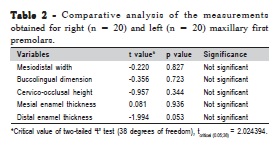
Minimum, maximum and mean values, as well as standard deviations and coefficients of variation for the crown measurements and enamel thicknesses of maxillary first premolars are shown in Table 1. The greatest mean value was observed for the buccolingual crown measurement, followed by the cervico-occlusal and mesiodistal dimensions. Mean enamel thickness on the mesial surface was 1.22 mm on the right (± 0.17) and left (± 0.18) sides. On the distal surface, the corresponding values were 1.28 mm (± 0.19) on the right side and 1.39 mm (± 0.17) on the left side (Table 1). However, there were no statistically significant differences (p>0.05) between measurements obtained for right and left teeth (Table 2).
Based on the coefficients of variation, there was marked variability of data in relation to the means for enamel thicknesses on the mesial (13.93% to 14.75%) and distal (12.23% to 14.84%) surfaces of both sides (Table 1). Conversely, data obtained for the mesiodistal, buccolingual and cervico-occlusal measurements demonstrated homogeneity, since the coefficients of variation were lower than 10%. Although the coefficients of variation for proximal enamel thicknesses were higher in comparison to the values obtained for crown measurements, these indices may still be considered relatively low.
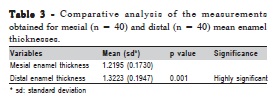
Because no significant differences between mean enamel thicknesses on the mesial and distal surfaces of right and left maxillary first premolars were found, the measurements for both sides were considered for comparison in Table 3. The resultant mean value of enamel thickness was significantly higher on the distal surfaces compared to the mesial surfaces of maxillary first premolars.
Discussion
The analyses of tooth crown measurements and proximal enamel thickness is actually useful to establish the diagnosis and adequate orthodontic treatment planning, specifically concerning the decision between tooth extraction and interproximal enamel stripping. The latter treatment modality may avoid extractions, decrease treatment time and provide more favorable outcomes3-6. In addition, the orthodontist should take into account that many patients may not be willing to undergo tooth extractions14.
Interproximal enamel stripping may be a suitable treatment alternative to solve mild to moderate tooth crowding1,3,5,9. Accordingly, this therapeutic option may be used in tooth-size discrepancies occurring in Class I malocclusions, Class II malocclusions with mild deviations in cephalometric measurements, especially after the growth period, and Bolton discrepancy14, in which the teeth sizes are greater than the space available in the dental arch. Around 8.9 mm of space may be gained in the dental arches using interproximal enamel stripping techniques, which may also be applied in posterior teeth15. However, the amount of enamel to be removed should be estimated according to the severity of tooth-size discrepancy5,11,16. Enamel reduction may be substantial on teeth with deviating morphology, while incisors with parallel proximal surfaces, screwdriver-shaped teeth and rotated premolars may not be eligible for any stripping1.
Concerning the crown measurements of maxillary first premolars (Table 1), the smallest mean values were observed for the mesiodistal width (7.03 – 7.07 mm). Another Brazilian study recorded slightly greater values (7.51 – 7.53 mm)9. Presumably, this variation may be attributed to methodological differences between studies. In the present experimental research, all measurements were taken directly on the teeth using a digital caliper accurate to 0.01 mm, while the other authors obtained the measurements on images of histological sections of teeth projected on a computer monitor screen. Digital images were acquired by a coupled camera and the operator used the software tools for measuring crown width9. This procedure may cause some image magnification, though increasing mesiodistal crown measurement. The greatest mean value was observed for the buccolingual crown dimension (9.59 – 9.65 mm). Interestingly, the cervico-occlusal height presented greater values of standard deviation and coefficient of variation, maybe because the crown heights in some teeth were reduced by occlusal wear (Table 1).
The direct register of crown measurements in the mouth using a caliper revealed that the teeth had smaller mesiodistal and greater buccolingual dimensions17. This finding corroborates the results shown in Table 1. In another study5, an index was designed to evaluate morphological deviations of teeth, adding knowledge for better understanding mandibular incisors crowding. The sample was composed of White young adult females divided into two groups: one group with satisfactory alignment of mandibular incisors and the second group of patients with diagnosis of tooth crowding, which was taken as the control group. Measurements were also obtained directly on the patient's mouth, using a caliper with Venier scale. Comparison of the mesiodistal and buccolingual dimensions of the same tooth revealed that the former was smaller than the latter measurement in the second group5.
Conventional and digital intraoral radiographs, as well as computed tomography, are considered proper diagnostic adjuncts for clinical assessments of tooth crown and proximal enamel measurements18-19. Nevertheless, one disadvantage of computed tomography is the blurred image on the limits of enamel thickness smaller than 1.1 mm, which precludes determination of the point from which the measurements should be initiated, despite the high image resolution19. This study presented data on the proximal enamel thickness of maxillary first premolars (Table 1). Mesial (1.22 mm for both sides) and distal (varying from 1.28 mm on the right side to 1.39 mm on the left side) mean values of enamel thickness indicated a possible difference according to the proximal surface. As shown in Table 3, the proximal enamel wassignificantly thicker on the distal surface in comparison to the mesial surface (p = 0.001). This finding agrees with a Brazilian study in which measurements were similarly obtained on human maxillary first premolars, yet using a different methodology9. The authors observed mean values of mesial enamel thickness of 1.08 mm (right side) and 1.19 mm (left side) and distal enamel thickness of 1.29 mm (both sides). A recent study also reported the significantly higher enamel thickness on the distal surface in second mandibular premolars, compared to the mesial surface13. It is worth mentioning that some studies suggest limits for proximal enamel stripping of 0.4-0.5 mm, regardless of the surface6-7,10.
Tooth banks do not provide information on the age range, gender or race of the donors. However, since this sample included only sound human premolars, it may be assumed that these teeth were donated by adolescents or young adults. Even though mastication also influences the reduction of proximal enamel, its greater effect occurs on occlusal wear. Moreover, considering that people have adopted a predominantly semi-solid diet since the past century, a significant loss of proximal enamel due to mastication forces is more frequent in elderly individuals20-22. With regard to gender dimorphism, a study revealed that the mesiodistal dimensions of the tooth crown for males were greater compared to the measurements obtained in females23. Some authors evaluated the mesiodistal and buccolingual dimensions of tooth crowns in North Americans, Egyptians and Mexicans24. All these populations exhibited significant difference between measurements in males and females24, which confirmed the findings of that previous study23. Males presented greater canines and first molars24. A plausible explanation for the gender dimorphism may be related to the fact that the dentin thickness seems to be greater in males10,18. Thus, the greater mesiodistal crown measurement in males may probably be a consequence of the thicker dentin layer under the tooth enamel.
In the present study, the mesiodistal, buccolingual and cervico-occlusal crown measurements, as well as the proximal enamel thickness, were evaluated irrespective of the gender. Furthermore, the maxillary first premolars selected were donated by patients who underwent a certain degree of the so-called miscegenation. However, for all measurements obtained, there was no statistically significant difference between right and left teeth (Table 2), demonstrating symmetry in crown morphology and proximal enamel thickness of the maxillary first premolars.
Radiography and computed tomography, specifically cone-beam computed tomography, can be used in the clinical practice to estimate the amount of proximal enamel that may be safely removed, considering each patient individually9. Nonetheless, it would also be clinically relevant to perform experimental studies for assessing crown measurements and proximal enamel thickness, since these values may be taken as parameters during interproximal stripping. In the present study, distal enamel was significantly thicker compared to the mesial enamel. Hence, it is suggested that greater interproximal stripping may be performed on the distal surface. After interproximal stripping, the use of accurate measuring devices is advocated to estimate the magnitude of enamel reduction25. As a contribution to orthodontists, this study demonstrated that, in maxillary first premolars, the buccolingual measurement presented the highest mean value, followed by the cervico-occlusal and mesiodistal dimensions, even though the difference between the mean values related to these measurements were lower than 2 mm.
Acknowledgments
The authors are especially thankful to Professor Washington Steagal Junior from the Restorative Dentistry Department of the University of São Paulo (FOUSP) for his dedication and collaboration in the statistical analyses of this study.
References
1. Zachrisson BU, Minster L, Ogaard B, Birkhed D. Dental health assessed after interproximal enamel reduction: caries risk in posterior teeth. Am J Orthod Dentofacial Orthop. 2011; 139: 90-8. [ Links ]
2. Zachrisson BU, Mjör IA. Remodeling of teeth by grinding. Am J Orthod. 1975; 68: 545-53. [ Links ]
3. Ballard ML. Asymmetry in tooth size: a factor in the etiology, diagnosis and treatment of malocclusion. Angle Orthod. 1944; 14: 67-70. [ Links ]
4. Neff CW. Tailored occlusion with the anterior coefficient. Am J Orthod. 1949; 35: 309-13. [ Links ]
5. Peck H, Peck S. An index for assessing tooth shape deviations as applied to the mandibular incisors. Am J Orthod. 1972; 61: 384-401. [ Links ]
6. Germeç D, Taner TU. Effects of extraction and nonextraction therapy with air-rotor stripping on facial esthetics in postadolescent borderline patients. Am J Orthod Dentofacial Orthop. 2008; 133: 539-49. [ Links ]
7. Rossouw PE, Tortorella A. Enamel reduction procedures in orthodontic treatment. J Can Dent Assoc. 2003; 69: 378-83. [ Links ]
8. Zachrisson BU, Nyoygaard L, Mobarak K. Dental health assessed more than 10 years after interproximal enamel reduction of mandibular anterior teeth. Am J Orthod Dentofacial Orthop. 2007; 131: 162-9. [ Links ]
9. Macha AC, Vellini-Ferreira F, Scavone-Junior H, Ferreira RI. Mesiodistal width and proximal enamel thickness of maxillary first bicuspids. Braz Oral Res. 2010; 24: 58-63. [ Links ]
10. Stroud JL, Buschang PH, Goaz PW. Sexual dimorphism in mesiodistal dentin and enamel thickness. Dentomaxillofac Radiol.1994; 23: 169-71. [ Links ]
11. Demange C, François B. Measuring and charting interproximal enamel removal. J Clin Orthod. 1990; 24: 408-12. [ Links ]
12. Jarjoura K, Gagnon G, Nieberg L. Caries risk after interproximal enamel reduction. Am J Orthod Dentofacial Orthop. 2006; 130: 26-30. [ Links ]
13. Fernandes SA, Vellini-Ferreira F, Scavone-Junior H, Ferreira RI. Crown dimensions and proximal enamel thickness of mandibular second bicuspids. Braz Oral Res. 2011; 25: 324-30. [ Links ]
14. Stroud JL, English J, Buschang PH. Enamel thickness of the posterior dentition: its implications for nonextraction treatment. Angle Orthod. 1998; 68: 141-6. [ Links ]
15. Sheridan JJ. Air rotor stripping. J Clin Orthod. 1985; 19: 43-59. [ Links ]
16. Tuverson DL. Anterior interocclusal relations. Parts I and II. Am J Orthod. 1980; 78: 361-93. [ Links ]
17. Doris JM, Bernard BW, Kuftinec MM, Stom D. A biometric study of tooth size and dental crowding. Am J Orthod. 1981; 79: 326-36. [ Links ]
18. Harris AF, Hicks JD. A radiographic assessment of enamel thickness in human maxillary incisors. Arch Oral Biol. 1998; 43: 825-31. [ Links ]
19. Spoor CF, Zonneveld FW, Macho GA. Linear measurements of cortical bone and dental enamel by computed tomography: applications and problems. Am J Phys Anthropol. 1993; 91: 469-84. [ Links ]
20. Begg PR. Stone age man's dentition. Am J Orthod. 1954; 40: 298-312. [ Links ] 21. Molnar S, Gantt DG. Functional implications of primate enamel thickness. Am J Phys Anthropol. 1977; 46: 447-54. [ Links ]
22. Macho GA, Berner ME. Enamel thickness of human maxillary molars reconsidered. Am J Phys Anthropol. 1993; 92: 189-200. [ Links ]
23. Ghose LJ, Baghdady VS. Analysis of the Iraqi dentition: mesiodistal crown diameters of permanent teeth. J Dent Res. 1979; 58: 1047-54. [ Links ]
24. Bishara SE, Jakobsen JR, Abdallah EM, Fernandez Garcia A. Comparisons of mesiodistal and buccolingual crown dimensions of the permanent teeth in three populations from Egypt, Mexico, and the United States. Am J Orthod Dentofacial Orthop. 1989; 96: 416-22. [ Links ]
25. Chudasama D, Sheridan JJ. Guidelines for contemporary air-rotor stripping. J Clin Orthod. 2007; 41: 315-20. [ Links ]
 Correspondence:
Correspondence:
Rívea Inês Ferreira
Universidade Cidade de São Paulo (UNICID)
Pós-Graduação (Mestrado em Ortodontia)
Rua Cesário Galeno, 448 – Bloco A
CEP 03071-000 – Tatuapé, São Paulo, Brasil
E-mail: riveaines@yahoo.com
Received for publication: September 09, 2011
Accepted: January 24, 2012
