










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.4 Piracicaba Out./Dez. 2012
ORIGINAL ARTICLE
Dental caries-related quality of life and socioeconomic status of preschool children, Bauru, SP
Angela XavierI; Fábio Silva de CarvalhoI; Roosevelt da Silva BastosII; Magali de Lourdes CaldanaIII; José Roberto de Magalhães BastosIV
IPhD student, Department of Pediatric Dentistry, Orthodontics and Community Health Dentistry, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
IIPhD, Professor, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
IIIAssociate Professor, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
IVProfessor, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
ABSTRACT
AIM: To evaluate oral health-related quality of life of preschool children of Bauru, State of São Paulo, Brazil, and associate it with socioeconomic profile of households.
METHODS: The sample consisted of 229 preschool children between 3 and 5 years and the dmft (decayed, missing due to caries, filled teeth) index was adopted for assessment children's dental caries in accordance with the standards recommended by the World Health Organization. Questionnaires were used for evaluation oral health-related quality of life (Early Childhood Oral Health Impact Scale) and socioeconomic profile of parents or guardians of the preschool children. Statistical analysis was performed descriptively by relative and absolute frequencies and by Spearman's correlation and Kruskal-Wallis test (p <0.05).
RESULTS: A dmft of 1.65 (± 2.87) and a Sic Index 4.88 (± 3.20) were found, indicating the polarization of dental caries in the studied group. It was verified low influence of oral health on quality of life of the children examined. With respect to socioeconomic classification, 66.38% of families were in the lower middle class. Linear and statistically significant correlation was found between dmft and oral health-related quality of life for the overall score and domains of the questionnaire (p<0.001).
CONCLUSIONS: It was found low influence of oral health on quality of life of the preschool children and the assessment of socioeconomic conditions of the children's families may guide practices aiming to reducing inequalities in the distribution of dental caries in the population.
Keywords: quality of life, dental caries, oral health.
Introduction
The association between social and economic conditions and dental caries prevalence has been observed in several studies1. Researchers have found that people living in precarious socioeconomic conditions are more favorable to be exposed to risk factors that influence oral health conditions, and this is directly related to quality of life, not only in functional domains, but also in its social and psychological ones2. The environment in which children live and grow up has also been reported as influencing their health behaviors and their perception of oral health3.
Oral health problems has been increasingly recognized as important factors causing a negative impact on daily performance and quality of life because they influence how people grow, enjoy life, speak, chew, taste food, and socialize4 Most studies on evaluation oral health status were carried out using only clinical measures, however, oral health-related quality of life (OHRQoL) instruments should be used in conjunction with them5. Adults' and children's perception of health conditions takes place in a different way and in the case of children that accuracy varies with cognitive capacity for each age group. This ability may vary according to the stage of emotional development, language or social environment of the child. Moreover, the socioeconomic and cultural conditions in which children were born and grew up may also influence their perception6.
Thus, there may be a child's difficulty in answering questions concerning the events in their health during a previous period of time depending on the age, where a questionnaire directed to 12-year-old children should not be answered by a 5-year-old child. The capacity for abstraction as well as comparisons of physical characteristics and personality starts from 6 years of age, and temporal concepts from 8 years of age. This mean that very young children as those in preschool age have difficulties in providing accurate information on the influence of oral health conditions on quality of life and, thus, questionnaires geared to this age group are answered by parents or guardians of them7.
Based on the foregoing considerations, the main purpose of this study was to evaluate the influence of oral healthrelated quality of life of preschool children of Bauru, State of São Paulo, Brazil, and associate it with socioeconomic profile of households.
Material and methods
The research protocol was approved by the Institutional Review Board (IRB) of Bauru Dental School, University of São Paulo, Brazil, (process no 156/2009), and the authorization for conduction of study was obtained from the municipal secretary education and directors of kindergartens. Also, written informed consent was obtained from the parents/legal representatives prior to enrolment of the children.
To perform this cross-sectional observational research the target population consisted of preschool children of public Kindergartens in Bauru, State of São Paulo, Brazil, totaling 6502 preschool children. The municipality of Bauru has 60 public kindergartens8 and the city was divided according to five regions described as follows: north, south, east, west and central region. Thus, the districts of each region were grouped to perform a raffle which would be the research participant. Likewise, schools of each district were grouped and randomly selected for the survey. This way, six public kindergartens were randomly selected to be part of the research.
Sample calculation was made based on the error levelá = 0.05 and â error level of 0.20. For this calculation, was established a correlation coefficient (R) of 0.20 finding an amount of 198 children to be examined.
Six hundred thirty (630) consent forms were sent to the five public kindergartens that were part of this research, and there was a response rate of 36.35% allowing children to participate in the study. The participating children were those who were in kindergarten at the time of the survey and who were allowed to participate in research through the informed consent signed by parents/guardians, and who permitted clinical examination. Therefore, 229 preschool children of both genders between 3 and 5 years of age were examined. However, this sample is not representative for preschool from public kindergarten population.
Clinical examinations were performed by a calibrated examiner and a recorder. An intra-examiner agreement of 0.92 was found. The preschool children were examined seated on chairs under natural light and the materials used for the clinical examinations were dental mirrors and CPI (Community Periodontal Index) probes in order to remove biofilm and to confirm visual evidence of caries. The clinical examinations used for observation of the mean number of decayed, missing due to caries or filled teeth (dmft index) were performed according to the criteria established by the World Health Organization (WHO)9.
To assess oral health-related quality of life of the preschool children was used the Early Childhood Oral Health Impact Scale (ECOHIS). The ECOHIS was developed by researchers of North Carolina University by the selection of 13 items from the 36 that comprise the questionnaire Child Oral Health Quality of Life Instrument (COHQOLI). The Brazilian version of the questionnaire was transculturally adapted in Brazil and this version has 14 questions, being 10 issues relating to the child subscale and 4 in the family's subscale. These items were considered most relevant to measure the impact of oral health on quality of life of preschool children and consider the experiences of the children's oral diseases and dental treatment10.
The ECOHIS is answered by the parents or guardians of the children, assessing their perceptions about the influence of oral health on quality of life of the children in preschool age. The responses options are listed in codes ranging from 0 to 5, where code 0 = never, 1 = almost never, 2 = sometimes 3 = frequently, 4 = very frequently 5 = do not know. The amount scores and domains were calculated from the sum of the reply codes. The responses "not know" were counted, but were excluded from the sum to calculate the amount score and by domain of each patient. The minimum score obtained in the questionnaire was zero corresponding to no influence of oral health on quality of life and the maximum was 56 where there was strong influence of oral health on quality of life of children.
It was proposed a classification of the questionnaire's results in different impacts aiming to verify the impact of oral health on quality of life of preschool children. The total score of the questionnaire ranges from 0 to 56 points. For the classification, score = 0 was considered with no impact and the score between 1 and 56 was divided into three equal ranges, being weak impact, when the sum score of the questionnaire is greater than zero and less than or equal to 18.67, impact medium when the result is greater than 18.67 and less than or equal to 37.34 and strong impact, when the score of the questionnaire is greater than 37.34 and less than or equal to 56.
For the socioeconomic classification of the family was used the methodology proposed by Graciano (1980) which assess five factors that received a score system. The sum of points allowed determination of an individual score and hence the ranking of the participants in one of the six classes propose11. Each of these factors has a specific goal, as follows:
Factor 1: The economic situation of the family. Seeks to identify the level of family income.
Factor 2: Number of family members. It is considered the number of family members who participate and/or depend on the economic situation.
Factor 3: Statement of the head of the family. With the evaluation of grade school to expand the possibilities for social mobility. Seeks to identify the education level of the medium in which the child lives.
Factor 4: Housing. Seeks to identify the status of ownership of their living.
Factor 5: Occupation of the head of the family. Seeks to identify through the profession and at the same time, social cultural and economic level of household head.
Depending on the sum of points from the evaluation is calculated socioeconomic classification itself, being: 0 to 5 points - Lower Low Class, 6 to 11 points- Upper Low Class, 12 to 20 points - Lower Middle Class, 21 to 29 points- Middle Class, 30 to 38 points- Upper Middle Class and over 39 - High Class.
Percentages of dmft and caries-free children were used to describe dental caries distribution among preschool children. Significant Caries Index (SiC Index), Gini Coefficient and Care Index were adopted to assess the unequal distribution of dental caries and oral health care.
SiC index was calculated by taking the mean dmft of the one third of the individuals having the highest of dmft values in a given population, and was used to measure the polarization of the dental caries occurrence among preschool children12. The Care Index was calculated using the means dmft without caries-free. The component "f" (filled teeth) was divided by the dmft and multiplied by 10013. The Gini Coefficient was used to assess inequality of caries distribution in this study14.
The Kruskal-Wallis test was used for comparison of dmft according to age. Spearman's correlation test was used to relate the mean dmft with the oral health-related quality of life and socioeconomic classification as well as to relate the results of oral health-related quality of life with the socioeconomic conditions. A significance level of 5% was adopted. The tests were calculated using Statistica 9.1 software.
Results
As much as 229 preschool children were recruited for the study, being 50.66% boys and 49.34 girls. These 229 children were part of the survey because consent forms were distributed beyond the amount calculated for the sample, due to losses that occur when distributing the consent forms of those mothers who do not want to allow the participation of children in research, being examined all children whose parents consented to participate.
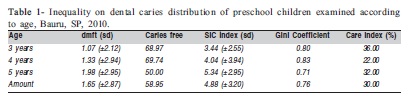
Table 1 summarizes the distribution of dental caries of preschool children examined according to age. There was a higher dmft in 5-year-olds than in 3-year-olds, whereas at 3 years it was found a dmft of 1.07 (2.12) and at 5 years a dmft of 1.98 (2.95). It was found a significant caries index of 4.88 (3.20), nearly three times higher than the average dmft.
The Gini coefficient shows a change from zero to one, where zero is related to absence of inequality and one demonstrates the presence of the same. In this population was observed a Gini Coefficient greater expressiveness in 4-year-olds (0.83), demonstrating the unequal distribution of dental caries.
The care index was used to assess the capacity of health services in meeting the needs of the population, which revealed a low percentage of care for this population (30.00%). In the 4-year-old group there was the lower percentage of care (22.00%), as described in Table 1.
With respect to socioeconomic status, it was found that 66.38% of the families of preschool children examined were classified in the lower middle class, 21.83% were classified in the middle class, 11.35% in the upper low, 0.44% in the upper middle class and there was no family in the lower low and high class.
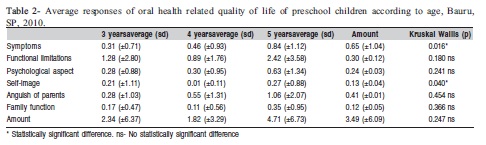
According to the responses of the different domains of the questionnaire oral health-related quality of life according to age, was verified that symptoms and functional limitations presented the highest means in subscale of children and anguish of parents demonstrated the highest mean in subscale of family. In the domains symptoms, psychological aspects and anguish of parents there was an increase in average with increasing age. It was verified statistically significant difference in the domains' symptoms (p=0.016) and selfimage (p=0.040), as shown in Table 2.
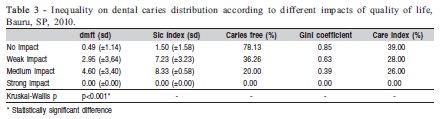
For the development of this research, it was proposed the assessment of the impact of oral health status in quality of life of preschool children, where it was observed 55.90%of children with no impact of oral health on quality of life, 39.74% with weak impact, 4.36% of the preschool children with medium impact, and no children with strong impact.
Assessing the dmft of children according to the different impacts of oral health on quality of life, it was found that children who showed no impact presented a dmft of 0.49 (1.14) and those who had a medium impact presented a dmft of 4.60 (3.40), where it was found a statistically significant difference between the different impacts (p<0.001). Moreover, it was found a reduction in the percentage of caries free children and the care index in accordance with the increasing impact of oral health on quality of life as described in Table 3.
Assessing the correlation between dmft and oral healthrelated quality of life was observed a linear and significant ratio for the overall score and domains of the questionnaire (p<0.001). Relating oral health-related quality of life with socioeconomic conditions of the families, it was observed a significant inverse relationship (r =- 0.183, p=0.006), i.e., with higher influence of oral health on quality of life of preschool children, lower the socioeconomic condition of households, as well as between oral health-related quality of life and income components (r =- 0.196, P= 0.003) and housing (r =- 0.166; p= 0.011). However, no relationship was found with the educational component of the parents or guardians (r =- 0.113, p= 0.086). Relating dmft with socioeconomic conditions of the families, it was found a significant inverse relationship (r = - 0.190, p= 0.003).
Discussion
In order to evaluate the prevalence and severity of dental caries according to WHO recommendations, this study used the dmft index. It was possible to evaluate the caries experience in preschool children from the city of Bauru, State of São Paulo. It could be observed polarization of dental caries in the studied group, with a Sic Index of 4.88 (+- 3.20) and it was found low care index, demonstrating the limited access of this population to health services and the low restorative care to which they have been exposed. The findings of this study are consistent with the goals of WHO for 2000 of 50% of caries-free children among 5-year-olds15, but are not consistent with the goals of WHO for 2020 in increasing the proportion of caries free children16.
It has been reported that when there is a large number of cases concentrated in a small group of individuals exist a phenomenon known as polarization17. This phenomenon is expressed in the concentration of greater burden of disease and treatment needs in a small portion of the population (20-40%), whereas most the children presents caries-free (40-60%), may be reflecting the measures of prevention and control of dental caries, based on solid population strategy, in which moved from a situation of high prevalence of the disease for a large percentage of caries-free individuals18. In this sense, the greater vulnerability to injury is associated with intense exposure to risk factors and social deprivation. In some studies, it was emphasized that the prevalence of dental caries decreased as socioeconomic level increased, even in areas without the addition of fluoride to public water supply19.
In order to quantify the extent which oral health problems interfere on daily life and well-being of people, were developed instruments of oral health-related quality of life to assess the impact of oral health in the physical and psychosocial development. Children, as well as young adults are also affected by several oral health problems, which have the potential to compromise the well-being and quality of life of them20-21.
The ECOHIS was developed for use in epidemiological studies aiming to evaluate the influence of oral diseases and treatment on preschool children's quality of life. It considers the experience of oral diseases and dental treatment of the child's lifetime with the answers provided by parents22.
There are few studies in the literature regarding the influence of oral health on quality of life of children in preschool age. This research found a greater influence of oral health on quality of life in the domains' symptoms and anguish of parents and lower means on self-image and family function. The maximum score obtained in the questionnaire was 33 points.
In this study the domains with the highest means were symptoms and functional limitations, which demonstrate that the influence of oral health on quality of life of children can be perceived by parents/guardians, when there are symptoms such as pain and limitations in daily activities such as speech and feeding. These results highlight the need to promote health education activities with parents or guardians of preschool children in order to raise awareness about the importance of maintaining a healthy primary dentition both for oral health and general health of children in this age group.
Similarly, Pahel et al. (2007) found that the highest average of the influence of oral health on quality of life domains were registered in symptoms, followed by functional limitations and emotional well-being. Children who had higher caries experience reported greater influence on quality of life that children who had lower caries experience7. In a research conducted by Abanto et al. (2010)22 with preschool children using the ECOHIS, parents reported greater impact related to the child's subscale (69.30%) than with family's subscale (30.70%). Parents reported no influence of oral health on quality of life in 40.10% and in 59.90% of children in child's subscales and family's subscale respectively. The maximum score of 30 was recorded at child's session and 12 on family's session.
A recent study conducted in the city of Diamantina, MG, Brazil showed that in the child impact section, "pain in the teeth, mouth or jaws" was the most frequently reported item by the parents (21.5%) and in the family impact section the most frequently reported item was "felt guilty" (14.2%)23.
This research also aimed to assess the perception of parents of oral health-related quality of life using a scale with different impacts from preschool children with no impact, weak impact, medium impact and strong impact, in order to facilitate their use in public health, where it was observed that 55.9 % of the children had no impact, i.e., a score of zero, and 39.74% were weak impact of oral health on quality of life. By linking the different impacts to the prevalence of dental caries, it was observed that children with medium impact showed a dmft of 4.60 (3.40) and those with no impact a dmft of 0.49 (1.14).
Likewise, the study by Li et al. (2008) revealed that the majority of parents reported a weak impact of oral health on quality of life of their children before they perform dental treatment, and according to the parents, the same children had dental problems that required treatment 24.
According to Baldani et al. (2002)15, the assessment of socioeconomic conditions allows to consider possible etiologic factors of social inequalities such as income, educational attainment and housing conditions. In this sense, it was found that 66.38% of the families evaluated in this study were in the lower middle class, 21.83%, in middle class, 11.35% in upper low and 0.44% in the upper middle class. Knowledge of these data allows a reorientation of health care and public spending on prevention and care activities, enabling a fair distribution of available resources, providing more resources to those groups with the greatest needs.
Epidemiological studies have been conducted to evaluate the relationship between oral health and socioeconomic conditions and have been observed that low socioeconomic status is related to higher prevalence of dental caries. The reason for the association between oral health and socioeconomic status is reasoned on the fact that socioeconomic status determines access to resources that determine the distribution of oral health, as well as, behavioral factors and consumption of sugar among them: toothbrushing, preventive activities and regular dental visits25.
Socioeconomic data were collected from parents in order to allow inequalities in oral health-related quality of life to be examined. An inverse and significant relationship was found between dmft and socioeconomic conditions (p=0.003) as well as the education level (p=0.046) and housing (p=0.010).
Likewise Meneghim et al. (2007)26 showed that income, education level, housing conditions and socioeconomic status have a significant relationship with higher prevalence of dental caries27. Similarly, a study conducted in Piracicaba, SP, Brazil, in 2009 found an inverse association between dental caries with income and with education level of the father and the mother.
The present study found inverse relation between oral health-related quality of life and socioeconomic conditions where children from low socioeconomic conditions demonstrated higher influence of oral health conditions on quality of life. These results indicate that people living in low socioeconomic conditions have worst oral health conditions due to exposure to risk factors interfering with their quality of life. Similarly, a study conducted with Brazilian schoolchildren found that higher impacts on COHRQoL were observed for children presenting with untreated dental caries. Socioeconomic factors were also associated with COHRQoL, as poorer scores were reported by children whose mothers had not completed primary education (RR 1.31; 95% CI 1.17-1.46) and those with lower household income (RR 1.17; 95% CI 1.05-1.31).2
Likewise, a study developed in Canada with schoolchildren demonstrated that in children from higher income backgrounds, mean CPQ11-14 scores were low, close to the minimum score of 10, irrespective of the presence or severity of oral diseases and disorders. For children from lower income backgrounds, those free of oral diseases and disorders also had relatively low scores. However, scores increased significantly in the presence of oral disease. This suggests that oral health problems have less perceived impact on high income children, but a more marked impact onchildren from low income environments3.
The questionnaires to evaluate oral health-related quality of life of preschool children can be a valuable instrument to demonstrate the perception of parents about the oral health of their children and to guide the oral health attention of this population group.
The present study identified low impact of oral health on quality of life of preschool children examined from the perspective of parents and verified socioeconomic inequalities associated with oral health related quality of life of the children. The results indicate the need of planning educational activities with parents about the importance of taking care of the primary teeth as well as the low capacity of the health system to treat people of this age group. The assessment of perceived needs by the use of quality of life questionnaires as well as socioeconomic parameters can assist the planning of oral health programs aiming the reduction of unnecessary and unavoidable inequalities in the distribution of dental caries in populations of different socioeconomic conditions.
Acknowledgements
The authors thank the children of public Kindergartens of the city of Bauru for their support in developing this study.
References
1. Ferraz MJPC, Queluz DPQ, Alves MC, Santos CCG, Matsui MY. Caries experience associated to social and preventive factors in children of a pastoral community from Limeira-SP. Braz J Oral Sci. 2011; 10: 152-7. [ Links ]
2. Piovesan CJLF, Guedes RS, Ardenghi TM. Impact of socioeconomic and clinical factors on child oral health-related quality of life (COHRQoL). Qual lLfe Res. 2010; 19: 1359-66. [ Links ]
3. Locker D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent Oral Epidemiol. 2007; 35: 348-56. [ Links ]
4. Piovesan C, Batista A, Ferreira FV, Ardenghi TM. Oral health-related quality of life in children: Conceptual issues. Rev Odont Cienc. 2009; 24: 81-5. [ Links ]
5. Koposova N, Widström E, Eisemann M, Koposov R, Eriksen HM. Oral health and quality of life in Norwegian and Russian school children: A pilot study. Stomatologija, BDM J. 2010; 12: 10-6. [ Links ]
6. Jokovic A, et al. Validity and Reliability of a Questionnaire for Measuring Child Oral-health-related Qual Life J Dent Res. 2002; 81: 459-63. [ Links ]
7. Pahel BT, Rozier RG, Slade GD. Paternal perceptions of children's oral health: The Early childhood oral helath impact scale (ECOHIS). Health Qual Life Outcomes. 2007; 5(6). [Cited 2010 Sept 10] Available from: www.hqlo.com/content/5/1/6. [ Links ]
8. Municipal Department of Education. The municipal Government of Bauru. [Cited 2012 Aug 20] Available from: http://www.bauru.sp.gov.br/secretarias/sec_educacao/infantil.aspx. [ Links ]
9. Word Health Organization. Oral health surveys, basics methods. 4th ed. Geneve: WHO; 1997. [ Links ]
10. Tesch FC, Oliveria BH, Leão A. Semantic equivalence of the Brazilian version of the Early Childhood Oral Health Impact Scale. Cad Saude Publica. 2008; 24: 1897-909. [ Links ]
11. Graciano MIG. Evaluation Criteria for Socioeconomic Classification. Serv Social Soc. 1980; 1: 81-103. [ Links ]
12. Nishi M, Stjernswärd J, Carlsson P, Bratthall D. Caries experience of some countries and areas expressed by the Significance Caries Index. Community Dent Oral Epidemiol. 2002; 30: 296-301. [ Links ]
13. Smith GE. Tooth decay in the developing world. N Z Med J. 1987; 100: 669-70. [ Links ]
14. Armfield JM, Spencer AJ, Slade GD. Changing inequalities in the distribution of caries associated with improving child oral health in Australia. J. Public Health Dent. 2009; 69: 125-34. [ Links ]
15. Bastos RS, Silva RP, Maia-Junior AF, Carvalho FS, Merlini S, Caldana ML et al. Dental caries profile in Monte Negro, Amazonian state of Rondônia, Brazil, in 2008. J Appl Oral Sci. 2010; 18: 437-41. [ Links ]
16. Hobdell M, Petersen PE, Clarkson J, Johnson N. Global goals for oral health 2020. Int Dent J. 2003; 53: 285-8. [ Links ]
17. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Dental caries in Brazil: decline, polarization, inequality and social exclusion. Pan Am J Public Health. 2006; 19: 385-93. [ Links ]
18. Sales Peres SHC, Carvalho FS, Carvalho CP, Bastos JRM, Lauris JRP. Polarization of dental caries in teen-agers in the Southwest of the state of São Paulo, Brazil. Cien Saude Colet. 2008; 13(Sup 2): 2155-62. [ Links ]
19. Baldani MH, Narvai PC, Antunes JLF. Dental caries and socioeconomic conditions in the State of Paraná, Brazil, 1996. Cad Saude Publica. 2002; 18; 755-63. [ Links ]
20. Barbosa TS, Gavião MBD. Oral health-related quality of life in children: Part II. Effects of clinical oral health status. A systematic review. Intern J Dent Hyg. 2008; 6: 100-7. [ Links ]
21. Peres KG, Peres MA, Araujo CLP, Menezes AMB, Hallal PC. Social and dental status along the life course and oral health impacts in adolescents: a population based birth cohort. Health Qual Life Outcomes. 2009; 7: 95. [ Links ]
22. Abanto J, et al. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol. 2011; 39: 105-14. [ Links ]
23. Martins-Júnior PA, Ramos Jorge J, Paiva SM, Marques LS, Ramos-Jorge ML. Validations of the Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS). Cad Saude Publica. 2012; 28: 367-74. [ Links ]
24. Li S, Malkinson S, Veronneau J, Allison PJ. Testing responsivenss to change for early childhood oral health impact scale (ECOHIS). Community Dent Oral Epidemiol. 2008; 36: 542-8. [ Links ]
25. Marmot M. Social determinants of health inequalities. The Lancet. 2005; 365; 1099-104. [ Links ]
26. Cortellazzi KL et al. Influence of socioeconomic, clinical and demographic variables on caries experience of preschool children in Piracicaba, SP. Rev Bras Epidemiol. 2009; 12: 490-500. [ Links ]
27. Meneghim MC, Kozlowski FC, Pereira AC, Ambrosano GMB, Meneghim ZMAP. A socioeconomic classification and the discussion related to prevalence of dental caries and dental fluorosis. Cien Saude Colet. 2007; 12: 523-9. [ Links ]
 Correspondence:
Correspondence:
Angela Xavier
Departamento de Pediatria, Ortodontia e Saúde
Coletiva, Faculdade de Odontologia de Bauru,
Universidade de São Paulo
Alameda Otávio Pinheiro Brisolla n° 9-75
CEP: 17012-901, Bauru, SP,Brasil
E-mail: dra.axavier@gmail.com
Received for publication: July 29, 2012
Accepted: November 28, 2012
