










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.7 no.3 Joinville Set. 2010
ORIGINAL RESEARCH ARTICLE
Prevalence of aggressive periodontitis among Yemeni students from schools in the city of Thamar
Abdullah Gh. ImranI; Mansour Ali S. AtaaII
IDepartment of Dentistry, Thamar University – Thamar – Yemen
IIDepartment of Dentistry, Sana'a University – Sana'a – Yemen
ABSTRACT
INTRODUCTION AND OBJECTIVE: Aggressive periodontitis (AgP) is a type of periodontitis that causes rapid destruction of alveolar bone, especially in young ages. In Yemen, there is no previous study about aggressive periodontitis, so the aim of this study was to assess the prevalence and related risk factors for aggressive periodontitis among school students in the city of Thamar.
MATERIAL E METHODS: In this study, a two-stage sampling method was used. At first stage, a random sample of eight public schools was selected from the schools of the city of Thamar by simple random sampling. In the second stage, a sample of 807 students (458 female and 349 male) was drawn from the chosen schools by simple random sampling. People aged from 10 to 22, with mean age of 17. The classification considered in the current paper was based on the American Academy of Periodontology classification of 1999. A questionnaire was applied and included questions that would give information about the risk factors that might be considered causal factors for aggressive periodontitis.
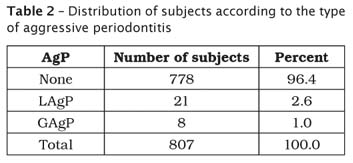
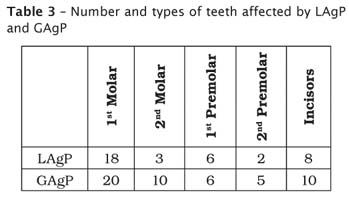
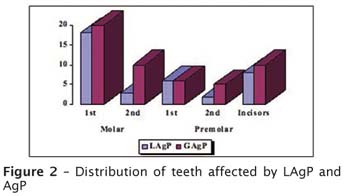
RESULTS: The number of affected students with AgP was 29 among 807 students, that is, 3.6% of the sample. The percentages of localized aggressive periodontitis (LAgP) and generalized aggressive periodontitis (GAgP) were, respectively, 2.6% (21 students) and 1.0% (8 students). The following teeth were found to be affected: first molars, second molars, incisors, first premolars and second premolars. In GAgP, 20 first molars, 22 incisors, 6 first premolars, 3 second molars and 2 second premolars showed clinical attachment loss. But in LAgP, 18 first molars, 19 incisors, 6 first premolars, 3 second molars and 2 second premolars showed clinical attachment loss. With regards to the risk factors – socioeconomic level, age, poor oral hygiene status, plaque index and gingival bleeding –, the statistical results indicated that each of these factors showed highly significant relationships with AgP.
CONCLUSION: The prevalence of AgP among Yemeni schools students was relatively high: 3.6%. This might be related to the low socioeconomic level and poor oral hygiene status of most of the Yemeni students.
Keywords: aggressive periodontitis; risk factors; alveolar bone loss; logistic regression.
Introduction
Periodontitis is a loss of supporting connective tissue and alveolar bone around teeth [10]. The terms "early-onset periodontitis" (EOP) and "juvenile periodontitis" (JP) were replaced by that of "aggressive periodontitis" (AgP) according to the classification of periodontal diseases and conditions in 1999 [24]. Aggressive periodontitis differs from the chronic form by the rapid rate of disease progression seen in, an otherwise healthy individual, an absence of large accumulation of dental plaque and calculus. This form of periodontitis usually affects young people at or after puberty, and thus can be observed during the second and third decade of life.
The disease may be localized, as described for localized juvenile periodontitis (LJP), or generalized, as was previously described for generalized juvenile periodontitis (GJP) and rapidly progressive periodontitis (RPP) [12]. Localized aggressive periodontitis (LAgP) is characterized by affecting at least one first molar and one incisor with proximal attachment loss on at least two permanent teeth, one of which is a first molar that has more than 3 mm of attachment loss.
In generalized aggressive periodontitis (GAgP), the proximal attachment loss affects at least three teeth other than first molars and incisors. In this case, teeth have more than 3 mm of attachment loss [6]. Radiologically, the destruction of alveolar bone appears as arc-shaped bone loss in the molar region and as horizontal bone loss in the incisors, besides appearing as bilateral symmetrical patterns of bone loss in the molar region. The degree and the shape of the bone loss are generally dependent upon whether the lesion is diagnosed in an early or advanced stage. At the terminal stage of the disease, the bone loss is no longer vertical in nature, but it assumes a horizontal shape [7, 13].
There are many risk factors that could be considered as causal factors for aggressive periodontitis. Risk factors may be modifiable or non-modifiable. Modifiable risk factors are usually environmental or behavioral in nature, whereas non-modifiable risk factors are usually intrinsic to the individual, and therefore will not easily be changed. Non-modifiable risk factors are also known as determinants.
It was believed that all individuals were uniformly susceptible to developing periodontal disease and that accumulation of plaque, poor oral hygiene and perhaps occlusal trauma were sufficient to initiate periodontitis. However, during the past four decades, it has become accepted that periodontal disease is caused by specific bacterial infections, and those individuals are uniformly susceptible neither to these infections nor to the damage caused by them [22]. It has been suggested that the low socioeconomic level is considered a positive risk factor for development of aggressive periodontitis. Besides, smoking is considered the more established of the modifiable risk factors for periodontal disease [5].
Cross-sectional and longitudinal data provide strong support for the statement that the risk of developing periodontal disease, as measured by clinical attachment loss and alveolar bone loss, increases with increased smoking [23]. Some epidemiological studies in the literature have clearly demonstrated that the prevalence, extent and severity of periodontal attachment loss used to increase with age [2].
Gender may also be considered as a risk factor for periodontal disease. There are some epidemiological studies that have consistently shown that the periodontal disease and periodontal tissue loss are more prevalent in females than in males, and this might be related to the earlier eruption of first molars and incisors in females [4]. The effect of gender as a risk factor for aggressive periodontitis and the exact mode of inheritance of the disease remain unclear.
The available evidence from the literature suggests that, at the circumpubertal age, young females might be more predisposed than males, and this effect decreases with increasing age [12]. Other studies have also demonstrated that individuals under psychological stress are more likely to develop clinical attachment loss and loss of alveolar bone [13]. One possible link in this regard may be referred to the increases in the production of IL-6 in response to increased psychological stress [15]. However, some studies indicated that race/ethnicity groups are associated with a significantly higher risk of developing early-onset periodontitis, by having both the aggressive and chronic form [15].
The non-modifiable risk factors that may play a very important role in the development of periodontitis of either chronic or aggressive forms are genetic factor, host response and osteoporosis [16]. For comparative reasons, we introduce the results of some previous studies which were devoted to asses the prevalence of periodontitis among population of different communities, e.g., in an urban population in southern Brazil, the prevalence of AgP among 612 subjects aged 14 to 29 years was 5.5% [21]. In some other countries, the prevalence of AgP was as follows: 2.7% in Syria [14], 0.1% in Switzerland [16], 0.32% in Chile [18], 0.13% LJP and 1.61% GJP in the United States of America [17], 0.42% in Saudi Arabia [19]. Moreover, the prevalence of LAgP among young Turkish population was reported to be 0.6%, and the ratio of females to males was 1.25:1 [8].
Thus, the aim of this study was to assess the prevalence of aggressive periodontitis among school students in the city of Thamar, based on some risk factors which are considered to be a determinant for this disease.
Material and methods
In this study, a two-stage sampling method was used. At first stage, a random sample of eight public schools was selected from the schools of the city of Thamar by simple random sampling. In the second stage, a sample of 807 students was drawn from the chosen eight schools by simple random sampling. The sample size was estimated to have significant numbers for statistical analysis. The sample was randomly chosen from eight schools of basic education level (5th to 9th grade) and secondary education level (11th to 12th grade) in the city of Thamar. The selected sample was of 807 students, comprising 349 males and 458 females, aged from 10 to 22 years. Prior to visiting the chosen schools, an approval of the Administration of Education in Thamar Governorate was obtained.
The purpose of the study was, subsequently, explained to both school authorities and students. Once the participation of the students in the study was approved, they were sent to the prepared room for examination by the researcher, during their spare time. The information and data were registered in a special questionnaire designed to include important information that would help us to detect the correlation between aggressive periodontitis and some risk factors, comprising the age of the student, gender and oral hygiene, as well as local factors associated with provision of dental care, smoking, socioeconomic level and the general health of the student. Moreover, the level of education of the student's parents and the history of the student's oral health, as well as the history of his/her family's oral health, was asked. The people that constituted the sample of this study were free from systemic diseases such as diabetes, osteoporosis and heart diseases, and anyone that had been affected by one or more of these diseases was excluded.
Clinical examination
All clinical examinations were carried out by the examiner. The examination of the following six sites per tooth of the mandibular and maxillary permanent teeth was performed: mesio-lingual, mid-buccal, disto-buccal, disto-lingual, mid-lingual and mesio-lingual. The assessments of periodontal parameters included in the examination were plaque index [20] and gingival bleeding, which was done by bleeding on probing index with two scores, coded as 0 for no bleeding and 1 for the presence of bleeding after 30 seconds of probing pocket depth > 5mm.
Loss of attachment was assessed by using William's Periodontal Probe (Zafero), which was introduced by Glavined and Löe [9], and performed as follows: (a) measuring the distance (in mm) from the free gingival margin (FGM) to the cemento-enamel junction (CEJ); (b) measuring the distance from the FGM to the bottom of sulcus or pocket at each site; (c) the attachment loss was obtained by subtracting the first measurement from the second one [17].
The students having 2 or more teeth of 5 mm or deeper pockets were invited for panoramic x-ray and periapical radiographic examination in the Faculty of Dentistry, Thamar University. Before the beginning of clinical examination, the examiner examined ten of the students. He examined these parameters: plaque index, gingival bleeding and clinical attachment loss. After one week, examination was rebated by the examiner himself for calibration (Intra-examiner calibration); the percentage of calibration considered here was 94%.
Results
Data analysis was carried out using simple logistic linear models. The response variable is the aggressive periodontitis (AgP), which is a binary response variable coded as 0 for affected and 1 for non-affected student. The following independent variables were considered in this study: age (years), gender, father's education level (Felevel), mother's education level (Melevel), father's job (Fathjob), mother's job (Mothjob), socioeconomic level, family size, toothbrush use, use of toothpicks or dental floss. Plaque index, gingival bleeding, pocket depth and loss of attachment were evaluated during the clinical examination.
The analysis results for testing the relationship between AgP and either of these risk factors considered in this study were obtained by simply fitting AgP to each of these risk factors taken one at a time. The statistical analysis results are displayed in Table 1.
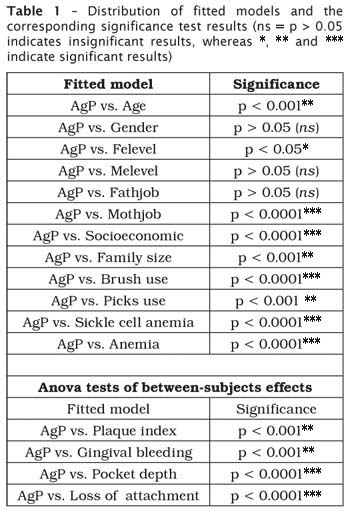
The results obtained indicated that the age of the student was found to be significantly associated with AgP (p < 0.001). On the other hand, the gender of the student was found to be insignificant for showing a poor relationship with AgP (p > 0.05). With regards to parents' education level, the results indicated that the father's education level appeared to be significantly related to AgP (p < 0.05), while the mother's education level was not related to AgP (p > 0.05).
The relationship between parents' job and occurrences of AgP were also investigated using Chi-square test. The results obtained yielded a strong association between mother's job and AgP (p < 0.0001), but father's job was not significantly related to the occurrence of AgP (p > 0.05).
The study has clearly demonstrated that there is a strong relationship between the socioeconomic level of the student and the prevalence of AgP (p < 0.0001). The study also indicated that the prevalence of AgP among students from poor families is significantly higher than that occurred among students from rich families. Furthermore, the family size was found to be a significant risk factor in determining the prevalence of AgP.
Results obtained indicated that the number of students who were affected by AgP was higher in families with more than ten members. For oral hygiene care, more than a half of the sample (408) responded that they have never used a toothbrush. Out of those 408 students, there were 22 students who were found to be affected by AgP. From the data records, there were 312 students who were found to use a toothbrush more than once per day and 58 students who used toothbrush for only once per week.
The Chi-square test of whether or not the use of toothbrush is significantly associated with AgP yielded that the use of toothbrush when tested against incidence of AgP was significant (p < 0.0001).
For local risk factors as represented by dental plaque, gingival bleeding and bleeding on probing, the data study consists of 448 students with score 2 of dental plaquew, 229 students with score 1, 110 students with score 3 and 19 students with score 0. Anova test was applied to test the dental plaque against AgP, and the results obtained were found to be highly significant (p < 0.0001).
Gingival bleeding was classified into two categories: 0 for no bleeding and 1 for bleeding on probing. There were 634 students with score 1 and 173 students with score 0. Thus, the Anova test showed that gingival bleeding was significantly associated with the occurrence of AgP (p < 0.001). The Anova test also showed that pocket depth and loss of attachment were significantly associated with AgP (p < 0.0001).
With regards to smoking as a risk factor, there were only 50 smokers in the sample, and the other 757 students were non-smokers. Chi-square test yielded that there is no relationship between smoking and occurrences of AgP.
In order to evaluate the medical history, each participant was asked if he/she had a history of one or more systemic disease such as diabetes, asthma, heart disease, sickle cell anemia, anemia, rheumatoid arthritis etc. In this study, there were 4 students with a history of sickle cell anemia and 8 students with a history of anemia, and all of them were affected by AgP. Hence, the Chi-square test showed significant results regarding the association of sickle cell anemia with AgP (p < 0.0001).
Tables 2 and 3 show, respectively, the distribution of LAgP and GAgP and the number of teeth affected by LAgP and GAgP. As we can see in Table 2, the percentages of LAgP and GAgP forms are, respectively, 2.6% and 1.0%. Table 3 shows that the following teeth were found to be affected: first molars, second molars, incisors, first premolars and second premolars. As we can see in Table 3, the highest number of teeth with affected by LAgP and GAgP are first molars and incisors, respectively, whereas the lowest numbers are those of second molars and second premolars.
Figures 1 and 2 show, respectively, the distribution of subjects according to the type of aggressive periodontitis and the types of teeth affected by LAgP and GAgP (1st and 2nd molars, 1st and 2nd premolars and incisors).
Discussion
Because there is no previous study about aggressive periodontitis in Yemen, this present study is considered the first one performed among Yemeni students in the city of Thamar, in Yemen. This study demonstrated that the prevalence of aggressive periodontitis was 3.6% among 807 students, a relatively high result in comparison to other previous studies conducted in other countries [8, 14, 16, 17, 18, 19]. Such result might be related to the low socioeconomic level of the students in Yemen. Moreover, the first molars and incisors were the ones more affected by loss of attachment, and this may be related to the earlier eruption of these teeth.
With regards to risk factors thought to be related to the development of aggressive periodontitis, the Chi-square test indicated that the younger age of the student was found to be significantly associated with AgP (p < 0.001).
Even tough some epidemiological studies have shown that the prevalence of periodontal disease is often higher among young females, which might be related to their earlier eruption of first molars and incisors [3], the current study concluded that there is no significant difference between males and females (p > 0.05).
The current study indicated that there is a strong relationship between the low socioeconomic level and the prevalence of aggressive periodontitis among Yemeni students (p < 0.001). This result might be due to the increasing number of the family members (p < 0.001). Because most students' mothers have no job, the mother's job factor was found to be significantly associated with AgP (p < 0.0001).
Thus, the results obtained for the considered risk factors have clearly demonstrated that the prevalence of AgP among students from poor families is higher in comparison to rich families. Moreover, this result suggests that the low socioeconomic level is considered a positive risk factor for the development of aggressive periodontitis. This conclusion agrees with results drawn from previous epidemiological studies [22].
It can be noted that oral hygiene status may play an important role in the occurrence of AgP, as this study yielded that the prevalence of AgP among students who are not using toothbrush is much higher than among those students who are usually using toothbrush (p < 0.0001). This might be due to the increasing accumulation of some local factors, such as dental plaque and calculus that contribute to the development of gingival inflammation, and therefore these local factors may increase the percentage of occurrence of AgP.
Although some previous studies indicate that there is a strong relationship between periodontitis and smoking [5, 23], the current study provided insignificant relationship between AgP and the smoking factor. This may be due to the fact that only a few number of students in the sample were smokers (50 out of 807 students).
Considering the medical history of some systemic diseases, the study showed a significant relationship between the occurrence of AgP and those students having a history of anemia and/or sickle cell anemia (p < 0.0001). This might be due to severe iron and B12 deficiency that are associated with anemia, which leads to aggressive periodontitis. This study, however, indicated that there is no significant relationship between AgP and the other medical history of diabetes, rheumatoid arthritis, heart diseases etc. (p > 0.05). Such a result might be related to the absence of these systemic diseases among the sample of students that participated in this study.
Conclusion
The prevalence of AgP among Yemeni schools students was 3.6%. Low socioeconomic level and poor oral hygiene may play a very important role in the development of aggressive periodontitis and its increasing prevalence.
References
1. Albandar JM, Brown LJ, Löe H. Clinical features of early-onset periodontitis. J Am Dent Assoc. 1997;128(10):1393-9. [ Links ]
2. Albandar JM, Brunelle JA, Kingman A. Destructive periodontal disease in adults 30 years of age and older in the United States, 1988-1994. J Periodontol. 1999;70(1):13-29. [ Links ]
3. Albandar JM, Muranga MB, Rams TE. Prevalence of aggressive periodontitis in school attendees in Uganda. J Clin Periodontol. 2002;29:823-31. [ Links ]
4. Albandar JM, Rams TE. Risk factors for periodontitis in children and young persons. Periodontol 2000. 2002;29:207-22. [ Links ]
5. Albandar JM, Streckfus CF, Adesanya MR, Winn DM. Cigar, pipe, and cigarette smoking as risk factors for periodontal disease and tooth loss. J Periodontol. 2000;71:1874-81. [ Links ]
6. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999;4(1):1-6. [ Links ]
7. Baer PN. The case for periodontosis as a clinical entity. J Periodontol. 1971;42:516-20. [ Links ]
8. Ereş G, Saribay A, Akkaya M. Periodontal treatment needs and prevalence of localized aggressive periodontitis in a young Turkish population. J Periodontol. 2009 Jun;80(6):940-4. [ Links ]
9. Glavind L, Löe H. Errors in the clinical assessment of periodontal destruction. J Periodontal Res. 1967;2(3):180-4. [ Links ]
10. Haubek D, Ennibi OK, Poulsen K, Vaeth M, Poulsen S, Kilian M. Risk of aggressive periodontitis in adolescent carriers of the JP2 clone of Aggregatibacter (Actinobacillus) actinomycetemcomitans in Morocco: a prospective longitudinal cohort study. Lancet. 2008 Jan;371(9608):188-9. [ Links ]
11. Hugoson A, Ljungquist B, Breivik T. The relationship of some negative events and psychological factors to periodontal disease in an adult Swedish population 50 to 80 years of age. J Clin Periodontol. 2002 Mar;29(3):247-53. [ Links ]
12. Ishikawa I, Kawashima Y, Oda S, Iwata T, Arakawa S. Three case reports of aggressive periodontitis associated with Porphyromonas gingivalis in younger patients. J Periodontal Res. 2002;37(5):324-32. [ Links ]
13. Kayalibay H, Gnanesekhar DJ. Juvenile periodontitis: a case report. J Islamic Academy of Sciences. 1989;2(2):131-4. [ Links ]
14. Kazem M, Albandar JM. Risk indicators of aggressive periodontitis in Syrian adolescents. J Clin Periodontol. 2006;33(7):765-73. [ Links ]
15. Kiecolt-Glaser JK, Preacher KJ, MacCallum RC, Atkinson C, Malarkey WB, Glaser R. Chronic stress and age-related increases in the proinflammatory cytokine IL-6. Proc Natl Acad Sci USA. 2003;100(15):9090-5. [ Links ]
16. Kronauer E, Borsa G, Lang NP. Prevalence of incipient juvenile periodontitis at age 16 years in Switzerland. J Clin Periodontol. 1986;13(2):103-8. [ Links ]
17. Löe H, Brown LJ. Early onset periodontitis in the United States of America. J Periodontol. 1991 Oct;62(10):608-16. [ Links ]
18. Lopez NJ, Rios V, Pareja MA, Fernandez O. Prevalence of juvenile periodontitis in Chile. J Clin Periodontol. 1991;18(7):529-33. [ Links ]
19. Nassar MM, Afifi O, Deprez RD. The prevalence of localized juvenile periodontitis in Saudi subjects. J Periodontol.1994;65(7):698-701. [ Links ]
20. Silness J, Löe H. Periodontal disease in pregnancy. Acta Odontol Scand. 1964;22:121. [ Links ]
21. Susin C, Albandar JM. Aggressive periodontitis in an urban population in southern Brazil. J Periodontol. 2005;76(3):468-75. [ Links ]
22. Van Dyke TE, Dave S. Risk factors for periodontitis. J Int Acad Periodontol. 2005;7(1):3-7. [ Links ]
23. Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings from NHANES III – National Health and Nutrition Examination Survey. J Periodontol. 2000;71:743-75. [ Links ]
24. Tonetti MS, Mombelli A. Early-onset periodontitis. Ann Periodontol. 1999;4:39-52. [ Links ]
 Address for correspondence:
Address for correspondence:
P.O. BOX: 87246
Thamar, Yemen
E-mail: yaser2002m@yahoo.com
Received on January 6, 2010
Accepted on April 12, 2010
