










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.63 no.4 Porto Alegre Out./Dez. 2015
CLÍNICO / CLINICAL
Dental considerations on the management of Idiopathic Thrombocytopenic Purpura in children: case report
Considerações odontológicas no atendimento de crianças com Púrpura Trombocitopênica idiopática: relato de caso
Viviane Ferreira ROSSIERI; Stella Maria Coda Pinto Alves Campos VIEIRAII; Ana Lídia CIAMPONII; Renata de Oliveira GUARÉIII
I Universidade de São Paulo, Faculdade de Odontologia
II Universidade Federal de São Paulo, Programa de Pós-Graduação em Pediatria e Ciências Aplicadas à Pediatria. São Paulo, SP, Brasil
III Universidade Cruzeiro do Sul, Programa de Pós-Graduação em Odontologia. São Paulo, SP, Brasil
ABSTRACT
Idiopathic Thrombocytopenic Purpura (ITP) is a hematological disease characterized by decreased number of blood platelets. Clinically, children with ITP may present petechiae, ecchymoses, haematuria, epistaxis and occasionally hemorrhage. Oral manifestations include spontaneous gingival bleeding, petechiae or hematomas of the mucosa, palate and tongue. It is important for dentists to be aware of ITP in order to properly recognize this condition and offer the adequate treatment to the patient. The aim of this report was, therefore, to relate the case of a 4-yearold patient with acute ITP, to review its main clinical signs in children and describe the management of these patients at the dental office.
Indexing terms: Hemoglobinopathies. Pediatric dentistry. Thrombocytopenic purpura.
RESUMO
Dentre as hemopatias a púrpura trombocitopênica idiopática (PTI) se enquadra no grupo de doenças com alterações plaquetárias e se caracteriza pela diminuição no número de plaquetas do sangue. Clinicamente, crianças com PTI podem apresentar petéquias, equimose, hematúria, epistaxe e ocasionalmente hemorragias teciduais. As manifestações bucais, quando presentes, se caracterizam pelo sangramento gengival espontâneo e petéquias ou hematomas na mucosa, palato e língua. Portanto, é fundamental que o cirurgião-dentista tenha conhecimento sobre a patologia e terapêutica necessária e assim possa determinar o tratamento ideal para estes pacientes. O objetivo do trabalho é relatar o caso de um paciente de 4 anos de idade com PTI aguda, discutir as principais manifestações clínicas em crianças e orientar o cirurgião-dentista para o correto manejo destes pacientes.
Termos de indexação: Hemoglobinopatia. Odontopediatria Purpura. Trombocitopênica.
INTRODUCTION
Hemopathies are categorized in three large groups, according to the nature of the altered hematologic component. Thus, they are divided in disorders that affect erythrocytes (red blood cells), leucocytes (white blood cells) and hemorrhagic disorders, among which are included platelet and coagulation factors alterations1.
Purpura is a disease included in the large group of hemorrhagic disorders and is distinguished by cutaneous hemorrhage and blood loss from mucous membranes and internal organs, which is always related to vascular or platelet alterations2. Thus thrombocytopenia, which is distinguished by the decrease in the number of blood platelets, is included in this large group1,3-9.
Platelets are small granular corpuscles measuring 2 to 4μ in diameter found in the bloodstream. Their role in the coagulation process is the production of a loose aggregate of platelets (temporary hemostatic plug) immediately after a lesion in the blood vessel. This plug is maintained and posteriorly converted into a definite fibrin clot10.
Idiopathic Thrombocytopenic Purpura (ITP) is considered one of the most common disorders in children2,11, and the incidence of asymptomatic illness is approximately 3-8:100,000 children/year12. IPT differential diagnosis must be performed in order to distinguish it from other conditions that may cause the symptoms of thrombocytopenic purpura, such as thrombocytopenia induced by medication (barbiturate, quinine, lengthen therapy with glucocorticoids), hereditary thrombocytopenia . (Bernard-Soulier Syndrome, Aldrich-Schlonlein Syndrome), vitamin C deficiency, viral infections (HIV, infectious mononucleosis), autoimmune disorders (systemic Lupus erythematosus), aplastic anemia, acute leukemia, and non- Hodgkins lymphoma4,11-15.
In laboratorial exams, complete blood count shows severe decrease in platelet count bellow 20,000/ mm3 in acute IPT and between 30,000/mm3 up to 100,000/mm 3 in chronic IPT. In the coagulogram, bleeding time and coagulum retraction are possible alterations6-7,11. The number of white cells is normal and anemia may be present in some cases11.
Currently, IPT is considered an autoimmune disease and its etiology is related to immunological mechanisms such as antibodies and antiplatelet immunoglobulin in the blood16. Genetic studies show the correlation of clinical development of IPT and certain genotypes, suggesting a genetic predisposition and modulation of the illness progression15. IPT is the result of the increment of the destruction of antiplatelet antibodies (autoantibodies) through cells of the reticuloendothelial system, especially the spleen17. The autoantibodies bind to platelets and are eliminated by the spleen, thus the disease severity reflects the balance of the capacity to produce platelets by the bone marrow mega-karyocyte and platelet destruction by the reticuloendothelial system.
IPT is categorized as acute and chronic; the latter is described based on the presence of thrombocytopenia for more than six months before the first signs and symptoms. Acute IPT prevails in children below 10 years old, affecting both genders. It is usually related to a viral infection history before the development of clinical signs with an interval of 2-21 days from the viral infection and the beginning of IPT5,10,14. There are reports that associate the illness to Epstein-Barr infection, varicella zoster infection and, particularly, after rubella vaccination11.
Chronic IPT affects more teenagers than younger children, especially the female gender. There is a greater probability of patients affected by chronic IPT to develop autoimmune diseases, and 1/3 of these patients present laboratorial and clinical symptoms of collagen vascular disease12. Clinical signs of chronic IPT are milder and in some cases they can conceal and hamper the diagnosis6.
IPT clinical symptoms include petechiae, ecchymoses, hematomas, epistasis, hematuria, mucinous cutaneous bleeding and occasionally tissual hemorrhage1,4-6,11,15. In general, splenomegaly doesn't occur, and spleen is only palpable in 10% of the patients with acute IPT. Complications are rare; however intracranial, subglottic, gastrointestinal and genital-urinary hemorrhage may occur11.
Medical treatment for IPT patients adopts different intervening forms, according to individual conditions of each patient given that the immune system of each patient demands up-to-date therapeutics. Asymptomatic children or those whose illness is moderate without severe hemorrhagic episodes can be monitored and don't need specific medicinal therapy. In these cases follow-up without medication intervention is the best form of treatment and success of intermittent controls of platelet count until the disease remission3,17-19. In more severe cases with risks of intracranial, gastro-intestinal and genitourinary hemorrhage, there is the option of platelet transfusion3,11,18-20.
In cases of chronic IPT, in which no success was achieved with all the attempted therapeutic resources, splenectomy3 is recommended, despite its performance restricted success20. In the case of acute IPT in children, there are treatment options with corticoids with high doses of intravenous immunoglobulin doses, and more recently with Anti-D immunoglobulin18,20-21.
Mechanisms of action of corticoids employed in the treatment of acute IPT include the decrease of the antibody-platelet complex clearance and prevention of platelet phagocytosis. High doses of corticoids for a short period are used to increase platelets within 2 to 4 days. The dose ranges from 4mg/kg per day to 30mg/kg of prednisone or methyl prednisone for up to four days. No excessive collateral effects were observed for doses of 4mg/kg per day for four days18-19.
Another treatment option for acute IPT is intravenous immunoglobulins. The most utilized dose is of 0.8 to 1.0/kg/day for 1 or 2 days. In this dosage, it was observed an increase of platelet counts 24 hours after infusion. Collateral effects verified in the usage of intravenous immunoglobulin are headaches, body tremor, fever, nausea, vomit and aseptic meningitis18.
Among the alternatives for the treatment of acute IPT, the anti-D immunoglobulin is the most recent option for children who were not submitted to splenectomy and whose erythrocytes are rhesus-positive. The Anti-D mechanism of action, in spite of its incomplete elucidation, acts on the reduction of platelet clearance18-19. The dosage (50-75μg/kg) favors platelet increase within 24 to 48 hours after its administration. The collateral effects observed include headaches, body tremor, fever, nausea, vomiting and myalgia18. Hemolysis may occur and, consequently, temporary decrease of hemoglobin that in some cases develop hemoglobinemia and /or hemoglobinuria with renal insufficiency, anyhow, it is a rare occurrence18-21.
Despite its tendency to be a benign and self-limited condition, acute and chronic IPT are distinct diseases defined by age, platelet counts, bleeding symptoms and previous acute disease before the diagnosis22.
Regarding buccal health, IPT can frequently bring about buccal mucosa alterations, among which petechiae, ecchymoses and hematomas in areas that are easily traumatized as buccal mucosa, tongue lateral edge and the limit between the hard palate and the soft palate1,4,11. Other IPT findings include spontaneous gingival bleeding, mucocutaneous bleeding4,15 and hemorrhagic vesicles11.
This study objective is to provide guidance to the surgeon-dentist with regards to diagnose and attendance of children with Idiopathic Thrombocytopenic Purpura and a clinical case presentation.
CASE REPORT
The patient, 4 years old, was referred to the Centro de Atendimento a Pacientes Especias (CAPE) [Center for Special Patients Care] at Faculdade de Odontologia da Universidade de São Paulo (FOUSP) with a diagnosis of idiopathic Thrombocytopenic Purpura for odontological follow up. The clinical treatment started after the signature of the Free and Clarified Consent Term for the fulfillment of ethical principles of Helsinki Principle (2000) and Brazilian specific legislation (Figure 1).

During anamnesis it was verified a history of viral infection before the development of IPT symptoms. In the physical exam, petechiae and hematomas were noticed around the knees (Figure 2) and on the forearm. According to the mother, these purple spots developed spontaneously and/or after minor wounds.

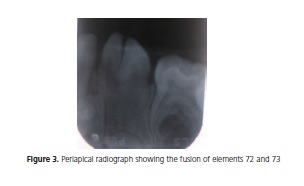
Intra-buccal exam revealed no buccal alterations as the result of IPT. Buccal hygiene of the patient was satisfactory and no dental caries and gingival inflammation were observed. An anterior open bite due to pacifier sucking habit, removed 3 months before the first visit, was found. After the clinical and radiographic exam, it was verified the presence of the fusion of elements 72 and 73 (Figure 3).
Full hemogram analysis of the patient showed the presence of thrombocytopenia (78,000/ mm3) and discreet anemia (Figure 4). The patient was not under medication and was attended by a physician to control IPT.
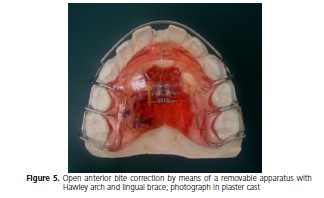
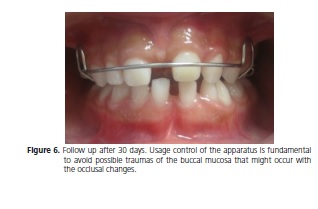
The treatment consisted of nutrition guidance and buccal hygiene for the patient and her guardians, prophylaxis and topic application of fluoridated varnish (Duraphat®, Colgate). For the correction of the open anterior bite, a removable apparatus with Hawley arch and lingual brace (Figure 5) were used. The patient has been under preventive and orthodontic follow-up for 24 months. She has also been submitted to phonoaudiology treatment to promote the development of correct lingual position (Figure 6).
DISCUSSION
IPT is a common childhood disease with low morbidity and mortality, with or without hemorrhage8. Therefore, the surgeon-dentist knowledge with regards to potential alteration caused by this hemopathy is of great importance for dental treatment.
IPT typical signs observed in the patient, as petechiae and hematomas, coincide with the findings in the literature1,4,11,15. However, the patient didn't present the usual symptoms of the disease, as the presence of petechiae, ecchymoses and hematomas on the tongue lateral border and on the limit between the hard palate and the soft palate1,4,11 and, spontaneous gingival bleeding4,15. Such clinical evidences show IPT attenuation, proven by laboratorial tests6.
Medical treatment of patients with IPT assumes different intervention forms in accordance with the clinical conditions observed. Patients affected by IPT in the absence of severe hemorrhage are monitored and don't need specific medicinal therapy3,17-19, a fact which was verified with this patient.
Regarding dental treatment of children affected by ITP, the clinical performance of the odontopediatrician must be based on previous knowledge of the evolution of the patient illness. Appropriate and comprehensive anamnesis is essential, given that sometimes the patients affected by this pathology don't show buccal clinical signs, as the patient herein described. Hence, the illness might not be noticed by the dentist, if the patient's history is not appropriately reported by their parents.
Dental procedures can be performed in patients with platelet counts above 50,000/mm3. In the need of surgical interventions on a patient whose platelet count is too low, blood transfusion or previous corticosteroid treatment is deemed necessary according to medical prescription11. The surgeon-dentist must avoid trauma to the buccal mucosa by carefully puncturing the needles, adapting orthodontic braces and avoiding super-activation4. Prescription of antiplatelet drugs, such as acetylsalicylic acid and ibuprofen, must be avoided.
Appropriate control of dental biofilm is of the utmost importance, in order to prevent gingival inflammation and infections. Individual protocols for prevention of caries must be established according to caries risk and age of each patient. If there is the need for restoration treatments, endodontic and surgical treatment, antibiotics prophylaxis can be performed to reduce the risk of postoperative infections11.
The treatment of children with IPT must involve an interdisciplinary approach in which the odontopediatrician works together with the hematologist physician.
CONCLUSION
Hematological diseases present physical and buccal alterations that are considered important clinical signs for their diagnosis, as buccal mucosa alterations among which petechiae, ecchymoses and hematomas. Notwithstanding, these clinical signs are rare and the professional must be able to recognize Idiopathic Thrombocytopenic Purpura after a critical anamnesis aimed at providing guidance and effective treatment of the patients, as well as refer them to the physician.
Collaborators
VF ROSSIER provided clinical attendance to the patient and participated in the article writing. SMCPAC VIEIRA was responsible for the orthodontic assessment and orthodontic attendance and participated in the article writing. AL CIAMPONI was responsible for the conception and drawings of the clinical case and participated of the article writing. RO GUARÉ was in charge of the analysis of clinical data and participated of the article writing.
REFERENCES
1. Barnard K, Smallridge J. Recognizing and caring for the medically compromised child: 2. Haematological disorders. Dent Update. 1998;25(9):402-10. [ Links ]
2. Almeida TV. Púrpuras. In: Marcondes E. Pediatria básica. 7a ed. São Paulo: Sarvier; 1988. p. 1348-53.
3. George JN, Kojouri K, Perdue JJ, Vesely SK. Management of patients with chronic, refractory, idiopathic thrombocytopenic purpura. Semin Hematol. 2000;37(3):290-8.
4. Hunter ML, Hunter B, Lesser L. Acute idiopathic thrombocytopenic purpura in childhood: report of a case presenting in general practice. Br Dent J. 1997;183(1):27-9. doi: 10. 2174/1874210601408010164
5. James WD, Guiry CC, Grote WR. Acute idiopathic thrombocytopenic purpura. Oral Surg. 1984;57:149-151.
6. Linenberg WB. Idiopathic Thrombocytopenic purpura. Oral Surg. 1964;17(1):22-30.
7. Thoma KH, Holland DJ, Woodbury HW, Sleeper. Thrombocytopenic purpura associated with bleeding from the gingiva. Oral Surg. 1948;1(1):12-6.
8. Watts RG. Idiopathic thrombocytopenic purpura: a 10- year natural history study at the children hospital of Alabama. Clin Pediatr (Phila). 2004;43(8):691-702. doi: 10. 1177/000992280404300802
9. Pinto LAM, Pansani CA, Giro EMA, Lima FCBA, Costa JH. Púrpura Trombocitopênica. RGO, Rev. Gaúch Odontol. 1990;38(4):280- 1.
10. Ganong WF. Fluidos circulantes do organismo. In: Ganong WF. Fisiologia médica. 3ª ed. São Paulo: Atheneu; 1977. p. 385-99.
11. Vaisman B, Medina AC, Ramirez G. Dental treatment for children with chronic idiopathic thrombocytopaenic purpura: a report of two cases. Int J Paediatr Dent. 2004;14(5):355-62. doi: 10. 1111/j. 1365-263X. 2004. 00541. x
12. Chu YW, Korb J, Sakamoto, KM. Idiopathic thrombocytopenic purpura. Pediatrics Rev. 2000;21:95-104.
13. Bolton-Maggs PHB. Idiopathic thrombocytopenic purpura. Arch Dis Child. 2000;83:220-2.
14. Lowe EJ, Buchanan GR. Idiopathic thrombocytopenic purpura diagnosed during the second decade of life. J Pediatr. 2002;141(2):253-8. doi:10. 1067/mpd. 2002. 125909
15. Özsoylu S, Karabent A, Irken G, Tuncer M. Antiplatelet antibodies in childhood idiopathic thrombocytopenic purpura. Am J Hematol. 1991;36(2):82-5. doi: 10. 1002/ajh. 2830360203
16. Ripamonti U, Petit JC, Penfold G, Lemmer J. Periodontal manifestations of acute autoimmune thrombocytopenic purpura. J Periodontol. 1986;57(7):429-32. doi: 10. 1902/jop. 1986.57.7.429
17. Rischewski JR, Imbach P, Paulussen M, Kühne T. Idiopathic Thrombocytopenic Purpura (ITP): is there a genetic predisposition? Pediatr Blood Cancer. 2006;47:678-80. doi: 10. 1002/pbc. 21005
18. Blanchette V, Carcao M. Approach to the investigation and management of immune thrombocytopenic purpura in children. Semin Hematol. 2000;37(3): 299-314.
19. Panepinto JA, Brousseau DC. Acute idiopathic Thrombocytopenic purpura of childhood- Diagnosis and Therapy. Pediatr Emerg Care. 2005;21(10):691-6.
20. El-Alfy MS, Mokhtar GM, EL-Laboudy MAM. Randomized trial of Anti-D immunoglobulin versus low-dose intravenous immunoglobulin in the treatment of childhood chronic idiopathic thrombocytopenic purpura. Acta Haematol. 2006;115(1-2):46- 52. doi: 10. 1159/000089465
21. Gebauer E, Vijatov G. Idiopathic thrombocytopenic purpura in children. Med Pregl. 1998;51(3-4):127-34.
22. Tarantino MD, Bolton-Maggs PHB. Update on the management of immune thrombocytopenic purpura in children. Curr Opin Hematol. 2007;14(5):526-34.
23. Glanz J, France E, Xu S, Hayes T, Hambidge S. A populationbased, multisite cohort study of the predictors of chronic idiopathic thrombocytopenic purpura in children. Pediatrics, 2008;121(3):e506-12. doi: 10. 1542/peds. 2007-1129.
 Correspondence to:
Correspondence to:
VF ROSSIER
e-mail: virossier@uol.com.br
Received on: 1/4/2013
Final version resubmitted on: 18/11/2013
Approved on: 17/2/2014
