










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.2 Piracicaba Abr./Jun. 2012
ORIGINAL ARTICLE
Clinical reproducibility of a low cost electronic apex locator
Nathalia Vilaça SoaresI; Emmanuel João Nogueira Leal da SilvaII; Claudio Malizzia Alves FerreiraI; Renato Liess KrebsIII; Tauby de Souza Coutinho-FilhoIII
IDDS, Private Practice
IIDDS, MSc, PhD student, Department of Endodontics, University of Campinas, Brazil
IIIDDS, MSc, PhD, Department of Endodontics, State University of Rio de Janeiro, Brazil
ABSTRACT
AIM: To evaluate the clinical reproducibility of three electronic apex locators (EALs), Joypex 5, RomiApex A-15 and Novapex.
METHODS: Twenty-five patients requiring endodontic treatment were selected. Sixty root canals were measured by the three EALs to determine their respective working length, which was defined as a zero reading on the EAL. A new K-file of the same size was used for each measurement. The file length was fixed with a rubber stop and measured with a caliper to an accuracy of 0.1 mm. Data were analyzed statistically using paired t-tests with the Bonferroni correction and Bland-Altman plot to determine the reproducibility of clinical data among the EALs. Significance level was set at 5%.
RESULTS: Mean and standard deviation values measured by the three EALs showed no statistically significant differences. Identical readings by all three EALs were found in 38% of root canals. Fifty percent differed by less than ± 1.0 mm and only 1.3% exceeded a difference of 2.0 mm.
CONCLUSIONS: The clinical reproducibility of the three devices was confirmed with no significant differences among them, indicating that they are effective for clinical use.
Keywords: apex locator, working length, working length determination.
Introduction
The determination and maintenance of the working length (WL) is an important step in root canal treatment, ensuring an efficient chemomechanical preparation and a hermetic seal of the root canal system, both of which are necessary to avoid damage to the periradicular tissues1. Several methods have been proposed for determining the length of the root canal, such the patient's response to pain caused by the passing of the instrument through the apical foramen and the use of conventional or digital radiographs2-3. The advent of electronic apex locators (EALs) provides an additional feature to the endodontic arsenal for determining the correct WL determination.
The latest generation of EALs operates by measuring changes in impedance (alternating current). For this, two or more different frequencies are used and processed using different mathematical algorithms4. Many studies report a high efficacy achieved by new generations of EALs, even in adverse situations like the presence of irrigating solutions, blood, and the existence of large foramens2-5.
With the necessity of effective techniques to locate the root apex, EALs are being widely used and many models have been imported and commercialized in the international market. Recently, various brands of inexpensive EALs were launched in the dental market. Although these EALs have proven accurate in determining the correct WL6, there is little evidence regarding the clinical reproducibility of these devices. Reproducibility indicates whether or not two or more techniques used to measure a given variable, in identical circumstances, produce the same result7. Thus it is reasonable to expect that the WL measured by an EAL should be reproducible by similar EALs in the same root canal under the same clinical conditions.
The aim of this study was to evaluate the reproducibility of the EALs Joypex 5 (Denjoy®, China), RomiApex A-15 (Romidan, Israel) and Novapex (Forum, Israel) under clinical conditions. The null hypothesis is that there is no significant difference in clinical reproducibility between the low cost EAL (Joypex 5) and the other trademarks.
Material and methods
Twenty-five patients from the State University of Rio de Janeiro, including 13 men and 12 women, aged between 18 and 60 years, were selected. Informed consent was obtained from all patients, and the study was conducted in compliance with the ethical principles of the Helsinki Declaration and Good Clinical Practice. Inclusion criteria were pulpal pathosis with or without radiographically confirmed periapical lesions in incisors, canines, premolars, and molars. Teeth with previous endodontic treatment, internal or external root resorption, and/or intracanal calcification were excluded. Patients with active systemic disease and physical or mental disability were also excluded.
Thirty-one teeth were treated including 11 incisors, 7 premolars and 13 molars, totaling 60 root canals. In each case, the diagnosis was based on the patient's history, clinical examination, and radiographs. Local anesthesia was applied in all cases. Access cavities were prepared with a round diamond bur (Dentsply Maillefer, Ballaigues, Switzerland) and refined with a Endo Z bur (Dentsply Maillefer) using a high-speed handpiece. Where necessary, all remaining occlusal cusps were flattened using a high-speed conical diamond bur (Dentsply Maillefer) to achieve a flat reference plane. After verifying the initial patency of the root canal with a size 10 K-file (Dentsply Maillefer,), pulp tissue was removed using 5.25% sodium hypochlorite as an irrigant. The EALs were used in the following sequence: Joypex 5, RomiApex A-15, and Novapex.
In total, 180 measurements in 60 root canals were undertaken by the same experienced operator. The WL was defined as the most apical point of the root canal and was registered when the "0" or "OU" appeared on the EAL display. The WL was determined by inserting a K-file into the root canal until any of the afor ementioned marks were reached and remained stable for at least 5s. The file was then removed and the measurement made with a digital caliper (Mitutoyo, Suzano, SP, Brazil).
Data were analyzed statistically using paired t-tests with the Bonferroni correction for multiple comparisons in order to control the overall Type I error rate at 0.05. The Bland- Altman plots were used to determine inter-EAL reproducibility. Statistical analysis was performed using SPSS (SPSS Inc., Chicago, IL, USA).
Results
Three measurements were performed for each canal, one with each EAL. Table 1 shows mean and standard deviation (SD) values of absolute differences between pairs of the tested EALs. There were no significant differences between tested EALs (p>0.05; paired t-tests with the Bonferroni correction).
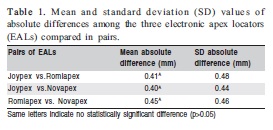
Table 2 shows the difference between the WL values measured by different pairs of EALs, with a high reliability between the EALs. In 38% of the canals full precision was achieved (difference of 0.0 mm) and, only in three cases, a difference greater than 2.0 mm was verified.
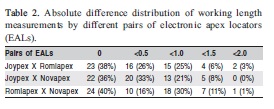
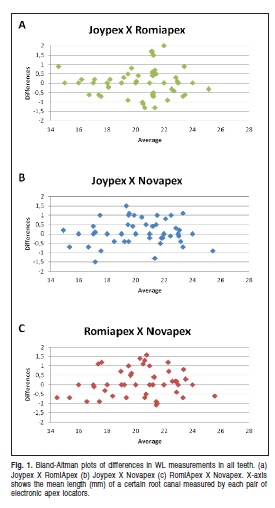
Figure 1 shows Bland-Altman plots of the differences in WL measurements in all patients with mean values and limits of agreement. Limits of agreement indicated the range that contained 98% of the differences between pairs of EALs and were between 0 and 2.0 for the three pairs of EALs. Bland- Altman plots with differences randomly scattered around a mean value close to zero confirmed the reproducibility of the three EALs. A random scatter of points along the X-axis on all three plots indicated that the inter-EAL reproducibility was independent of the length of the root canals. A random scatter of points along the Y-axis on all the three plots indicated that none of the three EALs showed predominantly longer or shorter WL measurements compared to the other EALs.
Discussion
The apical foramen location is extremely important to endodontic treatment success8. In general, 0.5-1.0 mm short to the radiographic apex is used as a reference for the foramen location and the working length. Apex locators have been developed to improve the accuracy of apical constriction determination and consequently increase the success rates of endodontic treatment2-5,9.
Several studies have reported the accuracy of EALs in determining the WL, validating its clinical use as a simple and effective alternative and optimizing endodontic therapy2-5,9-11. Although these studies have showed the clinical efficacy of EALs, the cost of this technology hinders their wider dissemination and use. Recently, new EALs were released with more accessible prices. A previous study has shown the efficacy of these EALs in vitro6, but this is the first clinical study comparing the reproducibility of a less costly EAL, Joypex 5, in relation to other EALs such as Novapex and Romiapex. The choice for Novapex and Romiapex was based on previous studies that have shown a good efficacy and accuracy of both EALs12-13.
All measurements were made by the same experienced and trained operator, thus eliminating the possibility of operator bias. Although the issue of how the operator's skill influences EAL accuracy has not yet been described in the literature, extensive training and practice are required to ensure familiarity with these devices and consequently accurate measurements14-15.
Root canals with unstable readings or different initial and repeated readings were excluded from this study. Only two root canals were excluded, indicating consistency of the tested EALs. These results were observed in a previous study that demonstrated a high clinical reproducibility of EALs12. A number of studies evaluated EALs, but comparisons of results should take into account the adoption of the same parameters of apical limits and the use of similar methods. In the present study, standardization of the WL measurements involved the same file type and size, irrigant concentration, reference point, and teeth serving as their own controls. This approach is similar to that of other studies and allows certain variables to be controlled in the clinical setting12-18.
The null hypothesis was upheld because no significant difference was observed in reproducibility among the tested EALs. This result confirms the clinical reliability of these devices to determine the WL, as in 69 out of 180 measurements there was no difference (0.0mm) and in 92 measurements the differences were approximately ± 0.5mm and ± 1.0 mm. A previous study showed that even the same EAL can have differences in the repeatability coefficient, showing different measurements values using the same sample13. Also, during the measurement of files with the caliper, small differences could result is nonidentical results. In addition, only 3 cases showed a greater difference than 2.0 mm, demonstrating high reproducibility among the EALs.
There is no study in the literature comparing the reproducibility of Joypex 5, RomiApex A-15 and Novapex either in vitro or in vivo, although several studies have shown the accuracy of Novapex and RomiApex A-1512-13,19-21. It is impossible to compare reproducibility and accuracy results as the former may be perfect even when the EALs are inaccurate. Furthermore, comparison of an accurate to inaccurate EAL results in unacceptable reproducibility. The accuracy of each EAL needs to be determined in order to differentiate which device is responsible for wide limits of agreement. The aim of study was not to determine which device was more or less accurate than others but to examine the reliability of various EALs in reproducing "APEX" readings under same clinical conditions. The results obtained in this study confirmed the clinical reproducibility of the EALs Joypex 5, RomiApex A-15 and Novapex.
References
1. Ricucci D. Apical limit of root canal instrumentation and obturation. Part 1. Int Endod J. 1998; 31: 384-93. [ Links ]
2. Cianconi L, Angotti V, Felici R, Conte G, Mancini M. Accuracy of three electronic apex locators compared with digital radiography: an ex vivo study. J Endod. 2010; 36: 2003-7. [ Links ]
3. Janner SF, Jeger FB, Lussi A, Bornstein MM. Precision of endodontic working length measurements: a pilot investigation comparing cone-beam computed tomography scanning with standard measurement techniques. J Endod. 2011; 37: 1046-51. [ Links ]
4. Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PM. The fundamental operating principles of electronic root canal length measurement devices. Int Endod J. 2006; 39: 595-609. [ Links ]
5. Ding J, Gutmann JL, Fan B, Lu Y, Chen H. Investigation of apex locators and related morphological factors. J Endod. 2010; 36: 1399-403. [ Links ]
6. Vardasca de Oliveira PT, Chita JJ, Silva PG, De Vicente FS, Pereira KF. Accuracy of two apex locators made in China compared to Root ZX II. Pesq Bras Odontoped Clin Integr. 2010; 10: 83-8. [ Links ]
7. Petrie A, Sabin C. Med Stati at a Glance. 3rd ed. Oxford: Wiley-Brackwell; 2009. [ Links ]
8. Kojima K, Inamoto K, Nagamatsu K, Hara A, Nakata K, Morita I et al. Success rate of endodontic treatment of teeth with vital and non-vital pulps. A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97: 95-9. [ Links ]
9. Grimberg F, Banegas G, Chiacchio L, Zmener O. In vivo determination of root canal length: a preliminary report using the Tri Auto ZX apex-locating handpiece. Int Endod J. 2002; 35: 590-3. [ Links ]
10. Plotino G, Grande NM, Brigante L, Lesti B, Somma F. Ex vivo accuracy of three electronic apex locators: Root ZX, Elements Diagnostic Unit and Apex Locator and ProPex. Int Endod J. 2006; 39: 408-14. [ Links ]
11. Ravanshad S, Adl A, Anvar J. Effect of working length measurement by electronic apex locator or radiography on the adequacy of final working length: a randomized clinical trial. J Endod. 2010; 36: 1753-6. [ Links ]
12. Miletic V, Beljic-Ivanovic K, Ivanovic V. Clinical reproducibility of three electronic apex locators. Int Endod. J 2011; 44: 769-76. [ Links ]
13. D‘Assunção FL, Alburquerque DS, Salazar-Silva JR, Dos Santos VC, Sousa JC. Ex vivo evaluation of the accuracy and coefficient of repeatability of three electronic apex locators using a simple mounting model: a preliminary report. Int Endod J. 2010; 43: 269-74.
14. Akisue E, Gavini G, de Figueiredo JA. Influence of pulp vitality on length determination by using the Elements Diagnostic Unit and Apex Locator. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104: 129-3. [ Links ]
15. Renner D, Grazziotin-Soares R, Gavini G, Barletta F. Influence of pulp condition on the accuracy of an electronic foramen locator in posterior teeth: an in vivo study. Braz Oral Res. 2012; 26:106-11. [ Links ]
16. Dunlap CA, Remeikis NA, Begole EA, Rauschenberger CR. An in vivo evaluation of an electronic apex locator that uses the ratio method in vital and necrotic canals. J Endod. 1998; 24: 48-50. [ Links ]
17. Venturi M, Breschi LA. A comparison between two electronic apex locators: an ex vivo investigation. Int Endod J. 2007; 40: 362-73. [ Links ]
18. Elayouti A, Dima E, Ohmer J, Sperl K, Ohle C, Lost C. Consistency of apex locator function: A clinical study. J Endod. 2009; 35: 179-81. [ Links ]
19. Stein TJ, Corcoran JF, Zillich RM. Influence of the major and minor foramen diameters on apical electronic probe measurements. J Endod. 1990; 16: 520-2. [ Links ]
20. Olson DG, Roberts S, Joyce AP, Collins DE, McPherson JC III. Unevenness of the apical constriction in human maxillary central incisors. J Endod. 2008; 34: 157-9. [ Links ]
21. Silveira LF, Petry FV, Martos J, Neto JB. In vivo comparison of the accuracy of two electronic apex locators. Aust Endod J. 2011; 37: 70-2. [ Links ]
 Correspondence:
Correspondence:
Emmanuel João Nogueira Leal da Silva
Rua Herotides de Oliveira, 61/902 – Icaraí
CEP: 24230-230 - Niterói - RJ - Brazil
E-mail: emmanuel@fop.unicamp.br
Received for publication: January 06, 2012
Accepted: May 03, 2012
