










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.63 no.2 Porto Alegre Abr./Jun. 2015
ORIGINAL / ORIGINAL
Glove perforations after dental care
Perfurações em luvas após atendimento odontológico
Thália Líbni Costa Saraiva FULLYI; Eudes Euler de Souza LUCENAI; Tasiana Guedes de Souza DIASI; Jimmy Charles Melo BARBALHOI; Vicente Cleiton Ferreira LUCENAI; Hécio Henrique de Araújo MORAISI
I Universidade do Estado do Rio Grande do Norte, Curso de Odontologia. Rua André Sales, Paulo VI, 59300-000, Caicó, RN, Brasil
ABSTRACT
Objective
To assess surgical and procedure glove perforations after dental care.
Methods
A total of 279 pairs of gloves pairs were analyzed, 36 surgical and 243 procedure gloves used in the dentistry specialties surgery, cosmetic dentistry, endodontics, pediatric dentistry, periodontics, and prosthodontics. A diluted alkaline solution of fuchsine in water was used for analyzing the gloves. Each glove was filled with 500 ml of the solution and manually pressed at the height of the wrist for two minutes. Statistical analysis included the chi-square test at a significance level of 5%.
Results
Of the 279 study gloves, 106 had been perforated, corresponding to 38%. Most perforations occurred in the dominant hand, mainly in the finger area. Most procedures that caused perforations lasted more than 40 minutes, and most were in the area of cosmetic dentistry.
Conclusion
There were a considerable number of perforations in the study gloves, which can increase the risk of cross-infection between students and patients.
Indexing terms: Dentistry. Exposure to biological agents. Infection. Surgical gloves.
RESUMO
Objetivo
Avaliar as perfurações que acometem as luvas cirúrgicas e de procedimentos após o uso no tratamento odontológico.
Métodos
Foram analisados 279 pares de luvas, sendo 36 pares de luvas cirúrgicas e 243 pares de luvas de procedimentos, utilizados na prática odontológica nas especialidades de Cirurgia, Dentística, Endodontia, Odontopediatria, Periodontia e Prótese. Para análise das luvas, foi utilizada uma solução de fuccina básica diluída em água, cada luva foi preenchida com 500 ml de solução, seguida de compressão manual na altura do punho da luva por dois minutos. A análise estatística foi realizada pelo método do Qui-quadrado, adotando-se como nível de significância 5%.
Resultados
Dos 279 pares de luvas analisadas, 106 pares tiveram perfurações, o que corresponde a 38%. A mão que mais sofreu perfurações foi a mão dominante, e a região mais acometida foi a região digital. Observou-se que a maioria dos procedimentos realizados durou mais de 40 minutos, e que houve uma maior frequência de procedimentos realizados na área da Dentística.
Conclusão
Conclui-se que houve um considerado número de perfurações presentes nas luvas analisadas, o que pode contribuir para um maior risco de infecção cruzada para acadêmicos e pacientes.
Termos de indexação: Exposição a agentes biológicos. Infecção. Luvas cirúrgicas.
INTRODUCTION
Dentistry is a profession characterized by exposure of both professionals and their teams to a variety of infectious agents. The use of personal protection equipment, such as cap, mask, glass, white coat, and gloves are essential for the safety of the dental team and the patient1. When not perforated, latex procedure and surgical gloves act as an effective protective barrier against contagious diseases, such as acquired immunodeficiency syndrome (AIDS), hepatitides, and herpetic diseases, among others.
When glove integrity is breached, professionals become at risk of direct contamination or act as a disease transmission vehicle. The main functions of intact gloves are to reduce the risk of professional contamination by pathological agents present in the patient's blood or saliva, to reduce the chances of microorganism transmission from the resident microbiota of the dentist's hand to the patient, and to reduce the possibility of the professional's hands transferring microorganisms from the mouth of one patient to the mouth of another.
The National Sanitary Surveillance Agency (ANVISA), through RDC no. 05/2008, provides the minimum identity and quality requirements for surgical and nonsurgical procedure gloves made of natural rubber, synthetic rubber, or a mixture thereof, under the regimen of the sanitary surveillance, defining its aspects, such as surface, shape, sterilization method, use of powder or other lubricants, and manufacturing and sales requirements (packaging, labeling, and storage). Moreover, according to Article 7 Paragraph III of RDC number 5 of ANVISA2, the gloves must be free of contaminants that may pose risks to human health and its safety to the human skin must have been tested.
Cavalcanti et al.3 conducted a study in the dentistry clinics of the State University of Paraíba to assess the frequency of perforations in procedure gloves and found that 15.8% of the gloves were perforated after clinical procedures.
In order to minimize the risks of cross-infection in dentistry, studies that analyze glove perforations after surgical and nonsurgical procedures are necessary. Hence, the objective of the present study was to verify the occurrence of glove perforations after clinical care and the associated factors.
METHODS
This study was conducted by 77 academics of the dentistry program of the State University of Rio Grande do Norte (UERN) who analyzed 279 pairs of gloves, 36 surgical and 243 procedure gloves, used in the dentistry specialties surgery, cosmetic dentistry, endodontics, pediatric dentistry, periodontics, and prosthodontics. This was an observational, cross-sectional study with an inductive approach, using an intensive direct documentation technique in a laboratory.
Before the dental procedures began, the students received two plastic bags, one for the right glove and another for the left glove, along with a form that they should fill out. This form was similar to that created by Cavalcanti et al.3, but some changes were made. The questions included program semester, student role during the procedure (surgeon or assistant), whether the glove was made of latex or vinyl, the student's dominant hand (left or right), dentistry specialty of the procedure, procedure duration, whether the student noticed glove perforation, perforation location (fingers, palm, and back of hand), and whether the skin was injured. We also investigated whether perforation occurred, the perforated hand, the perforated region (back of hand, palm, or fingers), and perforated finger.
At the end of the procedures, a single researcher using full personal protection equipment analyzed the gloves in the wastes room of the dentistry clinics of the university (a room reserved for contaminated material with counters and sinks that facilitate glove analysis and disposal of the solution) as recommended by Xavier et al.4. Each glove was filled with 500 ml of an alkaline fuchsine solution in water (working solution having 0.1% = 0.25g of alkaline fuchsine/100ml of water). Each glove was held at the wrist area and pressured for two minutes to check for leakages on a dark cardboard. Later, the data were transferred to the part of the form reserved for the researcher.
The project was approved by the Research Ethics Committee of UERN under protocol number 121/2011. It was also registered at the National Information System on Human Research Ethics (SISNEP) under number CAAE- 0116.0.428.000-11. The left-handed and right-handed students attending the program's semesters six, eight, and ten who agreed to participate in the study signed an informed consent form.
The database was constructed in the software Statistical Package for the Social Sciences, SPSS, version 21.0 (Chicago, IL, USA). All variables were analyzed descriptively (absolute frequencies and percentages) and by bivariate analysis using the chi-square test. The significance level was set at 5%.
RESULTS
The study included 77 students attending semesters six, eight, and ten of the dentistry program provided by the State University of Rio Grande do Norte (UERN). A total of 279 pairs of gloves were collected, 36 surgical gloves (12.9%) and 243 procedure gloves (87.1%). Of the study participants, 181 pairs of gloves were used by students acting as surgeons (64.9%) and 98, as assistants (35.1%). Thirty-six students were left handed (12.9%) and 243 were right handed (87.1%).
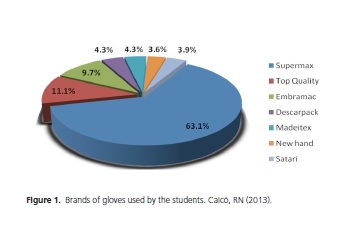
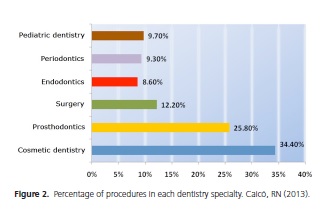
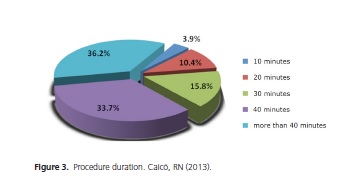
The most popular glove brand was Supermax (63.1%) and the least popular, New Hand (Figure 1). Cosmetic dentistry was the area with the highest number of procedures (96 procedures or 34.4%), followed by prosthodontics (72 procedures or 25.8%) (Figure 2). The area of endodontics involved the smallest number of procedures. Most procedures lasted more than 40 minutes, corresponding to 101 procedures or 36.2% (Figure 3).
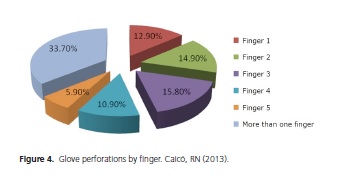
Of the 279 pairs of gloves, 106 had been perforated (38.1%) during the procedures. The dominant hand sustained most of the perforations (47.2); the non-dominant hand sustained 30.2% of the perforations. Both hands were perforated 22.6% of the time. The finger area was the most perforated region, with 60.7% of the perforations, followed by the palm with 29.9%, and the back of the hand with 9.3%. The most perforated finger was finger 3, with 15.8% of the perforations. Most gloves (33.7%) had been perforated in more than one finger (Figure 4).
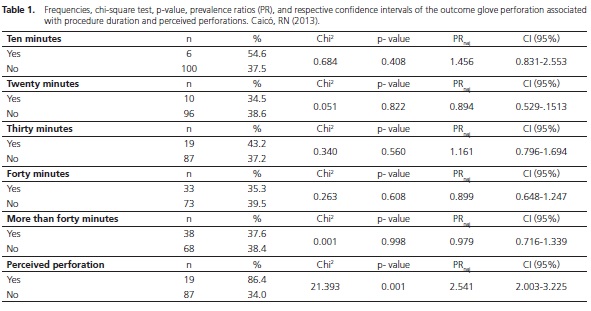
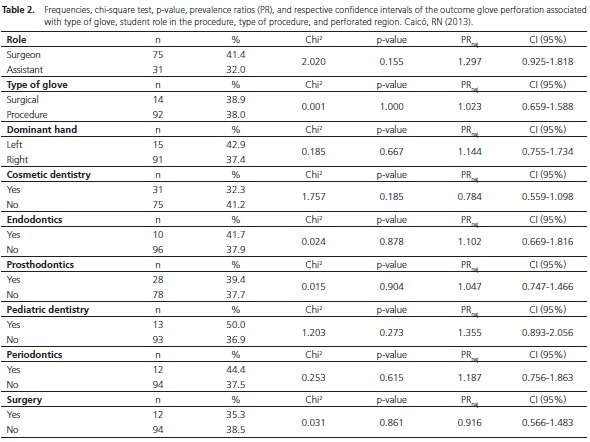
Only 22 students noticed that their gloves had been perforated. Perceived perforations were the only variable associated with the presence of perforations. The occurrence of perforations was indeed greater in individuals who perceived them (PR=2.541 / p-value=0.001) (Table 1). Procedures that involved pediatric dentistry and those that did not involve cosmetic dentistry stood out in inferential analysis. However, these variables were not significantly associated with outcome, that is, the presence of perforations (Table 2). Perforations were also more common in individuals acting as surgeons, but this variable was also not associated with the dependent variable (p-value = 0.155). Of the 106 perforated gloves, 38 had been used in procedures lasting longer than 40 minutes.
DISCUSSION
During professional practice, dentists come in contact with oral tissues, secretions, and blood from surgeries on a daily basis, hence, with a variety of microorganisms present in these locations5. Gloves can prevent contamination of the professional's hand as he touches the patient's oral mucosa, blood, and saliva, and also reduce the risk of transmission of possible microorganisms present on his hand to the patient during dental procedures6-7.
The present study found a higher rate of glove perforations (38.1%) than Oliveira Neto et al.8 (21.3%), Otis & Cottone9 (26.0%), Serratine et al.5 (14.8%), Leal et al.10 (15.6%), Cavalcanti et al.3 (15.8%), Soldá et al.11 (16.3%), and Teixeira et al.12 (10.6%). The study glove area that suffered the greatest number of perforations was the finger area (60.7%), a finding corroborated by Xavier et al.4, Soldá et al.11, Oliveira Neto et al.8, and Leal et al.10.
According to Otis & Cottone9, procedure duration affects the integrity of latex gloves: the number of perforations is significantly greater after two hours of use. In the present study, 101 (36.2%) of the procedures lasted longer than 40 minutes and of these, 38 suffered some kind of perforation. Otis & Cottone9 used a methodology similar to the one used in this study and found that most perforations occurred in the left hand (58%), which is not in agreement with the study finding since 243 participants (87.1%) were right handed. In this study, the dominant hand presented the highest number of perforations at 47.2%.
Laine & Amio13 found that the index finger of the non-dominant hand was the most common perforation site (35.08%), followed by the thumb of the non-dominant hand (18.85%). Burke et al.14 found that the non-dominant hand in oral surgeries were at a higher risk of being perforated. In this study, there was a higher perforation rate in the dominant hand regardless of specialty.
Pitten et al.15 claim that procedure duration and type correlate directly with the perforation index, concluding that perforation propensity increases with procedure duration. According to Guandaline et al.16, 0.7% to 41.3% of unused gloves already contain perforations. Lara17 assessed the visual detection of these defects and concluded that when the glove is not submitted to tension, some small perforations are not detected.
Perceived perforations were the only variable associated with the presence of perforations. Instructions given in pre-clinical disciplines may explain this finding. In a way, students already know how to identify and indeed perceive the existence of perforations. Many factors can compromise glove integrity, such as type of procedure (some specialties use sharper instruments than others), procedure duration, glove brand, and participant's role (surgeon or assistant), factors that have been investigated by this study. Professionals must pay attention to glove quality before and after the procedure to act more correctly and safely towards their team and the patient.
In a way, the absence of more significant findings in the present study may be a reflex of our heterogeneous sample, that is, a sample consisting of students attending different semesters. According to Lima et al.18, experience with occupational accidents increases as students advance in the program. The semester-related increase may also be related to hands-on classes in more clinics and the cumulative hour load of hands-on activities.
CONCLUSION
The present study emphasized the importance of using biosafety measures and assessing personal protection equipment since loss of equipment integrity increases the risk of contamination of the professional, his team, and the patient, contributing to cross-infection between them.
More than one-third (38.1%) of the 279 study glove pairs presented some type of perforation. The dominant hand suffered the most perforations. Cosmetic dentistry procedures and procedures lasting more than 40 minutes were associated with the highest number of perforations. Perceived perforation was the only variable associated with perforation.
Collaborators
TLCS FULLY collected data and helped to write the article. HHA MORAIS supervised the study and helped to write the article. EES LUCENA was responsible for biostatistics and helped to write the article. TGS DIAS supervised the cosmetic dentistry and pediatric dentistry procedures and helped to write the article. JCM BARBALHO supervised the procedures in oral and maxillofacial surgery and helped to write the article. VCF LUCENA supervised the endodontic procedures and helped to write the article.
REFERENCES
1. Brasil. Ministério da Saúde. Controle de infecções e a prática odontológica em tempos de AIDS: manual de condutas. Brasília: Ministério da Saúde; 2000 [citado 2013 Fev 10]. Disponível em: <http://cfo.org.br/wp-content/uploads/2009/10/manual_ conduta_odonto.pdf> [ Links ].
2. Agência Brasileira de Desenvolvimento Industrial. Manual de registro e cadastramento de materiais de uso em saúde / ABDI. Brasília: ABDI; 2011. p. 271-3 [citado 2013 Fev 10]. Disponível em: <http://www.abdi.com.br/Estudo/2%20-%20Manual%20 de%20Registro%20e%20Cadast%20de%20Materiais%20 de%20uso%20em%20Saude.pdf>.
3. Cavalcanti AL, Costa LB, Dantas OAB, Melo E S. Integridade de luvas de procedimentos após atendimento odontológico. POS - Perspect Oral Sci. 2010;2(2).
4. Xavier RL, Vasconcelos BC, da Silva LC, Porto GG. Glove perforation during oral surgical procedures. Med Oral Patol Oral Cir Bucal. 2006;11(5):E433-6.
5. Serratine ACP, Pacheco E, Miero M. Avaliação da integridade das luvas cirúrgicas após a utilização em cirurgias odontológicas. Arq Catarin Med. 2007;36(1):85-9.
6. Wood AJ, Nadershahi NA, Fredekind RE, Cuny EJ, Chambers DW. Student occupational exposure incidence: perception versus reality. J Dent Educ. 2006;70(10):1081-8.
7. Centers for Disease Control and Prevention. Recommended infection-control practices for Dentistry. MMWR Morb Mortal Wkly Rep. 1993;42:1-11.
8. Oliveira Neto JN, Silva LCF, Amaral GB, Oliveira Neto LA, Santos MG. Avaliação dos índices de perfurações em luvas de látex após procedimentos odontológicos. Rev Odontol UNESP. 2009;38(2):79-84.
9. Otis LL, Cottone JA. Prevalence of perfurations in disposable latex gloves during routine dental treatment. J Am Dent Assoc. 1989;118(3):321-4.
10. Leal MHC, Pinheiro JT, Aguiar CM, Leão EC. Avaliação da integridade das luvas de procedimento utilizadas na clínica ortodôntica. RGO - Rev Gaúch Odontol. 2004;52(4):251-5.
11. Soldá SC, Assef JC, Parreira JG, Perlingeiro JAG, Candelária PAP, Cury MP, et al. Perfurações não detectadas de luvas em procedimentos de urgência. Rev Assoc Med Bras. 2009;55(5):597-600.
12. Teixeira AR, Fernandes RA, Serratine ACP. Perfurações em luvas de látex utilizadas em cirurgias odontológicas. Odontol Clín Científ. 2008;7(2):145-50.
13. Laine T, Arnio P. How often does glove perforation occur in surgery? Comparison between single gloves and a doublegloving system. Am J Surg. 2001;181(6):564-6. doi:10.1016/ S0002-9610(01)00626-2
14. Burke FJT, Baggett FJ, Lomax AM. Assessment of the risk of glove puncture during oral surgery procedures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82(1):18-21. doi:10.1016/ S1079-2104(96)80372-6
15. Pitten FA, Herdemann G, Kramer A. The integrity of latex gloves in clinical dental practice. Infection. 2000;28(6):388-92.
16. Guandaline SL, Melo NSFO, Santos ECP. Como controlar a infecção na Odontologia. Londrin: Gnatus; 1997.
17. Lara LCAG. Biossegurança em Odontologia: identificação visual de perfurações em luvas de procedimento. Rev Odonto Ciência. 2002;17(36):183-6.
18. Lima AA, Azevedo AC, Fonseca AGL, Silva JLM, Padilha WWN. Occupation al Hazards: Knowledge, Attitude and Experience of Undergraduate Dental Students of the Federal University of Paraiba, Brazil. Pesq Bras Odontopediatria Clin Integr. 2008;8(3):327-32.
 Correspondence to:
Correspondence to:
Hécio Morais
e-mail: heciomorais@hotmail.com
Received on: 25/3/2014
Final version resubmitted on: 18/6/2014
Approved on: 17/11/2014
