










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.3 Piracicaba Jul./Set. 2012
ORIGINAL ARTICLE
Craniocervical posture: cephalometric and biophotogrammetric analysis
Priscila WeberI; Eliane Castilhos Rodrigues CorrêaII; Jovana M. MilanesiI; Juliana Corrêa SoaresI; Maria Elaine TrevisanIII
IPhysical therapist, Msc in Human Communication Disorders, Federal University of Santa Maria - UFSM, RS, Brazil
IIProfessor, Program of Human Communication Disorders, Department of Physical Therapy, Federal University of Santa Maria - UFSM, RS, Brazil
IIIProfessor, Department of Physical Therapy, Federal University of Santa Maria - UFSM, RS, Brazil
ABSTRACT
AIM: To investigate the correlation between the craniocervical posture measurements obtained by the biophotogrammetric and cephalometric analysis.
METHODS: 80 women aged between 19 and 35 years were evaluated by the cephalometric and biophotogrammetric methods. The cephalometric variables were: CVA (position of flexion/extension of the head) CPL (forward head posture) CVT/EVT ratio (cervical column curvature). For the biophotogrammetric analysis, photography were analyzed in right profile being two angles related to the head forward posture (A1 and A2) and one related to flexion-extension head position (FE). It was also measured the curvature of the cervical spine by the cervical distance. The correlation between the craniocervical posture variables, as measured by the two methods of assessment, was analyzed by the Pearson's correlation with a significance level of 5%.
RESULTS: It was observed a moderate and significant agreement (p=0.00) between the postural craniocervical variables that analyzed the flexionextension head position (FE and CVA) and the forward head (CPL and A1). The evaluation of the cervical curvature by the DC measure showed no correlation with the cephalometric variable CVT/EVT.
CONCLUSIONS: The biophotogrammetric analysis can be preferably chosen for assessing the head posture. However, the cephalometric analysis appears to be the most indicated for the
cervical curvature measurement, since it enables a more objective view of the bone structures without the influence of the soft tissues.
Keywords: evaluation, posture, cephalometry, photogrammetry.
Introduction
The applicability and the methods of craniocervical postural analysis have been investigated in the literature in a multidisciplinary way, basically by experts in the field of Physical Therapy, Dentistry and Speech Therapy. There are several procedures that serve as an aid to craniocervical postural analysis, being three of them considered more populars1.
The classic method is based on visual analysis, using qualitative observations of postural asymmetries, having as a reference pattern the model proposed by Kendall2 (1995). Regardless of the examiner's experience, this type of measure is considered of less credibility in relation to quantitative measures3.
The second proposed method, the biophotogrammetry, stands out because it represents a simple, noninvasive and low-cost method. It consists in the analysis of angles and linear measurements of points marked on the skin in some of theindividual body segments. Such measures can be viewed and interpreted in digital photographic records. With the advancement of technology is considered the most requested method by professionals who perform postural assessment, both for investigative slant as to aid in the clinical diagnosis and in the therapeutic approach4. Moreover, the great advantage of biophotogrammetry is to allow changes in craniocervical posture to be quantified and small changes to be detected5.
Currently, the most accurate craniocervical postural analysis method is the cephalometry, in which it is used the lateral radiograph of the skull and of the cervical spine to perform cephalometric measurements. By means of the radiography, it is possible a more objective visualization of the craniocervicomandibular structures, without the influence of soft tissues, as occurs in the biophotogrammetry1. However, cephalometric analysis has little impact on clinical practice because the limitation of its applicability is related to high costs and technique complexity6.
Recent studies have sought to investigate the correlation between measurements of posture, obtained by biophotogrammetry and by visual analysis3,5. On the other hand, there are few studies investigating the correlation between the findings obtained by the biophotogrammetric and cephalometric analyses.
Considering the increasing number of studies using the biophotogrammetric analysis, because of the easy access to it in the clinical practice, it is necessary to develop studies to verify the agreement of the photographic method of the postural analysis with the radiographic method, which is more objective, but more expensive and with the individual's exposure to radiation. In other words, are biophotogrammetric measures related to head posture and does the cervical spine reflect the postural changes observed in the cephalometric analysis?
For its interdisciplinary approach, it is believed that this research is of interest to dentists, physical therapists, speech therapists and other professionals since it may assist them in the reflection of their clinical practice and in the context of scientific research.
Material and methods
Eighty women with mean age of 23.8 ± 3.65 years (19-35 years) and BMI of 22.4 ± 3.83 kg/cm2 recruited voluntarily through the print media participated in this study.
This research project was approved by the Ethics Committee in Health Research under the number 0048.0.243.000-08, recognized by the National Research Ethics (CONEP). All individuals who participated in the study were included by accepting and signing a free informed consent form.
The exclusion criteria of the study were: history of facial and/or craniocervical trauma, presence of acute and severe musculoskeletal pain, musculoskeletal deformities (scoliosis, congenital bone malformation), craniomandibular orthopedic surgical procedures and/or neck, and a previous diagnosis of cervical disc herniation.
Biophotogrammetric evaluation
The posture of the head and of the cervical spine was evaluated by means of digital photograph, with biophotogrammetric analysis by the postural assessment software (SAPO®). Pictures were taken in standing position in right lateral view.
Anatomic points were marked in the subject's body with white Styrofoam balls wrapped in reflective tape and previously prepared with double-sided tape for attachment to the skin. During the image acquisition, the volunteers were oriented to keep the usual body posture with opened eyes glancing to the horizon line.
The participants with suitable clothing, hair tied back and barefoot were photographed in a scenario constituted by a black background of 3x1.5 meters, a plumb line suspended in the roof beside the volunteer, a base with 10x40x20 centimeters of dimensions with the foot outline drawn in a rubber rug. A tripod (Vanguard® - VT 131) was positioned at a distance of, at least, 3 meters from the digital camera (Sony® Cybershot 7.2 megapixels) and in a 1.20 meter height from the floor. In order to reproduce the natural position of the head, the individual was instructed to look at the reflection of his eyes in a mirror positioned at one meter of distance7-10.
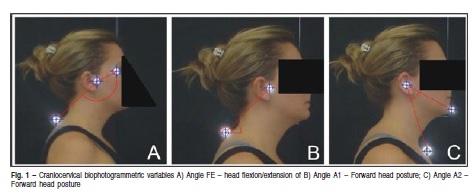
Four variables related to the craniocervical posture were evaluated (Figure 1). Three angles measured the position of the head, being two related to the forward head posture: A1 - angle formed between the tragus, spinous process of the seventh cervical vertebra (vertex) with the horizontal11-12 and A2 - angle formed between the external acoustic meatus (vertex), chin and sternal notch12. The third angle was related to the flexion-extension head position (FE) and it was formed by the points marked in the spinous process of the seventh cervical vertebra, tragus (vertex) and palpebral commissure11. The smaller the A1 angle and the greater the A2 angle, the more forward the head. Regarding the FE, the greater the angle, the greater the hyperextension of the head on the upper cervical spine.
The curvature of the cervical spine was measured by the horizontal distance from a vertical line tangent, by the apex of the thoracic kyphosis, called as thoracic plan, and by the point of the apex of the cervical concavity13.
With a one-week interval, the images of 20 individuals were randomly assigned to a second analysis of the variables to verify the intra-examiner reliability of the measurements.
Cephalometric evaluation
Subjects underwent a right lateral radiograph of the skull and of the cervical spine in a normal standing position, thus preserving the true resting position of the head and of the cervical spine. The posture adopted by the individual in the cephalometric evaluation of the right profile was the same as required for the acquisition of the photographic record, so that the natural position of the head was also reproduced.
The cephalometric radiography to assess the craniocervical posture was performed with the Orthophos Plus equipment (Siemens, Erlangen, Germany) with the chassis positioned parallel to the face and immediately adjacent to the shoulder of the individual to ensure the visualization of C7. It was used chassis with T MAT G Kodak film of de 18x24 cm, with a fixed focus distance of 1.52 m and in accordance with the protocol of radiation protection in accordance with Ordinance 453 of 06/01/1998 (Ministry of Health, Department of Health Surveillance).
All angles were traced manually by a single, previously trained examiner. The cephalograms were drawn on acetate paper with the aid of a mechanical pencil (graphite 0.3 mm) using a light box in order to enable a better visualization of the structures. A protractor to perform the angular measurements and a millimeter ruler for the linear measurements were used.
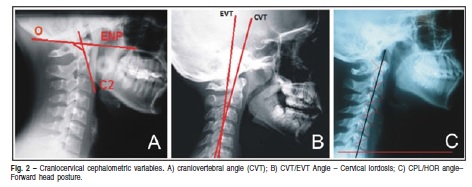
In the lateral radiographic record, three variables related to the posture of the head and of the cervical spine (Figure 2) were evaluated. The position of flexion/extension of the head was measured using the cranio-vertebral angle of Rocabado13 (1983), recently described in the literature3,14-15. This angle is formed by the McGregor Plane (a plane that touches the base of the occipital bone to reach the posterior nasal spine) and by the odontoid process (from the apex of the odontoid process of C2 to the most anterior and inferior point of the body of C2) . The smaller the CPL-Hor angle, the greater the hyperextension of the head on the upper cervical spine.
The forward head posture was measured by the angle formed by the intersection of the CPL line (craniocervical postural line) in relation to the horizontal8. The CPL line reaches the central points that are demarked in the body of the first six cervical vertebrae. The smaller the CPL-Hor angle, the more forward the head.
For the analysis of the cervical curve the CVT/EVT ratio was used15-16. The CVT line intersects the apex of the tooth of the second cervical vertebra with the most posterior-inferior point of the body of the fourth cervical vertebra, while the EVT line intersects the most posterior-inferior points of the body of the fourth and sixth cervical vertebrae. The smaller the CVT/EVT angle, the more rectified the cervical curvature.
The variables were measured by a single examiner through manual cephalometric tracing. With a one week interval, 20 radiographs were randomly assigned to a second analysis of the variables to verify the reliability of the performed tracing.
Statistical analysis
The Intraclass correlation coefficient (ICC) verifies the reliability of the cephalometric measurements. The ICC values should be greater than 0.75 to indicate good reliability andthose below 0.75 indicate poor to moderate reliability17.
A descriptive analysis of the demographic variables of age, weight, height and BMI was performed. Additionally, we analyzed the correlation between variables related to craniocervical posture measured by cephalometry and by biophotogrammetry as well as the correlation between postural variables measured by the two methods of evaluation. For this purpose, the Pearson´s coefficient was used ranging from -1 (negative correlation, variables vary in opposite direction) to 1 (positive correlation, variables vary in the same direction). The correlation was considered strong for values of correlation coefficient (r) greater or equal than 0.7, moderate when 0.3 <r <0.7, and weak when 0 < r < 0,318. Analysis were performed using the STATISTICA 7.1 (StatSoft Inc., Tulsa, OK, USA) and SPSS 17.0 (SPSS Inc., Chicago, IL, USA) softwares and a significance level of 5% was considered.
Results
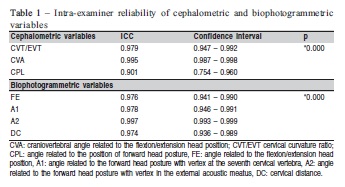
Results of the ICC showed excellent levels of reliability for all measurements in the biophotogrammetric and cephalometric analyses by the same examiner at two different times (Table 1).
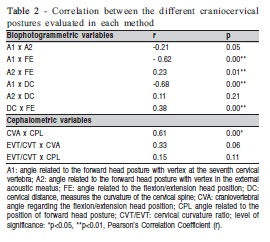
Correlations between biophotogrammetric and cephalometric variables tested separately for each method are presented in Table 2.
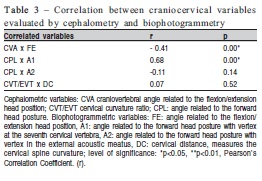
Table 3 shows the values related to the correlation between the two assessment methods of craniocervical posture. It was observed a moderate and significant agreement (p=0.00) between the craniocervical postural variables that measured the head flexion-extension position (CVA and FE) and the forward head posture (CPL and A1).
Discussion
The computerized biophotogrammetry is considered a reliable and reproducible method being an important tool in the evaluation of body posture3,19. High values of ICC for the craniocervical postural variables measured by means of the manual cephalometric tracing have been demonstrated20, corroborating the excellent levels of reliability for all drawing angles, in both biophotogrammetric and cephalometric analyses obtained in the present study.
Recent studies have used cephalometry as a tool for analyzing the alignment of the head and cervical spine in individuals with and without temporomandibular disorder, considering the hypothesis of a possible association betweencraniomandibular pain with the presence of postural changes in the craniocervical segment3,14,21. During radiographic and biophotogrammetric analysis, all volunteers were instructed to maintain their habitual posture. Thus, it was important to adopt natural head position in this study for faithfully representing the position of the craniocervical structures.
There are different biophotogrammetric measures capable of measuring the forward head as well as the cervical spine curvature and the head flexion/ extension. In a similar study, Silva et al.22 (2010) considered the use of the C7-tragus horizontal angle to characterize the forward head and the tragus-horizontal-eye angle to characterize the extension of the head.
Regarding the angular measurements used to assess the forward head posture through the biophotogrammetry (A1 and A2), a moderate and negative correlation between A1 and the angle of cranial flexion-extension (FE) was found. Thus, the forward head position required a head extension, possibly in order to maintain the horizontality of the optical plane23.
A moderate and a negative correlation between A1 and the cervical distance was found, that is, the more forward head posture (lowest angle), the greater the cervical distance. Neiva et al.24 (2009) reported that the forward head is characterized by the lower cervical flexion associated with the upper cervical extension, what in part, is in agreement with the photogrammetric findings of this study. The angles A1 and A2 showed to be consistent, but with a weak correlation.
In the analysis of cephalometric measurements, there were positive and moderate correlations between CVA and CPL. This finding strengthens the association between the forward head and the head extension. No significant correlation regarding the variable that measured the cervical curvature was observed (CVT/EVT).
Comparing the two different methods of assessment, the negative and moderate correlation between FE (biophotogrammetry) and CVA (cephalometry) reinforces the ability of the FE angle to evaluate head flexion/extension position. Furthermore, it was observed a positive and moderate correlation between A1 (biophotogrammetry) and CPL (cephalometry), confirming the ability of the A1 angle to evaluate the presence of a forward head. A positive and significant correlation between these variables was also demonstrated by Visscher et al.8 (2002), who also advocated the adoption of the natural head position during radiographic and photographic recordings. Similar craniocervical angular measurements were used by Van Niekerk et al.25 (2008) in the correlation between the photography and radiography, but in the sitting position. The authors considered the photogrammetric measurements valid and reliable for postural assessment.
Gadotti et al.5 (2010) considered another angle formed between chin, external auditory meatus and sternal notch (in this paper named A2) for testing the sensitivity of photogrammetry in evaluating the head posture in the sagittal plane. In the present study, this same photogrammetric measure compared with equivalent purposes used in cephalometry did not present significant correlation.
Rocabado13 (1983) reported that the head position on the neck related to the cervical spine curvature can be assessed by a distance (in cm) of a horizontal line, which has as reference the tangent to the apex of the thoracic spine, and the deepest point of the cervical spine. However, in this study, the DC (biophotogrammetry) showed no correlation with the cephalometric variable CVT/EVT expressing the cervical lordosis. Thus, it is assumed that this photogrammetric measure is best used for assessment of the forward head posture and not for the cervical curvature.
It is possible to study the craniocervical posture with reliable methods and without the exposure to radiation26. Based on the association found between the two methods regarding the analysis of the measures that characterized the forward head and the head flexion/extension, it can be suggested the use of the biophotogrammetric method to assess the craniocervical posture.
Based on the correlations obtained between the postural assessment methods, it can be concluded that computerized biophotogrammetry, apart from being reliable, seemed to be adequate to evaluate the head position. However, for analysis of the cervical curvature, it is suggested the radiographic method as a more objective view of the bone structures which are not influenced by the soft tissues.
References
1. Armijo-Olivo S, Jara X, Castillo N, Alfonso L, Schilling A, Valenzuela E, et al. A comparison of the head and cervical posture between the self-balanced position and the Frankfurt method. J Oral Rehabil. 2006; 33: 194-201. [ Links ]
2. Kendall F P, McCreary EK, Provance PG. Muscles: testing and function, with posture and pain. São Paulo: Manole; 1995. [ Links ]
3. Iunes DH, Bevilaqua-Grossi D, Oliveira AS, Castro FA; Salgado HS. Comparative analysis between visual and computerized photogrammetry postural assessment. Rev Bras Fisioter. 2009; 13: 308-15. [ Links ]
4. Iunes DH, Castro FA, Salgado HS, Moura IC, Oliveira AS, Bevilaqua-Grossi D. Intra and inter-examiner reliability and method repeatability of postural evaluation via photogrammetry. Rev Bras Fisioter. 2005; 9: 327-34. [ Links ]
5. Gadotti IC, Biasotto-Gonzalez DA. Sensitivity of clinical assessments of sagittal posture. J Eval Clin Pract. 2010; 16: 141-4. [ Links ]
6. Bryden L, Fitzgerald D. The influence of posture and alteration of function upon the craniocervical and craniofacial region. Craniofacial Dysfunction and Pain. In: Craniofacial dysfunction and pain: manual therapy, assessment, and management. London: Butterworth-Heinemann; 2001. p.164-71. [ Links ]
7. Solow B, Sandham A. Cranio-cervical posture: a factor in the development and function of the dentofacial structures. Eur J Orthod. 2002; 24: 447-56. [ Links ]
8. Visscher CM, de Boer W, Lobbezoo F, Habets LLMH, Naeije M. Is there arelationship between head posture and craniomandibular pain? J Oral Rehabil. 2002; 29 : 1030-6. [ Links ]
9. Ciancaglini R, Colombo-Bolla, G, Gherlone EF, Radaelli G. Orientation of craniofacial planes and temporomandibular disorder in Young adults with normal occlusion. J Oral Rehabil. 2003; 30: 878-86. [ Links ]
10. Rosa LP, Moraes LC. Comparative study of the influence of the conventional method and natural head posture for cephalometric lateral x-rays obtainment using the craniocervical analysis. Cienc Odontol Bras. 2009; 12: 56-62. [ Links ]
11. Lee WI, Okeson JP, Lindroth J. The relationship between forward head posture and temporomandibular disorders. J Orofac Pain. 1995; 9: 161-7. [ Links ]
12. Munhoz WC, Marques AP, Siqueira JTT. Evaluation of body posture in individuals with internal temporomandibular joint derangement. J Craniomandibular Pract. 2005; 23: 269-77. [ Links ]
13. Rocabado M. Biomechanical relationship of the crânio and hyoid regions. J Craniomandibular Pract. 1983; 1: 61-6. [ Links ]
14. Matheus RA, Ramos-Perez FMM, Menezes AV. The relationship between temporomandibular dysfunction and head and cervical posture. J Appl Oral Sci. 2009; 17: 204-8. [ Links ]
15. Currie P, Lobo-Lob S, Stark P, Metha N. The effect of maxillary molar distalization on cervical posture. J Stomat Occ Med. 2009; 2: 65-9. [ Links ]
16. Tecco S, Caputi S, Festa F. Evaluation of cervical posture following palatal expansion: a 12-month follow-up controlled study. Eur J Orthod. 2007; 29: 45-51. [ Links ]
17. Gadotti IC, Vieira ER, Magee DJ. Importance and clarification of measurement properties in rehabilitation. Rev Bras Fisiot. 2006;10: 137-46. [ Links ]
18. Chan VH. Biostatistics 104: Correlational Analysis. Singapore Med J. 2003; 44: 614-9. [ Links ]
19. Ferreira EAG, Duarte M, Maldonado EP, Burke TN, Marques AP. Postural assessment software (PAS/SAPO): validation and reliability. Clinics. 2010; 65: 675-81. [ Links ]
20. Chaves TC, Silva TSA, Monteiro SAC, Watanabe PCA, Oliveira AS, Grossi D B. Craniocervical posture and hyoid bone position in children with mild and moderate asthma and mouth breathing. Int J Pediatr Otorhinolarygol. 2010; 74: 1021-7. [ Links ]
21. Andrade AV, Gomes PF, Teixeira-Salmela LF. Cervical spine alignment and hyoid bone positioning with temporomandibular disorders. J Oral Rehabil. 2007; 34: 767-72. [ Links ]
22. Silva AG, Punt TD, Johnson MI. Reliability and validity of head posture assessment by observation a four-category scale. Man Ther. 2010; 15: 490-5. [ Links ]
23. Silva FWGP, Queiroz AM, Díaz-Serrano KV. Alteraciones posturales y su repercussion en el sistema estomatognatico. Acta Odontol Venez. 2008; ,46(4):1-17. [ Links ]
24. Neiva PD, Kirkwood RN, Godinho R. Orientation and position of head posture, scapula and thoracic spine in mouth-breathing children. Int J Pediatr Otorhinolarygol. 2009; 73: 227-36. [ Links ]
25. Van Niekerk S, Louw Q, Vaughan C, Grimmer-Somers K, Schereve K. Photographic measurement of upper-body sitting posture of high school students: A reliability and validity study. BMC Musculoskelet Disord. 2008; 9: 1-11. [ Links ]
26. Cuccia AM, Caradonna C. The measurement of craniocervical posture: A simple method to evaluate head position, Int J Pediatric Othorhinolaryngol. 2009; 73: 1732-6. [ Links ]
 Correspondence:
Correspondence:
Priscila Weber
Avenida Presidente Vargas 1855/1101, Centro
CEP: 97015-513, Santa Maria, RS – Brasil
E-mail: prifisio07@yahoo.com.br
Received for publication: June 25, 2012
Accepted: September 18, 2012
