










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.2 Joinville Abr./Jun. 2013
CASE REPORT ARTICLE
Apicoectomy after conventional endodontic treatment failure: case report
Lorena Oliveira PedrocheI; Neisiana BarbieriI; Flávia Sens Fagundes TomazinhoI; Luciene Miranda UlbrichI; Denise Piotto LeonardiI; Stephanie Martins SicuroI
I School of Dentistry, Positivo University – Curitiba – PR – Brazil.
ABSTRACT
Introduction: Paraendodontic surgery is a safe and adequate alternative when teeth are not responding to conventional treatment and endodontic re-treatment. It must only be applied in specific situations. Endodontic treatment failures can be related to: extraradicular infections such as periapical actinomycosis; to foreign body reactions that can be caused by endodontic material extrusion; to endogenous cholesterol crystal accumulation in apical tissues; and unresolved cystic lesion. Paraendodontic surgery comprehends a set of procedures recommended in periapical diseases treatment, when traditional endodontic therapy does not obtain favorable outcomes.
Objective: To report a clinical case where an apicoectomy was indicated due to failure in conventional endodontic treatment.
Case report and Conclusion: Clinical case report of a tooth with unsatisfying conventional endodontic treatment history, due to lack of treatment in fourth root canal and an unsuccessful apicoectomy, since the lesion and the fistula had persisted. It was chosen to retreat tooth #26 and perform a new apicoectomy in the mesiobuccal root. The treatment was successful due to absence of fistula and painful symptoms and due to periapical bone repair.
Keywords: microbiology; Endodontic; periodontal pocket.
Introduction
Traditional endodontic treatment aims to eliminate bacteria from root canal system and establish effective barriers against root recontamination 9. To achieve success, cleaning, shaping and filling of the entire root canal system are considered essential steps in endodontic therapy.
Failure factors in root canal conventional treatment are frequently related to presence of residual bacteria (persistent infection) or reinfection in a previously disinfected canal (secondary infection) 29. Endodontic treatment failures can be related to: extraradicular infections such as periapical actinomycosis 31; to foreign body reactions that can be caused by endodontic material extrusion I; to endogenous cholesterol crystal accumulation in apical tissues 20; and unresolved cystic lesion 21. Thus, success relies on different factors and is verified through clinical and radiographic evaluations during follow up 20-22,29,31.
Teeth treated in conventional ways, which presents persistent periapical lesion, may have retreatment as first therapeutic alternative. Especially, accidents during conventional treatment may have negative effect over success, contributing to infection establishment in inaccessible apical areas, requiring surgical intervention 7,35.
Parendodontic surgery comprehends a set of procedures recommended in periapical diseases treatment, when traditional endodontic therapy does not obtain favorable outcomes. Periapical surgery indications are: root canal obliteration impeding endodontic instrumentation access to apical region; endodontic material apical extrusion impeding radiolucent lesions repair and/or causing clinical symptoms; unsuccessful endodontic treatment and retreatment impossibility due to prothesis; root perforation impeding root canal hermetic sealing. The surgery goal is periapical lesion removal and the apical third sealing, allowing soft and hard tissue regeneration 13,33,43.
Parendodontic surgery is a widely studied procedure. According to the meta-analysis of Tsesis et al. 32, paraendodontic surgery success rate is 91.6%, while failure rate is 4.7%. However, its prognosis is influenced by several factors, such as: different surgical procedures and materials, clinical and radiographic evaluation, demography, systemic conditions, local quality factors, for example, the involved teeth and their anatomy, conventional treatment or previous root canal retreatment and restoration quality 32.
Thus, this study aims to report a clinical case of an apicoectomy indicated due to conventional endodontic treatment failure.
Case report
Patient, R. J. F., female, Caucasian, 53 years-old, attended to the Positivo University Dentistry clinic complaining about pain in tooth #26, which presented a history of endodontic treatment and parendodontic surgery (apicoectomy).
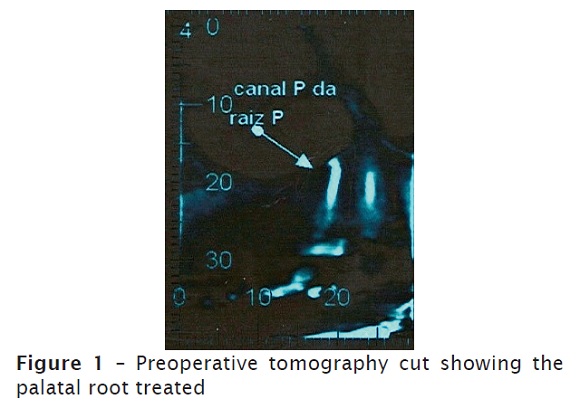
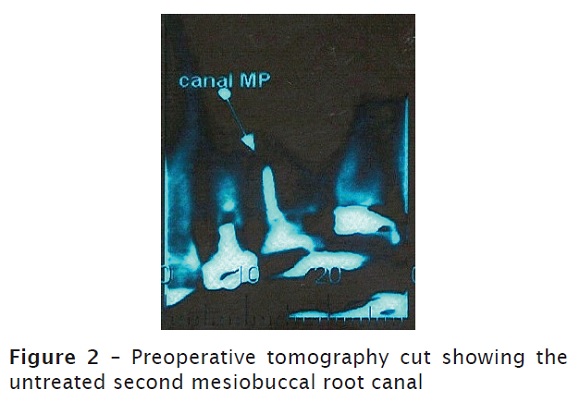
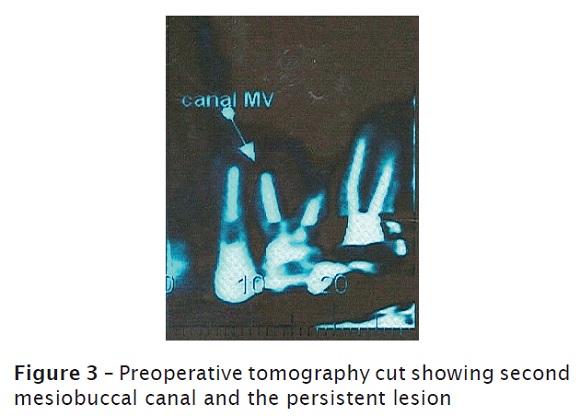
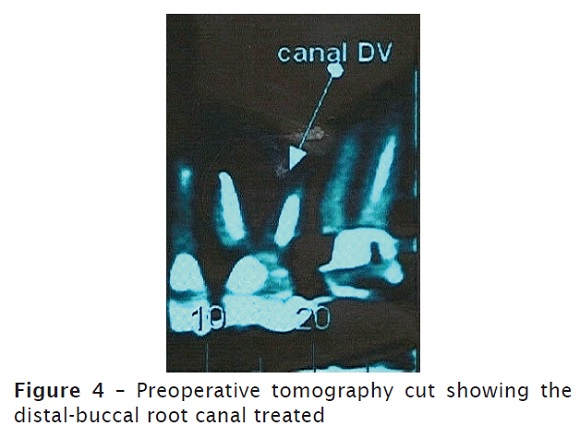
After clinical and radiographic examination, an unsatisfying endodontic treatment was confirmed in the referred tooth. It was observed that the fourth root canal was not treated. There was a radiographic image suggesting a persistent injury in the periapical region of the mesiobuccal root.
The patient was submitted to tomography (figures 1, 2, 3 and 4) and endodontic retreatment was recommended. Ten months after endodontic treatment completed, we observed the reappearance of fistula. Hence, the patient was submitted again to apicoectomy of the mesiobuccal root canal of tooth #26.
To perform the surgical procedure, supraperiosteral and subperiosteral anesthetic techniques were adopted. The topical anesthetic used was benzocaine (DFL, Jacarepaguá, Rio de Janeiro, Brazil) and the local anesthetic was 4% articaine with epinephrine 1:100.000 (DFL, Jacarepaguá, Rio de Janeiro, Brazil) because its anesthetic salt has the biggest anesthesia potential and duration. Three anesthetic tubes was used. Neumann's incision was chosen , starting from the mesial surface of tooth #24 to the distal surface of tooth #27, with the aid of a scalpel blade size #15 (BD, São Paulo, São Paulo, Brazil). The periapical exposure must be satisfactory, to make the injury visible. For this purpose, spherical burs size #6 and #4 were utilized (KOMET, Santo André, São Paulo, Brazil) to access the mesiobuccal root canal. Apical curettage was performed using lucas curette size #85 and #86 (Hu-Friedy, Rio de Janeiro, Rio de Janeiro, Brazil).
Then, 2 mm were cut from root apical area, with the aid of size #702 (KOMET, Santo André, São Paulo, Brazil). Surgical site irrigation was executed with water for injection.
After apical resection, apical surface planing and finishing was performed using multi bladed drills with 5 and 10 blades (KOMET, Santo André, São Paulo, Brazil) and spherical diamond drill size #6 (KOMET, Santo André, São Paulo, Brazil), counterclockwise. The flap was repositioned and fixed with moderated digital pressure and moist gauze. Suturing was made with silk thread 4.0 (Ethicon Johnson, São Paulo, São Paulo, Brazil), performing simple stitches.
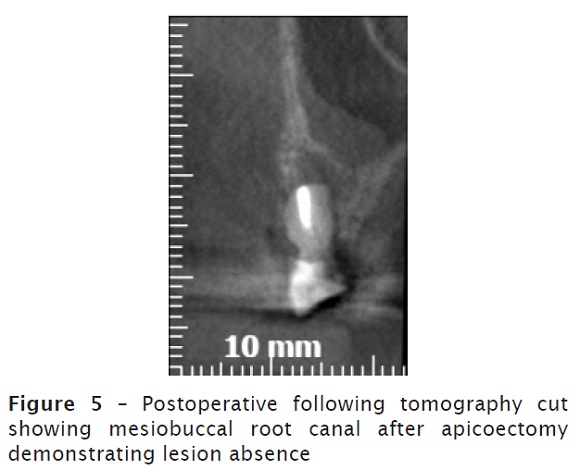
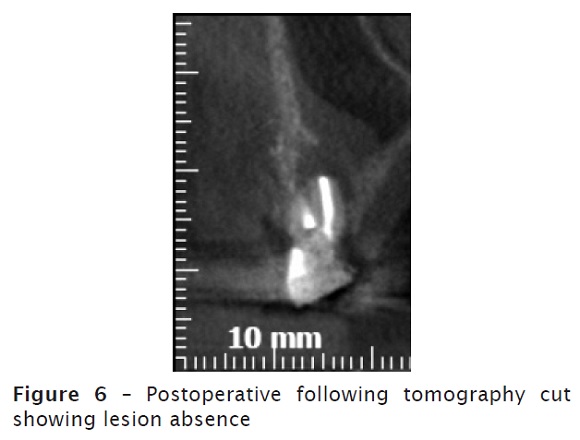
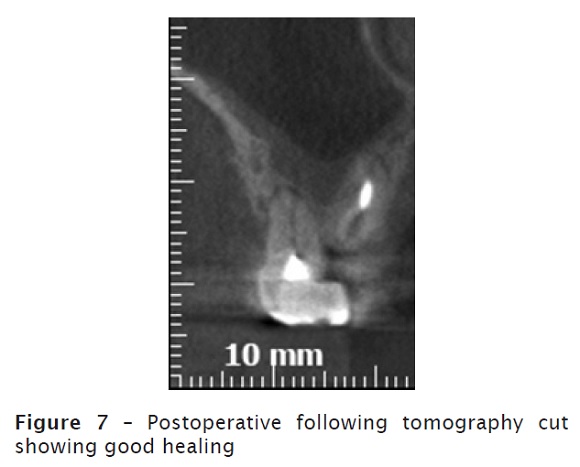
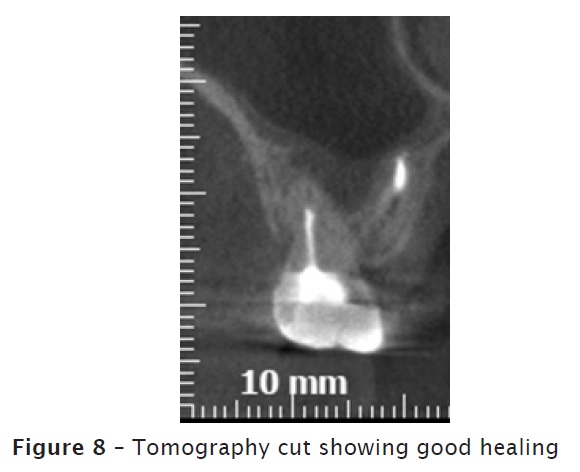
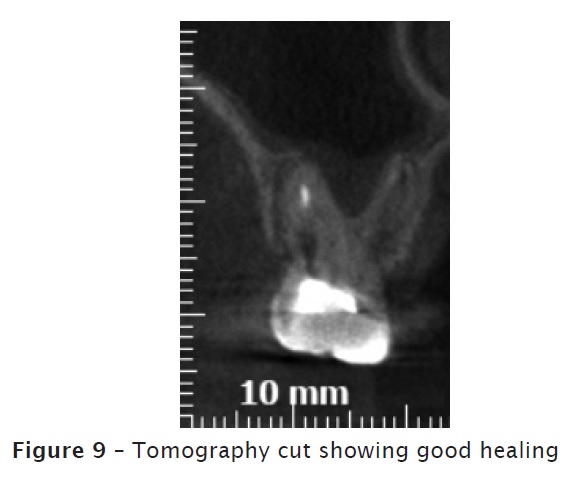
The postoperative medication prescribed to the patient, was Amoxicillin 500mg every 8 hours for 7 days in therapeutic regime, tramadol 50mg every 6 hours for 3 days and dipyrone 500mg for analgesia every 6 hours during 3 days. To oral hygiene, it was prescribed 0.12% chlorhexidine solution twice a day. The patient returned after 7 days for suture removal. After 7 months, a new computed tomography was requested to follow-up the case (figures 5 and 6). In this examination, the successful of the apicoectomy surgery was proven due to healing and lack of fistula (figures 7, 8 and 9).
Discussion
Endodontic surgery is a surgical procedure which consists in the excision of pathological periapical tissue from root surface (including apical accessory canals), and, lastly, canal or canals sealing against pathologic agents, thus reaching the goal of creating the best conditions to the tissue health, regeneration and creation of new tooth structural support.
Among the most adopted surgical methods to solve difficulties, accidents and complications of conventional endodontic treatment, are: curettage with apical planing, apicoectomy, apicoectomy with retrofilling, apicoectomy with retroinstrumentation and canal retrofilling and filling simultaneous to surgery 23.
Apicoectomy consists in the surgical removal of tooth apical portion. It can be indicated in several clinical situations: periapical lesions persistent to conventional treatment, perforations, fractured instruments, apical delta removal and external absorption presence 30,15,16. In this clinical case, the chosen treatment was apicoectomy with curettage and planing, because it was found that the filling was well compacted and then it was chosen not to apply retrograde filling.
Apical portion was cut in 45º related to tooth long axis 6. Despite some authors 10 advocate that the larger the cut angle the larger will be dentinal tubules exposure, this inclination degree was needed to allow total root surface exposure, aiming to facilitate the operative procedures. The chosen drill to cut was size #702 tapered bur, which makes cutting easier through all root extension. The apical cut performed at 3 mm leads to the reduction of the lateral canal in 93%, without the need of largest resections, such as 4 mm. However, we chose to just perform the cut at 2 mm, because the tooth had already suffered an earlier apicoectomy.
Leonardi et al. 11 stated that several factors can influence apicoectomy success, such as: the root region where the apicoectomy is done; the drill type employed or laser execution, as well as the cut angle. It is important to obtain the cut surface as regular as it can. The apical cut must involve anatomical variations such as the presence of isthmuses and accessory canals, because they act as a reservoir for bacteria and necrotic pulp tissue, which can lead to treatment failure. After apicoectomy, it must be observed whether the filling material is not displaced, using a microscope, because failures may be invisible with unaided eyes.
To pathological tissue removal, lucas curettes size #85 and #86 were employed. Periapical curettage aims to remove pathological tissue in a lesion at the apical level of a tooth or foreign bodiesat periapical region.This must be followed by apical planing. This is necessary, because the cement covering the root apical portion is reabsorved due to periapical lesion 28.
Lastly, it is very important to perform the apical cut surface finishing, which can be made with manual or mechanical instruments, such as steel files and drills, to promote neoformed cement deposition over the sectioned apical dentine 1. In this clinical case, multibladed drills with 5 and 10 blades and spherical bur size #6 were employed, counterclockwise. This aims to the planing and sealing of dentinal tubules that were exposed to promote repair.
To complement diagnosis and guide the treatment, pre and postoperative tomography were applied. Computed tomography has better detection performance in periapical lesions 4,12,18,24, root canal system evaluation 13,17, reabsorption evaluation, and endodontic surgery planning when compared with conventional radiography. It has the advantage of overcoming conventional radiography limitations, such as anatomical image overlaying and geometric distortion 2,26.
Seven months after, it was perceived the absence of fistula, painful symptoms and periapical bone repair, data that confirms a successful procedure. By the means of computed tomography, the radiolucent image, it is interpreted as fibril healing.
Conclusion
The surgical technique applied in this case, apicoectomy, was appropriate. This was proven by both clinical results and computed tomography.
References
1. Bramante CM, Torres M, Morais IG, Bernardineli N, Garcia RB. Avaliação da superfície apical após apicectomia e alisamento com instrumentos manuais e mecanizados. J Bras Endod. 2003. [ Links ]
2. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic application of cone-beam volumetric tomography. J Endod. 2007;33:1121-32. [ Links ]
3. Eskandarinezhad M, Ghasemi N. Nonsurgical endodontic retreatment of maxillary second molar with two palatal root canals: a case report. J Dent Res Dent Clin Dent Prospect. 2012;6(2):75-8. [ Links ]
4. Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008;34:273-9. [ Links ]
5. Friedman S. Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure). Endod Topics. 2002;1:54-78. [ Links ]
6. Gilhe PA, Figdor D, Tyas MJ. Apical dentin permeability end microleakage associated if root end ressection end retrograde filling. J Endod. 1994;20:22-6. [ Links ]
7. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004;30:1-4. [ Links ]
8. Gutmann JL, Harrison JW. Surgical endodontics. Blackwell Scientific Publications. 1991:362-8. [ Links ]
9. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006(32):601-23. [ Links ]
10. Kim S, Pécora G, Rubinsten R, Dorscher-Kim J. Microsurgery in endodontics. W.B. Saunders Company; 2001. 172 p. [ Links ]
11. Leonardi DP, Fagundes FS, Haragushiku GA, Tomazinho PH, Baratto-Filho F. Cirurgia parendodôntica: avaliação de diferentes técnicas para a realização da apicectomia. RSBO. 2006. [ Links ]
12. Lofthag-Hansen S, Huumonen S, Grondahl K, Grondahl HG. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:114-9. [ Links ]
13. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34:87-9. [ Links ]
14. Martos RR, Lagares DT, Cosano LC, Figallo MRS, Egea JJS, Perez JLG. Evaluation of apical preparations performed with ultrasonicdiamond and stainless steel tips at different intensities usinga scanning electron microscope in endodontic surgery. Med Oral Patol Oral Cir Bucal. 2012. [ Links ]
15. Matsura SJ. A simplified root-end filling technique using silver amalgam. J Mich St Dent Assoc. 1962;44:40-1. [ Links ]
16. Messing JJ. The use of alamgam in endodontics surgery. J Br Endod Soc. 1967;1:34-6. [ Links ]
17. Michetti J, Maret D, Mallet JP, Diemer F. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J Endod. 2010;36:1187-90. [ Links ]
18. Nakata K, Naitoh M, Izumi M, Inamoto K, Ariji E, Nakamura H. Effectiveness of dental computed tomography in diagnostic imaging of periradicular lesion of each root of a multirooted tooth: a case report. J Endod. 2006;32:583-7. [ Links ]
19. Nakata K, Naitoh M, Izumi M, Ariji E, Nakamura H. Evaluation of correspondence of dental computed tomography imaging to anatomic observation of external root resorption. J Endod. 2009;35:1594-7. [ Links ]
20. Nair PN. Cholesterol as an aetiological agent in endodontic failures: a review. Aust Endod J. 1999;25:19-26. [ Links ]
21. Nair PN, Pajarola G, Schroeder HE. Types and incidence of human periapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81:93-102. [ Links ]
22. Nair PN, Sjögren U, Krey G, Sundqvist G. Therapy-resistant foreign body giant cell granuloma at the periapex of a root-filled human tooth. J Endod. 1990;16:589-95. [ Links ]
23. Orso VA, Sant'ana FM. Cirurgia parendodôntica: quando e como fazer. Rev Fac Odontol Porto Alegre. 2006. [ Links ]
24. Patel S, Dawood A, Mannocci F, Wilson R, Pitt Ford T. Detection of periapical bone defects in human jaws using cone beam computed tomography and intraoral radiography. Int Endod J. 2009;42:507-15. [ Links ]
25. Patel S, Dawood A, Wilson R, Horner K, Mannocci F. The detection and management of root resorption lesions using cone beam computed tomography: an in vivo investigation. Int Endod J. 2009;42:831-8. [ Links ]
26. Patel S. New dimensions in endodontic imaging: part 2 – cone beam computed tomography. Int Endod J. 2009;42:463-75.
27. Rigolone M, Pasqualini D, Bianchi L, Berutti E, Bianchi SD. Vestibular surgical access to the palatine root of the superior first molar: ‘‘low-dose cone-beam'' CT analysis of the pathway and its anatomic variations. J Endod. 2003;29:773-5.
28. Rosa Neto JJ. Estudo em microscopia eletrônica de varredura do ápice radicular e do limite de obturação em dentes portadores de lesão periapical crônica [dissertação]. Faculdade de Odontologia de Araraquara; 1997. [ Links ]
29. Siqueira Jr JF. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics. 2005;10:123-47. [ Links ]
30. Tanzilli JP, Raphael D, Moodnik RM. A comparison of the marginal adaptation of retrograde techniques: a scanning electron microscopic study. O Surg O Med O Pathol. 1980;50:74-80. [ Links ]
31. Tronstad L, Barnett F, Cervone F. Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod Dent Traumatol. 1990;6:73-7. [ Links ]
32. Tsesis I, Faivishevsky V, Kfir A, Rosen E. Outcome of surgical endodontic treatment performed by a modern technique: a meta-analysis of literature. J Endod. 2009;35:1505-11. [ Links ]
33. Von Arx T, Gerber C, Hardt N. Periradicular surgery of molars: a prospective clinical study with a one-year follow-up. Int Endod J. 2001;34:520-5. [ Links ]
34. Zerbinati LPS, Tonietto L, Moraes JFD, Oliveira MG. Assessment of marginal adaptation after apicoectomy and apical sealing with Nd:YAG laser. Photomedicine and Laser Surgery. 2012;30(8):444-50. [ Links ]
35. Wu MK, Dummer PM, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. Int Endod J. 2006;39:343-56. [ Links ]
 Corresponding author:
Corresponding author:
Lorena Oliveira Pedroche
Rua Alferes Ângelo Sampaio, n. 1.166
CEP 80420-160 – Curitiba – PR – Curitiba
E-mail: lo.pedroche@gmail.com
Received for publication: December 4, 2012
Accepted for publication: December 19, 2012
