










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.1 Joinville Jan./Mar. 2012
CASE REPORT ARTICLE
Periapical cemento-osseous dysplasia: case report
Francine Sumie Morikava I; Ligia Yumi Onuki I; Cassiano Lima Chaiben I; Maria Helena Martins Tommasi I; Iran Vieira I; Antonio Adilson Soares de Lima I
I School of Dentistry, Department of Stomatology, Federal University of Paraná – Curitiba – PR – Brazil
ABSTRACT
Introduction: Periapical cemento-osseous dysplasia is a pathologic entity resulting from bone and cementum reactional process which affects the periapical region of the anterior mandible. Its etiology is not fully understood, but possibly it is related to an unusual bone and cementum response to some local factor. Objective: The aim of this study is to present a case of periapical cemento-osseous dysplasia. Case report: A 50 years-old female patient sought for dental care due to pain in the lower right premolar region. The panoramic radiography revealed the presence of an extensive radiolucent lesion with radiopaque areas located between the roots of the teeth #43 and #35. Teeth presented vitality and it was not observed any changes involving the periodontal ligament. Periapical cemento-osseous dysplasia diagnosis was established through clinical and radiographic features. Periapical cemento-osseous dysplasia does not require any treatment unless complications occur. Patient's complaint of discomfort was related to occlusal imbalance and was solved after the occlusion reestablishment. The patient was radiographically followed-up for 12 months and the lesion exhibits satisfactory signs of healing. Conclusion: The dentists need to be aware of asymptomatic intra-osseous lesions affecting the anterior region of mandible not to misconduct the diagnosis that could compromise the patient's oral health.
Keywords: mandible; tooth cementum; panoramic radiograph; periapical tissue.
Introduction
Osseous dysplasia is defined as a reactional and non-neoplasic process developing in periapical tooth area and characterized by normal bone replacement by fibrous tissue and metaplastic bone. This pathological alteration can assume several clinical forms and therefore receive different denominations 22. When such process occurs in the periapical area of mandible's anterior teeth, is so-called periapical cemento-osseous dysplasia. However, other terms have been used for this pathological entity, such as: cementum's periapical dysplasia, periapical cemental dysplasia, focal cemento-osseous dysplasia, periapical osseous dysplasia, and periapical cementoma 14,21,23.
According to the classification proposed by Eversole et al. 6, among the large spectrum of osseous lesions, there is a group of entities so-called cemento-osseous dysplasias comprising focal cemento-osseous dysplasia and florid cemento-osseous dysplasia. For this authors, periapical cemento-osseous dysplasia or focal cemento-osseous dysplasia are two different terms for the same reactive lesion. However, the World Health Organization's most recent tumor classification says that periapical cemento-osseous dysplasia is a condition related to osseous lesions 2.
The etiology and pathogenesis of this entity are still unknown. On the other hand, clinical and histological evidences show this condition has a histogenetic origin derived from the periodontal ligament 29. Periapical cemento-osseous dysplasia exhibits a predilection for melanoderm women, at mid-age (40-50 age-range) and rarely below 20 years-old 4,27. Mandible's periapical area is the most common site of appearance; frequently multiple sites are affected (root apex of two or more teeth). A radiographic study performed by Su et al. 27 revealed that the lesions' mean size is about 1.8 cm, ranging from 0.2 to 11 cm. Additionally, although the lesions are close to the tooth apex, the periodontal ligament remains clearly visible in radiographs 9.
Periapical cemento-osseous dysplasia is a self-limiting problem because the osseous cortex is not expanded and progressive growth is rare. Its prevalence is difficult to be determined because it is an asymptomatic lesion and there is not the need of a biopsy to prove the diagnosis 14. In 1934, Stafne conducted a radiographic study in a sample of 10,000 patients and found a prevalence of 0.24%. Neville et al. 15 observed a prevalence of 5.9% of periapical cemento-osseous dysplasia in Black women. Vicci & Capelozza 30 determined the occurrence of tooth and osseous lesions by using the image of panoramic radiographs. This study revealed the prevalence of periapical cemento-osseous dysplasia was 1.8%. In 2008, Pereira et al. 18 performed a similar study and found a prevalence of 1% for this disease.
Periapical cemento-osseous dysplasia has a natural evolutional path in which changes in the pathology's features are noted. Traditionally, this evolution can be divided into three stages: osteolytic, cementoblastic and mature. However, Langlais et al. 11 believed that there would be two additional stages: a more early osteoporotic stage in all cases and a later florid stage in some cases. The replacement of osseous tissue by fibrous tissue is characterized by a radiolucent image at the tooth apexes, indicating the osteolytic stage of its development. As the condition progresses, the radiolucent lesion assumes a mixed pattern due to an increase of the cementoblastic activity leading to cementum spicules deposition. These aspects characterized the cementoblastic stage of the development. At the mature stage, periapical cemento-osseous dysplasia is a solid opaque mass, frequently surrounded by a radiolucent halo, due to its complete maturation. This process can take months or years to occur 14.
Due to the nature and evolution of this lesion, no treatment is necessary. Because the teeth remain vital, tooth extraction or endodontic treatment should not be performed On the other hand, regular following-up examinations are recommended comprising dental prophylaxis and oral hygiene instruction reinforcement to prevent periodontal disease and caries lesions which can lead to tooth loss 16. The aim of this study is to describe a case of a patient diagnosed with periapical cemento-osseous dysplasia based on the clinical and radiographical findings.
Case report
A 50-year-old, melanoderm patient sought for the Semiology Clinics of the School of Dentistry of Federal University of Parana due to a complain of discomfort at the area of tooth #44, #45, and #46, where implants had been installed two years ago.
During clinical examination, it could be noted the presence of caries lesions, gingival retraction, periodontal pocket at tooth #17 and a nodular lesion in lower lip whose diagnosis was fibrous hyperplasia. This lesion underwent an excisional biopsy and the anatomic-pathological examination confirmed the diagnosis.
To evaluate the origin of the patient's discomfort, oral examination, panoramic and periapical radiographs of the region were done. The radiographs revealed that the area where the implants had been installed did not show any significant alteration. Therefore, the patient was referred to the Periodontics Clinics for a more detailed assessment. Because no radiographic alteration involving the implants was seen, patient's periodontium and occlusion was checked. Periodontal examination did not find any contributory finding, but the occlusion examination revealed a premature contact in the prosthesis installed on the implant at the area of tooth #45. Patient's occlusion was reestablished through weariness with burs and polishing of the amalgam restoration in the antagonist tooth. The anterior teeth and the implants were submitted to root scaling, planing and polishing. Additionally, patient was instructed to improve her oral hygiene. At the following appointment, one week later, patient reported that her discomfort had stopped.
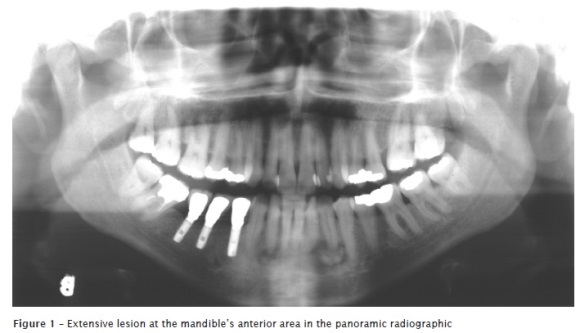
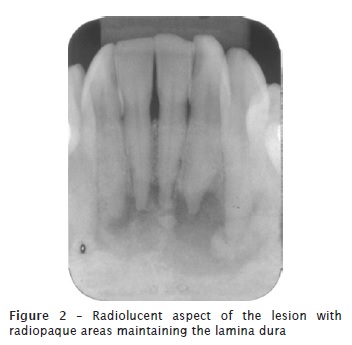
Notwithstanding, during the analysis of the panoramic radiographic, it was observed an extensive lesion of radiolucent aspect comprising areas of radiopacity within it, which was located at the area close to the lower incisors and radiographiccanine teeth (figure 1). Periapical radiographs were executed and showed that the lamina dura surrounding the apical area of the involved teeth was preserved (figure 2).
The patient was not aware about the presence of intra-osseous lesions and did not feel any discomfort in the area. The physical examination of the mucosa revealed that there was not any volume increase and that the periodontal tissues were normal (figure 3). All teeth in this area were submitted to thermal test, which responded positively demonstrating that tooth vitality was preserved. Vertical percussion test was also conducted, and the patient did not report any discomfort. The diagnosis of periapical cemento-osseous dysplasia was established based on the lack of symptomatology and on the clinical and radiographic aspects of the lesion (melanoderm patient, 50 years-old, female, painless lesion involving several lower incisors). Because the lesions were asymptomatic and already exhibited signs of repair, biopsy was not considered. The only procedure executed was periodic radiographic following-up. One year clinical and radiographical following-up examination showed satisfactory signs of lesion evolution.

Discussion
Periapical cemento-osseous dysplasia is an asymptomatic clinical condition occurring exclusively in the mandible's anterior area and whose etiology remains inconclusive. Literature has presented several clinical cases and in some of them due to misdiagnosis a satisfactory result was not achieved 3,5,7,8,10,12,19,20,24,25,26,31.
In this present case report, a 50-year-old melanoderm female patient sought for dental treatment because of a discomfort in the bicuspid area where there were osseointegrated implants. During the patient's examination, a routine panoramic radiograph was executed and revealed the presence of a lesion with mixed radiographic aspect. Periapical cemento-osseous dysplasia at its cementoblastic stage demonstrated a radiolucent-radiopaque mixed pattern with a well defined radiolucent halo surrounding the radiopacity areas 6. The cases of periapical cemento-osseous dysplasia are often detected through routine radiographic examinations 17. Although periapical cemento-osseous dysplasia is a lesion easily diagnosed, it can be mistaken by other alterations occurring at the area closer to tooth apexes, such as: apical periodontal cyst, periapical granuloma and chronic osteomyelitis. This could occur during periapical cemento-osseous dysplasia evolution first stages, and the case could be misled. Differential diagnosis of periapical cemento-osseous dysplasia at its cementoblastic stage includes chronic sclerosing osteomyelitis, ossifying/cementing fibroma, odontoma, and osteoblastoma 7. In this context, the case's clinical and radiographic features are fundamental at the moment of establishing the definitive diagnosis.
The radiographic image may be erroneously interpreted as an infection of endodontic origin. In these cases, tests evaluating pulp tissue vitality are important to elucidate any clinical confusion 8. In this case report, the radiographic image was very suggestive of periapical cemento-osseous dysplasia. However, even then, we opted to perform vitality cold/hot and vertical percussion tests.
The key points for this disease diagnosis, according to Brannon & Fowler 4 are:
• Predilection for mid-age Black women;
• One or more circumscribed lesions (0.5 cm or shorter) at the periapical area of vital teeth;
• Painless non-expansive lesion located usually at mandible's anterior area;
• Radiographic characteristics can be radiolucency of mixed density (radiolucent with opacities), or opaque with a narrow radiolucent margin;
• Cellular fibrous stroma with lamellar osseous tissue and/or oval calcifications.
The case here described fulfills almost all the characteristics of the diagnosis suggested by Brannon & Fowler 4. The lesion occurred in a mid-age Black woman presenting a non-expansive extensive painless intra-osseous lesion localized at the mandible's anterior area. The radiographic aspect observed in the radiographs revealed that the lesion was large, of mixed density, and it seemed a result of the union of several lesions affecting the incisors and canine teeth.
It is a consensus that the execution of invasive procedures, such as tooth extraction and biopsy for histopathological analysis in periapical cemento-osseous dysplasia patients is extremely contraindicated. Such procedures may cause the inoculation of bacteria into the lesions and begin a serious infection. Additionally, because blood vessels are not capable of penetrating into the thick cortical margins surrounding the lesions, the use of antimicrobial therapy is not effective 20. Therefore, since patient did not report any discomfort at the lesion area, radiographic follow-up of the case was conducted. Patient returned 12 months later and the lesion still preserved its radiolucent aspect with increase of internal radiopacity.
Because periapical cemento-osseous dysplasia approach is the clinical and radiographic following-up, biopsies are not executed. This contributes to some extent that further histopathological studies be limited. At macroscopic examination, stained fragments coming from periapical cemento-osseous dysplasia are of brownish color and friable aspect 28. The histomorphological findings of periapical, focal and florid dysplasias are essentially undistinguishable and show a spectrum of progressive features depending on, especially, the stage of the lesions' development. At the initial stages, the lesions are represented by a fibrous non-encapsulated conjunctive tissue exhibiting numerous blood vessels of small caliber and lack of inflammatory cells 4. The case here described, due to its radiographic aspect, probably was at cementoblastic stage, which is characterized by a variable amount of mineralized tissue comprising immature bone trabeculae and round drops of a tissue similar to cementum. These structures of tissue similar to cementum may fuse to each other and produce larger aggregates with rounded contours accounting for increasing the radiopacity degree within the lesions 11.
Periapical cemento-osseous dysplasias are probably the most common fibro-osseous lesions found in clinical practice. Its pathogenesis remains unknown, although it can represent a reactive or dysplastic process. The dentist must be aware of the appearance of these lesions in clinical practice and have enough knowledge to determine the proper diagnosis, avoiding therefore inappropriate approaches which can compromise the patient's health.
The patient searched for treatment due to her discomfort in an edentulous area where implants had been installed about one year ago. Pain or discomfort may be one of the first signs of implant's failure, usually with its mobility 13. Additionally, persistent discomfort could occur prior to any radiographic chance to be detected 32. A fractured or loosen implant should be the first hypothesis when a patient complaint about discomfort or that the implant is loosen. According to the American Academy of Periodontics 1, periodical evaluation after implant installation should follow the following factors: a) presence of plaque or calculus; b) clinical aspect of the periimplantar tissue; c) the implant's and surrounding structure's radiographic aspect; d) occlusal status and the prosthesis and implants' stability; e) probing depth and the presence of exsudate or bleeding to probe; f) the function and the patient's comfort.
This case report's patient underwent a clinical and radiographic examination which identified a possible relation of the reported sensibility to an occlusal imbalance. Once the occlusion adjustment was performed, patient returned without complaints.
Conclusion
Intra-osseous lesion misdiagnosis found in routine examinations is common. Periapical cemento-osseous dysplasia is a condition with particular characteristics and whose diagnosis is based on the case's clinical and radiographic information.
References
1. American Academy of Periodontology. Position paper. Dental implants in periodontal therapy. J Periodontol. 2000;71(12):1934-42. [ Links ]
2. Barnes L, Eveson JW, Reichart P, Sidransky D. Genética e patologia dos tumores de cabeça e pescoço. São Paulo: Santos; 2009.
3. Bittencourt S, Meira AL, Ferreira OS, Tunes U, Ribeiro E, Casati MZ. Displasia cementária periapical – relato de caso. Rev Inst Ciênc Saúde. 2007;25(3):319-21.
4. Brannon RB, Fowler CB. Benign fibro-osseous lesions: a review of current concepts. Adv Anat Pathol. 2001;8(3):126-43.
5. Cecília MS, Favieri A, Aroeira R. Displasia cementária periapical, conseqüência de diagnóstico incorreto: relato de caso. RBO. 2000;57(1):10-1.
6. Eversole R, Su L, ElMofty S. Benign fibro-osseous lesions of the craniofacial complex – a review. Head and Neck Pathol. 2008;2:177-202.
7. Galgano C, Samson J, Kuffer R, Lombardi T. Focal cemento-osseous dysplasia involving a mandibular lateral incisor. Int Endod J. 2003;36(12):907-11.
8. Gariba-Silva R, Sousa-Neto MD, Carvalho Jr JR, Saquy PC, Pecora JD. Periapical cemental dysplasia: case report. Braz Dent J. 1999;10(1):55-7.
9. Kawai T, Hiranuma H, Kishino M, Jikko A, Sakuda M. Cemento-osseous dysplasia of the jaws in 54 Japanese patients: a radiographic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87(1):107-14.
10. Komabayashi T, Zhu Q. Cemento-osseous dysplasia in an elderly Asian male: a case report. J Oral Sci. 2011;53(1):117-20.
11. Langlais RP, Langland OE, Nortjé CJ. Diagnostic imaging of the jaws. Malver: Williams & Wilkins; 1995. p. 540-6.
12. Leal RM, Santiago Mde O, Silveira FF, Nunes E, Capistrano HM. Periapical cemental dysplasia in twin sisters: a case report. Quintessence Int. 2009;40(10):e89-92.
13. Lekholm U, van Steenberghe D, Herrmann I. Osseointegrated implants in the treatment of partially edentulous jaws: a prospective 5-year multicenter study. Int J Oral Maxillofac Implants. 1994;9:627-35.
14. Melrose RJ. The clinicopathologic spectrum of cemento-osseous dysplasia. Oral Maxillofacial Surg Clinical North Amer. 1997;9(4):643-53.
15. Neville BW, Albenesius RJ, Charleston SC. The prevalence of benign fibro-osseous lesions of periodontal ligament origin in black women: a radiographic survey. Oral Surg Oral Med Oral Pathol. 1986;62(3):340-4.
16. Neville BW, Damm DD, Allen CM, Bouquot JE. Patologia oral e maxilofacial. Rio de Janeiro: Guanabara Koogan; 2004. p. 534-8.
17. Ogunsalu CO, Lewis A, Doonquah L. Benign fibro-osseous lesions of the jaw bones in Jamaica: analysis of 32 cases. Oral Diseases. 2001;7:155-62.
18. Pereira RM, Ribeiro EDP, Bittencourt S. Displasia cementária periapical: estudo de prevalência. Innov Implant J Biomater Esthet. 2008;3(5):43-6.
19. Pippi R, Della Rocca C, Sfasciotti GL. Periapical cemental (fibrous) dysplasia. Clinical, radiographic and pathologic aspects in 7 reported cases. Minerva Stomatol. 2004;53(4):135-41.
20. Sethusa MPS, Khan MI. The orthodontic management of a patient presenting with cemento-osseous dysplasia. SADJ. 2009;64(3):120-4.
21. Slootweg PJ. Bone diseases of the jaws. Int J Dent. 2010;2010:1-7.
22. Slootweg PJ. Displasias ósseas. Genética e patologia dos tumores de cabeça e pescoço. São Paulo: Santos; 2009. p. 323.
23. Slootweg PJ. Lesions of the jaws. Histopathology. 2009;54(4):401-18.
24. Smeele LE, Baart JA, Van der Waal I. Unusual behavior of periapical cementous dysplasia. Br J Oral Maxillofac Surg. 1991;29(1):58-60.
25. Smith S, Patel K, Hoskinson AE. Periapical cemental dysplasia: a case of misdiagnosis. Br Dent J. 1998;185:122-3.
26. Studart-Soares EC, Scortegana A, Azoubel E, Pezzi LPG, Sant'ana Filho M. Lesões fibro-ósseas: displasia cemento-óssea periapical X displasia cemento-óssea florida. R Fac Odontol Porto Alegre. 1998;39(2):26-30.
27. Su L, Weathers DR, Waldron CA. Distinguishing features of focal cemento-osseous dysplasia and cemento-ossifying fibromas. II. A clinical and radiologic spectrum of 316 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(5):540-9.
28. Su L, Weathers DR, Waldron CA. Distinguishing features of focal cemento-osseous dysplasias and cemento-ossifying fibromas: I. A pathologic spectrum of 316 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(3):301-9.
29. Summerlin DJ, Tomich CE. Focal cemento-osseous dysplasia: a clinicopathologic study of 221 cases. Oral Surg Oral Med Oral Pathol. 1994;78(5):611-20.
30. Vicci JG, Capelozza ALA. Incidência de lesões dentárias e ósseas evidenciadas através de radiografia panorâmica. FOL/UNIMEP. 2002;14(2):43-6.
31. Wilcox LR, Walton RE. Case of mistaken identity: periapical cemental dysplasia in an endodontically treated tooth. Endod Dent Traumatol. 1989;5(6):298-301.
32. Worthingon P, Bolender CL, Taylor TD. The Swedish system of osseointegrated implants: problems and complications encountered during a 4-year trial period. Int J Oral Maxillofac Implants. 1987;2:77-84.
 Correspondence:
Correspondence:
Antonio Adilson Soares de Lima
Curso de Odontologia – Departamento de Estomatologia da UFPR
Rua Prefeito Lothário Meissner, n.º 632 – Jardim Botânico
CEP 80170-210 – Curitiba – PR – Brasil
E-mail:aas.lima@ufpr.br
Received for publication: April 18, 2011
Accepted for publication: June 20, 2011
