










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.1 Joinville Jan./Mar. 2014
ORIGINAL RESEARCH ARTICLE
Endodontists perceptions of single and multiple visit root canal treatment: a survey in Florianópolis – Brazil
Monica de Souza NettoI; Flavia SaavedraII; Jacy Simi JúniorI; Ricardo MachadoI; Emmanuel João Nogueira Leal SilvaIII; Luiz Pascoal VansanIV
I Integrated College from North of Minas Gerais – Florianópolis – SC – Brazil
II State University of Rio de Janeiro – Rio de Janeiro – RJ – Brazil
III Grande Rio University – Duque de Caxias – RJ – Brazil
IV Ribeirão Preto Dental School, University of São Paulo – Ribeirão Preto – SP – Brazil
ABSTRACT
Introduction: One of the main debates that have occurred in Endodontics is about the amount of sessions required to complete an appropriate treatment. There are very different philosophies regarding this matter. Objective: to the aim of this study was to investigate the Endodontists' point of view regarding single and multiple visit root canal treatment, identifying the basis on which the choice is made and how the information necessary for the choice is acquired. Material and methods: Endodontists registered in the dental practice board of Florianópolis/SC were contacted, and if they agreed to participate, they were interviewed using a questionnaire. The following topics were addressed: demographics, current clinical procedures, treatment rationales and preferences. Forty-three endodontists agreed to participate in the study. Results: Single visit endodontic treatment is carried out in 59.5% of biopulpectomy cases, 31.0% of necropulpectomy cases without lesion and only 11.9% in necropulpectomy cases with periapical lesion. The presence of vital pulp (81.4%) and a canal without exudate (93.0%) are the most important criteria for carrying out single visit endodontic treatment. The most used intracanal medication was calcium hydroxide. The lack of studies comparing long-term success on single visit endodontic treatment is considered an important issue to determine this therapy. Conclusion: It can be concluded that Florianopolis-Brazil endodontists prefer multiple visit over single visit root canal treatment in pulp necrosis cases. When pulp vitality is not compromised there is an increase in the number of endodontists who choose single visit root canal treatment.
Keywords: Endodontics; single visit; multiple visit.
Introduction
Single and multiple visit root canal treatment has been the subject of long-standing debate in the endodontic community, not only on the biological and efficiency point of view, but also on the operator and patient's comfort, satisfaction and preferences 29. Both options of treatment, single and multiple visits, are based on solid studies, but the number of different opinions is still significant 12,14,16,18,24,26,30,33,39.
Single visit endodontic therapy has many advantage, e.g. (a) it reduces the number of patient appointments; (b) it eliminates the chance for interappointment microbial contamination; (c) it allows for the immediate use of the canal space retention of a post; and (d) it allows the endodontists perform the root canal filling when they are more familiar with the canal anatomy 4,22,32,40. However, two concerns regarding single visit root canal treatment still make many endodontists do not use this therapy: (a) the incidence of flare-ups and (b) the long-term success 9,36. Recent studies demonstrated no differences between single and multiple visit treatment regarding to postoperative complications 1,5,31; however, there is a lack of conclusive studies demonstrating the long-term success of single visit treatment in necrotic pulp teeth 14,26,39.
The aim of the present study was to investigate endodontists' point of view regarding single and multiple visit root canal treatment, identifying the basis on which the choice is made and how the information necessary for the choice is acquired.
Material and methods
A questionnaire was sent to 103 endodontists, resident in Florianópolis/SC, Brazil and listed in the Brazilian Federal Board of Dentists. It was e mailed with wording briefly explaining the purpose of the study. The questionnaires were divided in two sections: (i) The first one was about age, gender, place of work, time since graduation and level of academic degree; (ii) The second one consisted in questions about current clinical procedures, treatment options, preferences and opinion about single and multiple visit canal treatment. The answers were recorded and entered into spread sheet software for analysis. Descriptive statistics were used.
Results
Profile of the Endodontists and clinical preferences and procedures
Forty-three endodontists agreed to participate in the study. 53.5% were male and 46.5% were female. Of these, 88.4% had neither a master nor doctorate degree. Most of them have more than ten years of specialist practice (60.5%). Almost 80% of all participants used hand files for canal preparation, mostly in a crown-down technique. The sodium hypochlorite is the preferential irrigation substance for 86% endodontists.
Opinion about single and multiple visit canal treatment
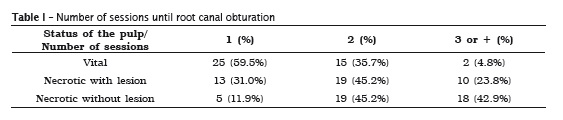
Concerning to the time to complete a single visit treatment, most part of the professionals reported taking more than 90 minutes to complete the treatment of a molar both for vital and necrotic pulp (44% and 60%, respectively). Single visit therapy is usually practiced by almost 60.0% of all endodontists interviewed in cases of vital pulp, but when the biological status of the pulp becomes necrotic very few still choose this treatment type (table I). However, most of participants were willing to provide single visit treatment in cases of necrot ic pulp without periapical lesion (53.4%) rather than in cases with periapical lesion (79.0%).
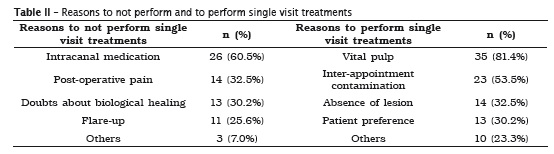
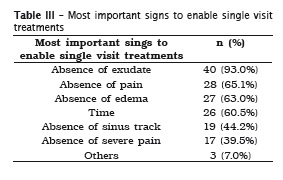
When questioned about what were the most commonly volunteered reasons for not performing a single visit therapy in teeth with pulp necrosis with or without periapical lesion, 60.5% of the participants answered the "importance of the intracanal medication". On the other hand, when asked about the main reason to perform a single visit treatment, 81.4% of the professionals answered that vital pulp is the most important aspect (table II). The most important reason to allow this treatment type was the absence of exudate for 93.0% of them. Other reasons are shown in table III.
Discussion
The aim of the present study was to investigate the endodontists' point of view regarding to single and multiple visit root canal treatment. When the answers of the questionnaire were analyzed, we realized that the single visit therapy is wellaccepted in cases of vital pulp. The concern about the chance of inter-appointment contamination, especially in vital pulp teeth, was also named as one of the important causes to perform a single visit treatment. These results are in agreement with the endodontic literature. Several studies have recognized the great importance of coronal seal for the long-term success of endodontic therapy 19,20,32,35. With regard to the endodontic treatment in teeth with necrotic pulp, the most of specialists still prefer to perform multiple visit therapy. Only a small amount of then prioritize a single visit therapy in this cases. These results are similar to previous studies, such as Araujo Filho et al. 3 who also found that single visits are widely accepted by the Endodontists from Rio de Janeiro, mainly in teeth with vital pulp. In contrast, the percentage of participants that performed single visit treatments decreases broadly in cases of necrosis with and without periapical lesion, which can probably be justified by another data from this research that shows the value of intracanal medication on the biological healing for these Brazilian endodontists, even though the current best available evidence does not support such notion 28.
Although single visit treatment was not performed by most of the endodont ists, the treatment of necrotic teeth with periapical lesion has been done successfully by many authors who justify the results by the elimination of bacterial contamination in the root canal through adequate instrumentation, irrigation and filling 2,7,41. Despite the large refusal, the treatment of teeth with pulp necrosis, with or without periapical lesion, has been successfully established and approved by many authors. Field et al. 11 retrospectively assessed the success rate of single visit root canal therapy. Both vital and necrotic cases, as well as those with and without periradicular disease were included. They found that 199 teeth had clinical and radiographic success over 223 available cases.
The major listed problem to not perform root canal treatment in single visit is the importance of using an intracanal medication to promote a better disinfection process. The most reported intracanal medication was calcium hydroxide for the time of seven days. Several studies highlighted the benefits of the use of calcium hydroxide during endodontic therapy 33,34. Trope 36 demonstrated that the use of intracanal medication with calcium hydroxide can improve healing when compared to single visit therapy. Despite of the well-known disinfection properties of this medication, several studies demonstrate its inability to completely eliminate microorganisms from the root canal system 18,25,26. Vivacqua-Gomes et al. 37 demonstrated that calcium hydroxide was unable to eliminate Enterococcus faecalis completely from dentinal tubules after seven or fourteen days.
In this present study, dry root canal without exudates, was pointed out as one of the important factors during the decision-making to perform a single visit appointment. These results are in agreement with previous studies 38,41 which confirm that the moisture condition of root canal is an important issue in the decision to perform this approach. Moisture and liquids can negatively affect the sealing ability. It may inhibit, prolong or accelerate the setting process of root canal sealers, which may result in higher leakage 27.
In this present study, most interviewed endodontists reported the use of hand files and the Crown-Down technique. It has been shown that this technique can reduce the chance of accumulation of smear-layer in the apical area, improving the prognosis of immediate obturation 10. Also, some studies demonstrated that shaping the canal by using Crown-Down philosophy provides a cleaner apical third of the root canals 6. The use of hand files instead of mechanical Ni-Ti files could be explained by the late popularization of these instruments and the discontinuous in the education of the endodontists in Brazil. 60.5% of all specialists have more than 10 years of experience, and at the time they were studying, Ni-Ti mechanical files were not so popular. Also, almost 90% of them have neither master's degree nor doctorate choosing to keep on a private practice career, which among Brazilian's endodontists almost always results in lack of updating on clinical and scientific knowledge.
Concerning to the irrigation solution, sodium hypochlorite and the EDTA were the most used ones. These results are in agreement with the literature, which confirms the bactericidal, organic tissue dissolution potential and low surface tension of the former 17,23, associate to the ability to remove smear-layer of EDTA 15.
Although there is a paradigm about single visit on the Brazilian endodontic community, it is important to highlight that regarding single versus multiple visit therapy, there is very few or no difference between its quality, post operative complication incidence, success and failure clinical indexes, which reinforce the practical of single session therapy 8,13,21.
Conclusion
Within the results of this study, it can be concluded that most of Florianopolis' Endodontists perform single-visit root canal treatment in cases of vital pulp endodontic therapy, but in cases of necrotic pulp, most of the participants perform multiple-visit endodontic treatment. The main and most important reason to perform a single-visit endodontic treatment is pulp vitality.
References
1. Albashaireh ZS, Alnegrish AS. Post-obturation pain after single and multiple visit endodontic therapy. A prospective study. J Dent. 1998;26:222-32. [ Links ]
2. Araújo Filho WR, Sendra MC. Tratamento endodôntico em sessão única. Avaliação clínicoradiográfica. Rev Cient OCEx. 1998;2:6-8.
3. Araújo Filho WR, Cabreira MS, Costa FF. Tratamento endodôntico em sessão única: levantamento da opinião de endodontistas da cidade do Rio de Janeiro. Rev Bras Odontol. 2003;60:103-5.
4. Ashkenaz, PJ. One-visit endodontics. Dent Clin North Am. 1984;28:853-63.
5. Bhagwat S, Mehta D. Incidence of post-operative pain following single visit endodontics in vital and non-vital teeth: An in vivo study. Contemp Clin Dent. 2013;4:295-302.
6. Bhuyan A, Boruah L, Katak R. Histological evaluation of the effectiveness of four instrumentation techniques for cleaning apical third of root canals – an in vitro study. J Conserv Dent. 2006;9:134-9.
7. Buchanan SL. The art of endodontics: selected case histories, part 2. Dent Today. 1997;16:50-1.
8. Davini F, Cunha RS, Fontana CE, Silveira CFM, Bueno CES. Radix entomolaris – a case report. RSBO. 2012;9:340-4.
9. Eleazer PD, Eleazer KR. Flare-up rate in pulpally necrotic molars in one-visit versus two-visit endodontic treatment. J Endod. 1998;24:614-6.
10. Fava LRG. A comparison of one versus tab appointment endodontic therapy in teeth with nonvital pulps. Int Endod J. 1989;22:179-83.
11. Field JM, Gutmann JL, Solomon ES, Rakusin H. A clinical radiographic retrospective assessment of the success rate of single-visit root canal treatment. Int Endod J. 2004;37:70-82.
12. Figini L, Lodi G, Gorni F, Gagliani M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2007;34:1041-7.
13. Fontana CE, Ibanéz CDM, Davini F, De Martin AS, Silveira CFM, Rocha DGP et al. Endodontic therapy of maxillary second molar showing an unusual internal anatomy. RSBO. 2012;9:213-7.
14. Friedman S. Success and failure of initial endodontic therapy. Ont Dent. 1997;74:35-8.
15. Hulsmann M, Heckendorff M, Lennon A. Chelating agents in root canal treatment: mode of action and indications for their use. Int Endod J. 2003;36:810-30.
16. Inamoto K, Kojima K, Nagamatsu K, Hamaguch A, Nakata K, Nakamura H. A survey of the incidence of single-visit endodontics. J Endod. 2002;28:371-4.
17. Leonardo MR, Leal JM. Endodont ia: tratamento de canais radiculares. 3. ed. São Paulo: Panamericana; 1998. 901 p.
18. Machado MEL. Endodontia: da biologia à técnica. 1. ed. São Paulo: Santos; 2007. 484 p.
19. Madison S, Swanson KL, Chiles SA. An evaluation of coronal microleakage in endodontically treated teeth. Part II. Sealer types. J Endod. 1987;13:109-12.
20. Madison S, Wilcox LR. An evaluation of coronal microleakage in endodontically treated teeth. Part Ill. In vivo study. J Endod. 1988;14:455-8.
21. Miranda TC. O tratamento endodôntico em sessão única depende do estado pulpar e/ou perirradicular? APCD. 1998 Jan-Feb.
22. Morse DR. One-visit endodontics. Hawaii Dent J. 1987;18:12-4.
23. Murad C, Sassone L, Souza M, Fidel R, Fidel S, Hirata R. Antimicrobial activity of sodium hypoclorite, chlorexidine and MTAD against enterococcus faecalis biofilm on human dentin matrix in vitro. RSBO. 2012;9:143-50.
24. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature – part 2. Influence of clinical factors. Int Endod J. 2008;41:6-31.
25. Peters LB, Van Winkelhoff AJ, Buijs JF, Wesselink PR. Effects of instrumentation, irrigation and dressing with calcium hydroxide on infection in pulpless teeth with periapical bone lesions. Int Endod J. 2002;35:13-21.
26. Peters LB, Wesselink PR. Periapical healing of endodontically treated teeth in one and two visists obturated in the presence or absence of detectable microorganisms. Int Endod J. 2002;35:660-7.
27. Roggendorf MJ, Ebert J, Petschel t A, Frankenberger R. Influence of moisture on the apical seal of root canal fillings with five different types of sealer. Int Endod J. 2007;33:31-3.
28. Sathorn C, Parashos P, Messer H. Antibacterial efficacy of calcium hydroxide intracanal dressing: a systematic review and meta-analysis. Int Endod J. 2007;40:2-10.
29. Sathorn C, Parashos P, Messer H. Australian endodontists' perceptions of single and multiple visi t root canal t reatment . Int Endod J. 2009;42:811-8.
30. Sathorn C, Parashos P, Messer H. Effectiveness of single versus multiple visit endodontic treatment of teeth with apical periodontitis: a systematic review and metaanalysis. Int Endod J. 2005;38:347-55.
31. Singh S, Garg A. Incidence of post-operative pain after single visit and multiple visit root canal treatment: a randomized controlled trial. J Conserv Dent. 2012;15:323-7.
32. Siqueira Jr. JF, Rôças IN, Lopes HP, Uzeda M. Coronal leakage of two root canal sealers containing calcium hidroxide after exposure in human saliva. J Endod. 1999;25:14-6.
33. Sjogren U, Figdor D, Peerson S, Sundqvist G. Influence of infection at the time of root filing on the outcome of endodontic treatment of teeth apical periodontitis. Int Endod J. 1997;30:297-306.
34. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long term results of endodontic treatment. J Endod. 1990;16:498-504.
35. Swanson KS, Madison S. An evaluation of coronal microleakage in endodontically treated teeth. Part I. Time periods. J Endod. 1987;13:56-9.
36. Trope M. Flare-up rate of single-visits endodontics. Int Endod J. 1991;24:24-7.
37. Vivacqua-Gomes N, Gurgel-Filho ED, Gomes BPFA, Ferraz CCR, Zaia AA, Souza-Filho FJ. Recovery of Enterococcus faecalis after single or multiple visit root canal treatments carried out in infected teeth ex vivo. Int Endod J. 2005;38:697-704.
38. Walton R, Fouad A. Endodontic interappointment flare-ups: a prospective study of incidence and related factors. J Endod. 1992;18:172-7.
39. Weiger R, Rosendahl R, Lost C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int Endod J. 2000;33:219-26.
40. Whal MJ. Myths of single visit endodontics. Gen Dent. 1996;44:126-31.
41. Wolch I. One appointment endodontic treatment. Dent J. 1975;41:613-5.
 Corresponding author:
Corresponding author:
Ricardo Machado
Faculdades Unidas do Norte de Minas (Funorte/Sobrás)
Rua Trajano, n. 265 – Centro
CEP 88010-010 – Florianópolis – SC - Brasil
E-mail: ricardo.machado.endo@gmail.com
Received for publication: October 12, 2013
Accepted for publication: November 18, 2013
