










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.13 no.3 Piracicaba Jul./Set. 2014
ORIGINAL ARTICLE
Sucking habits and anterior open bite among Venezuelan and Brazilian children
Andréia Carvalho CardosoI; Marisela González de BelloI; Flávio Vellini-FerreiraI; Rívea Inês Ferreira-SantosII
I Vellini Institute, Department of Orthodontics, São Paulo, SP, Brazil
II Universidade Paulista - UNIP, Department of Radiology, Campinas, SP, Brazil
ABSTRACT
Culturally different population groups have distinct infant feeding practices, which presumably may be related to diverse occlusal features in the primary dentition. Aim: To investigate the associations between nutritive and non-nutritive sucking habits and the prevalence of anterior open bite, in children from Aragua-Venezuela and São Paulo-Brazil. Methods: Seven calibrated examiners (κ = 0.89-1.0) performed clinical assessments in Venezuelans (N = 809) and Brazilians (N = 1,377) aged 3-6 years. Sucking habits were investigated using questionnaires answered by the mothers. Data were analyzed using logistic regression models (α = 0.05). Results: Among 380 children with anterior open bite, 309 were Brazilians. Approximately 65% of Brazilians with pacifier-sucking habit lasting beyond 3 years of age had this malocclusion. Brazilians who prolonged pacifier and digit-sucking habits beyond 3 years of age have, respectively, 68.5 and 14.5 times more chances of presenting anterior open bite than children without sucking habits (p < 0.001). In Venezuelans with open bite, 37.7% had digit-sucking habits beyond 3 years of age, resulting in a high odds ratio (9.3; p < 0.001) when compared to children without this habit. No significant effect was found for bottle feeding. However, non-breastfed Venezuelan children or those breastfed for periods shorter than 6 months have a two-fold higher chance of presenting anterior open bite than children who were breastfed for longer periods, p = 0.008. Conclusions: Infant feeding had some effect on Venezuelan children, since insufficient breastfeeding was related to a higher prevalence of anterior open bite. Pacifier-sucking was more prevalent in Brazilians, corresponding to pronounced chances (8-68 times greater) of diagnosing anterior open bite in pacifier users compared to non-users. Among Venezuelans, on the other hand, digit-sucking effect surpassed that of pacifier use and was associated with far higher chances (6-9 times) for this malocclusion.
Keywords: sucking behavior; open bite; child welfare; public health dentistry.
Introduction
Breastfeeding should be extensively promoted as opposed to bottle feeding and non-nutritive sucking habits, as far as it concerns the morphological, immunological and psychological aspects of child development1-5. Even though the relationship between prolonged non-nutritive sucking habits, especially pacifier use, and malocclusions in the primary dentition is well established3-10, the effect of bottle feeding is still controversial. Some studies diverge not only on the association between bottle feeding and the occurrence of malocclusions, but also as to the type of occlusal alteration5-8,11-12. In addition to methodological differences, there are sociocultural features involved in the development of sucking habits9,13-15.
A multicenter study, conducted on samples of 49 to 60 girls at 3 years of age in seven countries reported differences in the prevalence of sucking habits and some malocclusions, but no data were recorded on the prevalence of anterior open bite13. Open bites deserve clinical attention because the related dentoskeletal and myofunctional alterations require complex orthodontic treatment, which may include surgical procedures if there is no self-correction or interceptive treatment4,16. In childhood, the occurrence of anterior open bite is markedly associated to extended non-nutritive sucking habits4,5,7-12,14,17-22 and possibly related to bottle feeding8,11. Thus, the present study aimed at evaluating the effects of nutritive and non-nutritive sucking habits on the prevalence of anterior open bite in preschool children from Aragua- Venezuela and São Paulo-Brazil.
Material and methods
The research project was approved by Institutional Review Boards in Venezuela (protocol #014-2008) and Brazil (protocol #13505843), in compliance with the Helsinki Declaration.
Sample selection
In the state of Aragua (north-central Venezuela), among a total of 1,000 children recruited, information was selected from 809 (414 girls, 395 boys), enrolled in 12 public preschools in the cities of Girardot (N = 320), Mario Briceño Irragory (N = 217) and Santiago Mariño (N = 272), which are close to the capital Maracay. In the state of São Paulo (southeastern Brazil), specifically in the eastern region of São Paulo city, the sample comprised 1,377 children (687 girls, 690 boys) selected among 2,700 students enrolled in 11 public preschools. Information on the general health of the children, sociodemographic characteristics (name, birth date and sex of the children, monthly family income and parents' educational level), methods and duration of infant feeding and history of non-nutritive sucking were investigated by a prestructured questionnaire answered by the mothers.
Most families in both samples presented low-to-medium income. The Brazilian sample was geographically located in a strongly industrialized region with marked effect of capitalism. Venezuelans, however, lived in smaller less industrialized cities. According to the mothers' information, most parents had attended high school and, in general, completed this educational level. It was estimated that up to 10% of parents had college education.
Children included in Venezuelan and Brazilian samples met the following criteria: age range from 3-6 years, the predominant chronological age was 5 years, followed by 4 years in both Venezuelan (63.7% and 30.8%) and Brazilian (39.2% and 35.4%) samples; compliance during clinical examination; complete primary dentition, without erupted or erupting permanent teeth; absence of extensive carious lesions, coronal destructions or proximal restorations that might alter occlusion; no early loss of primary teeth and/or dental anomalies of shape, number, structure and eruption; and no syndromes and/or cleft lip and palate or any other developmental anomalies that might impair breastfeeding. Children had never been submitted to orthodontic treatment or speech therapy. Some children were excluded from Venezuelan (N = 191) and Brazilian (N = 1,323) samples because their parents did not sign the free and informed consent form, their mothers did not return the questionnaires, some questionnaires were answered ambiguously or incompletely, or the children did not meet the inclusion criteria.
The structured questionnaire was previously validated in a pilot study in Brazil to analyze the reliability of responses given by 30 mothers who answered it twice, with a six-month interval between the first and second survey. This group of 30 mothers was not included in the study samples. All variables presented high intra-examiner agreement, with Kappa (κ) coefficients of approximately 0.933,4,6. A Venezuelan version of the Brazilian questionnaire was prepared by a native orthodontist, who considered linguistic meaning, social issues equivalence and cross-cultural translation23, and then revised by the researchers who first planned the questions.
Occlusal assessment
Clinical examinations were conducted by four dentists in Venezuela and three in Brazil, who had been properly calibrated (κ = 0.89-1.0). Occlusal assessments were performed in school environment, with the child comfortably seated in an upright position under artificial light source. By visual inspection, with the child occluding in maximum intercuspation, the overbite was classified into three categories4: normal (maxillary central incisors covering nearly one third of the clinical crown of mandibular central incisors or edge-to-edge contact between maxillary and mandibular teeth), negative or anterior open bite (vertical distance of incisal edges of maxillary and mandibular teeth in the anterior region) and increased or deep bite (maxillary central incisors covering more than one third of the clinical crown of mandibular central incisors).
Study groups
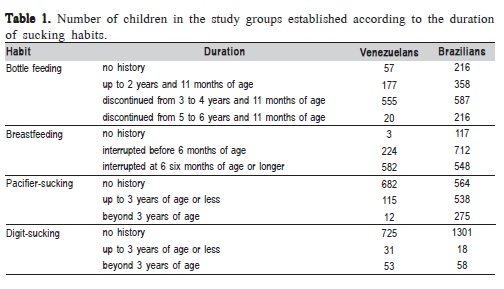
Venezuelans and Brazilians were divided into different bottle feeding2,11, breastfeeding15, pacifier-sucking20 and digitsucking groups according to the duration of these habits (Table 1).
Statistical analyses
A binary logistic regression model with multiple explanatory variables was adjusted, including infant feeding methods, non-nutritive sucking habits and two population groups, to analyze a possible effect of geographic location/ culture on the frequency of anterior open bite. The reference explanatory variables for comparisons were: Venezuela (geographic location/culture), absence of history (bottle feeding, pacifier use and digit-sucking habit) and no breastfeeding. Two additional logistic regression models were adjusted to analyze the effect of sucking habits duration on the prevalence of anterior open bite in Venezuelans and Brazilians. The significance level was set at 0.05 and the analyses were performed using the MINITAB® 14 (Minitab Inc., State College, PA, USA) software.
Results
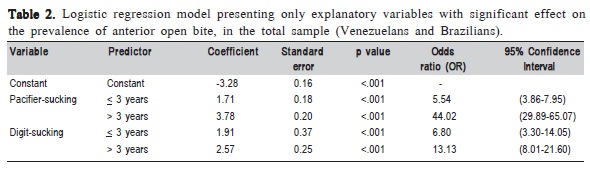
Considering both population groups (N = 2,186), 1,806 children did not present anterior open bite. However, among the 380 children with this malocclusion, 309 were Brazilians. Despite the high number of Brazilian children with anterior open bite, the logistic regression model adjusted for combined analysis of all explanatory variables did not indicate a significant effect of geographic location. In the total sample, including Venezuelans and Brazilians, only the duration of pacifier and digit-sucking habits demonstrated statistically significant effects on the prevalence of anterior open bite (Table 2).
Because each type of sucking habit may have a different effect according to the sociocultural characteristics of the two population groups, individual logistic regression models were adjusted for Venezuelan and Brazilian children.
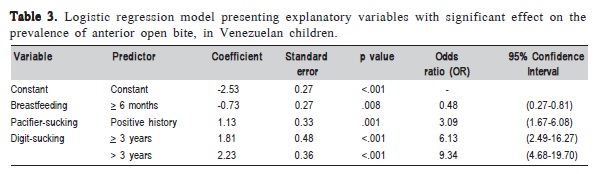
In the Venezuelan sample, besides the significant effects of non-nutritive sucking habits, which corroborate those in Table 2, breastfeeding extended to or beyond 6 months of age was significantly associated to decreased prevalence of anterior open bite (Table 3). For this model, the reference explanatory variables were: no breastfeeding and breastfeeding for a period shorter than 6 months (these subgroups were combined, since only three children had never been breastfed) and no history of pacifier and digit-sucking habits. Concerning pacifier-sucking, there was a very small number of children with anterior open bite that persisted with the habit beyond the age of 3 years (N = 1). Thus, positive and negative histories of pacifier use were considered.
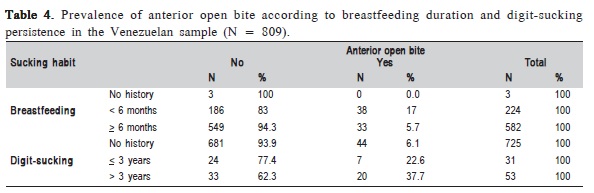
Children who were never breastfed or those who were breastfed for less than 6 months would have 2.08 (1/0.48) times more chances of presenting anterior open bite than those who were breastfed for 6 months or longer (Table 3). In a subgroup of 582 Venezuelans who were breastfed for 6 months or longer, only 5.7% (N = 33) had anterior open bite (Table 4). It should be noted that, in Venezuelan children, the effect of digit-sucking habit was more accentuated than pacifier use. Children with persistent digit-sucking habits beyond the age of 3 years (majority in the subgroup of digit suckers) would have 9.34 times more chances of presenting anterior open bite compared to those without this habit (Table 3). In the two groups with history of digit-sucking, the frequencies of anterior open bite were higher compared to children without this habit, reaching up to 37.7% in those who persisted with the habit beyond 3 years of age vs 6.1% in the counterpart (Table 4).
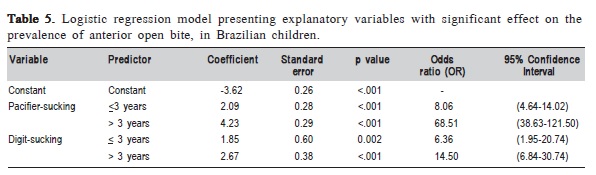
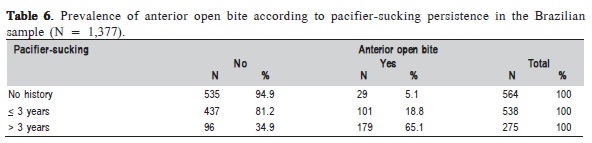
In the Brazilian sample, the effects of pacifier and digitsucking habits on the prevalence of anterior open bite surpassed any possible influence of other explanatory variables (Table 5). Pacifier use was very frequent in Brazilians (Table 1). The chances of diagnosing anterior open bite would be surprisingly high if the pacifier-sucking habit persisted beyond the age of 3 years (OR = 68.51, p < 0.001). Table 6 points out that approximately 65% of Brazilian children with pacifier-sucking habits that persisted beyond the age of 3 years presented anterior open bite.
Discussion
The prevalence of anterior open bite was four-fold higher in the Brazilian sample as compared with the Venezuelans. Notwithstanding the scientific relevance of this finding, the present study results should be carefully interpreted, since the sample analyzed in Venezuela is not representative of the country, yet provides indicators of regions close to the state capital of Aragua, Maracay. Similarly, the Brazilian sample provides epidemiological indicators of the eastern region of São Paulo city and due to the wide geographic dimensions and cultural peculiarities between and within states the frequencies of malocclusions and sucking habits may be different in relation to other cities.
Based on Table 4, a total of 71 children had anterior open bite, corresponding to 8.8% of the Venezuelan sample (N = 809). The respective percentage for the Brazilian sample (N = 1,377) was 22.4%. The prevalence of anterior open bite in children aged 3-6 years from Gran Caracas, which is located relatively close to Maracay, but classified as the largest and highly industrialized city of Venezuela, was estimated in 32.7%15. Two epidemiological studies carried out in different cities in the São Paulo state reported different frequencies of anterior open bite. In Piracicaba city, the prevalence of anterior open bite in 5-year-old children was 32.4%12. Conversely, in Araçatuba city, another study registered a prevalence of 14.4% for this malocclusion in children aged 5-6 years5. No parameters for comparison were found, since the scientific literature lacks multicenter studies on the sociodemographic factors implied in the etiology of anterior open bite.
Most Venezuelan and Brazilian parents have attended high school and some of them studied at a university, albeit with low-to-medium registered income. Information on monthly income and parental schooling are in agreement with that reported by previous research5. In fact, the effective role of some sociodemographic variables on malocclusion etiology, mainly in the primary dentition, is not completely elucidated7-8. Nevertheless, it may be assumed that parental schooling, family income and social class exert some positive effect on routine health practices5,12,18.
Considering both population groups, the effects of nonnutritive sucking habits were predominant in the chances of occurring anterior open bite (Table 2). Children who persisted with pacifier use beyond 3 years of age would present 44 times higher chances of having anterior open bite compared to those without history of this habit (p < 0.001), corroborating previous studies4,5,8-12,18. In the Brazilian sample, the effect of pacifier-sucking extended beyond 3 years of age was stronger than digit-sucking (Table 5). Similarly, in a Portuguese sample, the chances of diagnosing an anterior open bite in the primary dentition were higher among pacifier users (OR = 61.7, p < 0.05) than in children with thumbsucking habit (OR = 5.6, p < 0.05)9-10. In some Brazilian4, Spanish21 and Portuguese9 samples pacifier use has been reported with much higher frequency, compared with digitsucking. The opposite effect was observed for Venezuelan children (Table 3). This finding is in agreement with data from a Nigerian sample of children aged 2-5 years, in which the frequency of digit-sucking (59.6%) surpassed that of pacifier use (4.5%)14.
Moreover, extending breastfeeding to 6 months of age or longer was associated to lower frequency of anterior open bite in Venezuelans (Table 3). Non-breastfed children or those who were breastfed for less than 6 months would have 2.08 times more chance of presenting this malocclusion (p = 0.008). Breastfeeding was found to be a protective factor, stimulating the skeletal and muscular development of the child's face3,8. Open bite in the primary dentition was already associated to absence of breastfeeding or early weaning in two Brazilian studies4,18. Interestingly, in the Venezuelan sample, a higher frequency of anterior open bite was associated to weaning in an earlier period of life (< 6 months) in relation to previous study18. Peres et al.18 (2007) stated that breastfeeding for less than 9 months was a significant risk factor for developing anterior open bite. Romero et al.4 (2011) explained that breastfeeding interrupted between 6 and 12 months of age, or beyond 12 months of age, positively influenced dental occlusion, when compared with the complete absence of breastfeeding. However, breastfeeding for longer than 12 months of age had by far the best effect.
According to this study findings, it seemed that the protective effect of breastfeeding for periods equal to or longer than 6 months on the development of anterior open bite may have been obscured by the high frequencies of pacifier use among Brazilian children1,2,4,5,12,13. Nevertheless, it should be emphasized that breastfeeding beyond 6 months of age has a beneficial effect for avoiding the establishment of nonnutritive sucking habits1,2,8, thus indirectly favoring craniofacial development and preventing the occurrence of malocclusions and myofunctional alterations3,4,17.
Although some authors reported the effect of bottle feeding on the higher prevalence of anterior open bite8,11, the present study did not support this kind of association. This disagreement may be related to methodological differences, especially in the categorization of feeding groups, and sociocultural aspects. Furthermore, bottle feeding alone was not directly associated with higher prevalence rates of increased overjet and Class 2 canine relationship in the primary dentition6.
The effects of both analyzed non-nutritive sucking habits on the prevalence of anterior open bite were demonstrated by population group (Tables 3 and 5). However, the diagnosis of anterior open bite in some Brazilian children who did not use pacifiers (5.1%, Table 6 and Venezuelan children without history of digit-sucking (6.1%, Table 4), specifically mentioning that in the latter sample only 3 participants with anterior open bite were pacifier users. This encourages further studies on the possible role of other factors in the etiology of the types of malocclusion evaluated. Some authors stated that non-nutritive sucking habits, in addition to the direct influence, would also have an indirect effect on the etiology of malocclusions by the association with an abnormal swallowing pattern17,22. Anterior open bite has been related to a skeletal pattern with lower values for overbite and mandibular ramus height24. There was association between facial morphology and anterior open bite in children at 6 years of age. Children with mesofacial or dolichofacial morphology exhibited higher prevalence of this malocclusion19. Prolonged non-nutritive sucking habits and hyperdivergent facial pattern may be significant risk factors for the development of anterior open bite10.
From primary to mixed dentition, there is a tendency of self-correction of the anterior open bite after interruption of the non-nutritive sucking habits10,21-22. The diagnosis of anterior open bite, careful examination is mandatory, since this malocclusion may be diagnosed with other anomalies, i.e., posterior crossbite and tongue thrust. An anterior open bite alone will probably self-correct whenever the nonnutritive sucking habits are discontinued. Therefore, the dental team must be prepared for counseling parents or caregivers. Great efforts should be made to help the child discontinuing non-nutritive sucking habits before 3 years of age20, to prevent structural and myofunctional alterations that might sustain the morphological malocclusions17. Considering that bottle feeding has been related to the pacifier-sucking habit2, it is advisable to introduce semi-solid and solid foods as soon as the child has teeth and is able to perform masticatory movements, replacing the achievement of nutrients via baby bottle4.
In sum, this study demonstrated that anterior open bite was much more frequent, i.e. four-fold higher, in Brazilian children than in Venezuelans. Interestingly, considering only the Venezuelan sample, insufficient breastfeeding was related to a greater prevalence of anterior open bite in the primary dentition. Venezuelan children breastfed for 6 months or longer would have less chances of developing this malocclusion. Concerning non-nutritive sucking habits, pacifier-sucking was more prevalent in Brazilians, thus corresponding to increased chances (8-68 times greater) of diagnosing anterior open bite in pacifier users compared with non-pacifier users. In Venezuelans, digit-sucking effect surpassed that of pacifier use and was associated to far higher chances (6-9 times) for anterior open bite.
References
1. Moimaz Suzely AS, Zina LG, Saliba NA, Saliba O. Association between breast-feeding practices and sucking habits: A cross-sectional study of children in their first year of life. J Indian Soc Pedod Prev Dent. 2008; 26: 102-6. [ Links ]
2. Telles FBA, Ferreira RI, Magalhães LNC, Scavone-Junior H. Effect of breast- and bottle-feeding duration on the age of pacifier use persistence. Braz Oral Res. 2009; 23: 432-8.
3. Kobayashi HM, Scavone Jr H, Ferreira RI, Garib DG. Relationship between breastfeeding duration and prevalen
4. Romero CC, Scavone-Junior H, Garib DG, Cotrim-Ferreira FA, Ferreira RI. Breastfeeding and non-nutritive sucking
5. Santos RR, Nayme JG, Garbin AJ, Saliba N, Garbin CA, Moimaz SA. Prevalence of malocclusion and related oral habits in 5- to 6-year-old children. Oral Health Prev Dent. 2012; 10: 311-8.
6. Jabbar NSA, Bueno ABM, Silva PE, Scavone-Junior H, Ferreira RI. Bottle feeding, increased overjet and Class 2 primary canine relationship: is there any association? Braz Oral Res. 2011; 25: 1-7.
7. Oliveira AC, Paiva SM, Martins MT, Torres CS, Pordeus IA. Prevalence and determinant factors of malocclusion in children with special needs. Eur J Orthod. 2011; 33: 413-8.
8. Vasconcelos FM, Massoni AC, Heimer MV, Ferreira AM, Katz CR, Rosenblatt A. Non-nutritive sucking habits, anterior open bite and associated factors in Brazilian children aged 30-59 months. Braz Dent J. 2011; 22: 140-5.
9. Urzal V, Braga AC, Ferreira AP. Oral habits as risk factors for anterior open bite in the deciduous and mixed dentition - cross-sectional study. Eur J Paediatr Dent. 2013; 14: 299-302.
10. Urzal V, Braga AC, Ferreira AP. The prevalence of anterior open bite in Portuguese children during deciduous and mixed dentition—correlations for a prevention strategy. Int Orthod. 2013; 11: 93-103.
11. Charchut SW, Allred EN, Needleman HL. The effects of infant feeding patterns on the occlusion of the primary dentition. J Dent Child (Chic). 2003; 70: 197-203.
12. Hebling SRF, Cortellazzi KL, Tagliaferro EPS, Hebling E, Ambrosano GMB, Meneghim MC, et al. Relationship between malocclusion and behavioral, demographic and socioeconomic variables: a cross sectional study of 5-year-olds. J Clin Pediatr Dent. 2008; 33: 75-9.
13. Caglar E, Larsson E, Andersson EM, Hauge MS, Øgaard B, Bishara S, et al. Feeding, artificial sucking habits, and malocclusions in 3-year-old girls in different regions of the world. J Dent Child (Chic). 2005; 72: 25-30.
14. Ize-Iyamu IN, Isiekwe MC. Prevalence and factors associated with anterior open bite in 2 to 5 year old children in Benin city, Nigeria. Afr Health Sci. 2012; 12: 446-51.
15. Blanco-Cedres L, Guerra ME, Rodrígues S. Breastfeeding and dental malocclusions in preschool children from Gran Caracas. Acta Odontol Venez. 2007 [cited 2008 Mar 14]. Available from: http:// www.actaodontologica.com/ediciones/2007/2/lactancia_materna_maloclusiones_ dentales.asp.
16. Park YC, Lee HA, Choi NC, Kim DH. Open bite correction by intrusion of posterior teeth with miniscrews. Angle Orthod. 2008; 78: 699-710.
17. Ovsenik M, Farcnik FM, Korpar M, Verdenik I. Follow-up study of functional and morphological malocclusion trait changes from 3 to 12 years of age. Eur J Orthod. 2007; 29: 523-9.
18. Peres KG, Latorre MRDO, Sheiham A, Peres MA, Victora CG, Barros FC. Social and biological early life influences on the prevalence of open bite in Brazilian 6-year-olds. Int J Paediatr Dent. 2007; 17: 41-9.
19. Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008; 30: 580-5.
20. Dimberg L, Bondemark L, Söderfeldt B, Lennartsson B. Prevalence of malocclusion traits and sucking habits among 3-year old children. Swed Dent J. 2010; 34: 35-42.
21. Franco Varas V, Gorritxo Gil B. Pacifier sucking habit and associated dental changes. Importance of early diagnosis. An Pediatr (Barc). 2012; 77: 374-80.
22. Dimberg L, Lennartsson B, Söderfeldt B, Bondemark L. Malocclusions in children at 3 and 7 years of age: a longitudinal study. Eur J Orthod. 2013; 35: 131-7.
23. Su CT, Parham LD. Generating a valid questionnaire translation for crosscultural use. Am J Occup Ther. 2002; 56: 581-5.
24. Klocke A, Nanda RS, Kahl-Nieke B. Anterior open bite in the deciduous dentition: longitudinal follow-up and craniofacial growth considerations. Am J Orthod Dentofacial Orthop. 2002; 122: 353-8.
 Correspondence:
Correspondence:
Rívea Inês Ferreira-Santos
Universidade Paulista (UNIP) - Campus Swift
Avenida Comendador Enzo Ferrari, 280
CEP: 13045-770 – Swift, Campinas, SP, Brasil
E-mail: riveaines@gmail.com
Received for publication: June 29, 2014
Accepted: September 02, 2014
