










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.2 Joinville Abr./Jun. 2014
ORIGINAL RESEARCH ARTICLE
A 7-year retrospective study of biopsied oral lesions in 460 Iranian patients
Shila Ghasemi Moridani I; Fatemeh Shaahsavari I; Mohammad Bagher Adeli II
I Oral Pathology Department, Islamic Azad University, Dental Branch – Tehran – Iran
II Private practice – Tehran – Iran
ABSTRACT
Introduction: Frequency of oral lesions is varied in different population and knowledge of diseases prevalence in a geographic location will improve preventive measures. Objective: The objective of this study was to determine the prevalence of oral biopsied lesions in a major oral pathology laboratory center of city of Tehran. Material and methods: A retrospective study was done on data obtained from the archive of oral and maxillofacial pathology department of Islamic Azad University, dental branch of Tehran, from 2005 to 2011. Following variables were analyzed: age, gender, anatomic location, and the histological results obtained. Lesions were classified to 18 different categories. Data were analyzed using the SPSS version 12.0 for windows Xp. All the data were recorded in Microsoft Office Excel for further evaluation and making a data bank to easy access. Results: Of the 460 patients studied, the mean age was 38 years. The most frequent lesions were in the group of reactive lesions (22.51%), followed by odontogenic cysts. The most frequent lesion was radicular cyst and odontogenic keratocyst (keratocystic odontogenic tumor). Malignant lesions constituted 2.38%, of which squamous cell carcinoma was the most common malignancy (1.52%). Mandible was the most common location for occurrence of lesions (32.6%) followed by gingiva (11.95%). Conclusion: Our study provides helpful information of oral lesion's distribution in an Iranian population. The results showed high frequency of odontogenic keratocyst (keratocystic odontogenic tumor) which is not in agreement with other studies and need more evaluation of etiological factors.
Keywords: oral lesion; retrospective study.
Introduction
When comparing the frequency of oral lesions in different population, major and minor differences regarding to age, gender and geographic distributions would be found. Better control of diseases and improvement of preventive measures will be achieved considering the relative frequency of oral lesions in a geographic location. Many studies focusing on the prevalence of oral and maxillofacial lesions have been conducted around the world 1,2,4,5,11,16,24-27. But to our knowledge, few studies on Iranian population were reported 2,8,9,19,21,22. Surprisingly, we found few reports on the frequency of histologically confirmed oral lesions in Iran 19,21-23. The purpose of this study was to investigate the relative prevalence of different types of oral and maxillofacial biopsied lesions received by the Oral and Maxillofacial Pathology Department of Islamic Azad University and to review the literature on this subject.
Material and methods
This retrospective descriptive study was carried out on the biopsied specimen of the archives of the Oral and Maxillofacial Pathology Department of Islamic Azad University, which is one of the major oral pathology departments of Tehran. The department mainly receives specimen from general and specialized dental practitioners in the North-East of Tehran and affiliated hospital (BouAli hospital) which is located in the East of Tehran. All the specimens from 2005 to 2011 were surveyed and following data were retrieved: patient's age, sex, clinical manifestations and diagnosis and the histopathological results. Lesions were classified in 18 different categories, as detailed in table I.
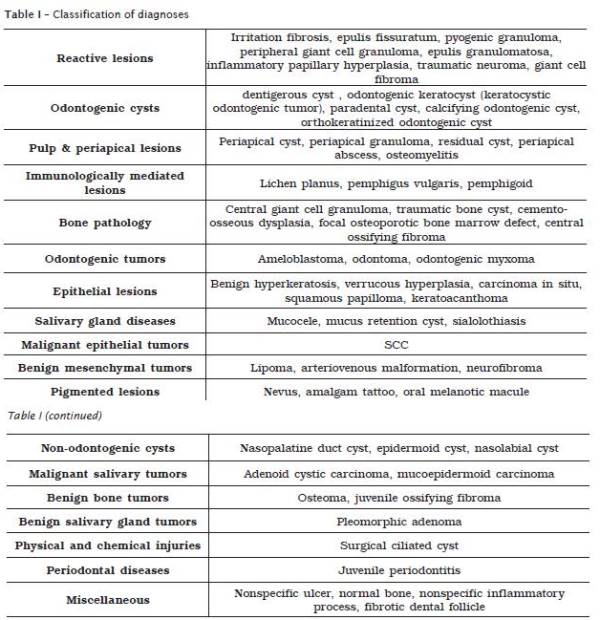
Based on the new WHO classification, odntogenic keratocyst is now considered as an odontogenic tumor, "keratocystic odontogenic tumor" 18. Because most of the previous studies are according to earlier classification system which included the odontogenic keratocyst in odontogenic cyst's group, to comparing the data and better evaluation, we have used the previous classification system 14.
All the results were subjected to statistical analysis, using the SPSS version 12.0 for windows Xp. The data also were recorded in Microsoft Office Excel, as a data bank.
Results
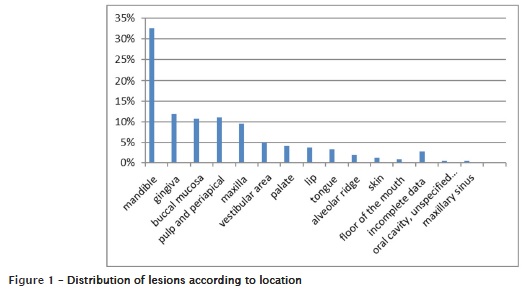
The number of patients studied was 460, excluding patients with incomplete records or those who had more than one biopsy at the same time. The age range of the patients was 3-89 years and the mean age was 38 years. Most of the lesions (62%) were found in the third to fifth decades of life. Females constituted 53.26% (n = 245) of the cases and 46.73% (n = 215) of the lesions found in males. The most affected anatomic location was the mandible (32.6%), followed by gingiva (11.95%) and buccal mucosa (10.86%). The distribution of lesions according to location is shown in figure 1. The prevalence of the most common different diagnoses is shown in table II.
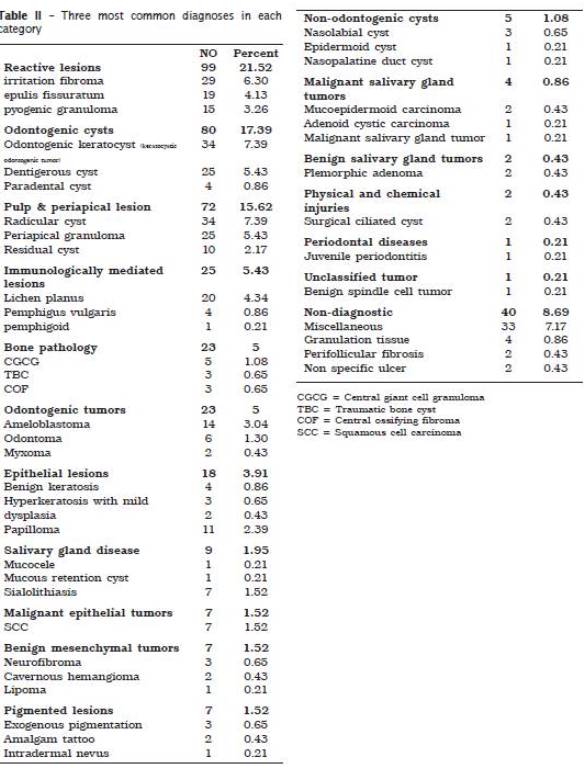
Intra-osseous lesions constituted 56.4% and extra-osseous lesions 43.6%. The most frequent lesions were in the group of reactive lesions (21.52%), followed by odontogenic cysts (17.39%). The most frequent lesion was radicular cyst and odontogenic keratocyst (7.39% each). Malignant lesions constituted 2.38%, of which squamous cell carcinoma was the most common malignancy (1.52%).
Discussion
In this study, we analyzed the prevalence of oral lesions, biopsied during seven years in an academic oral pathology laboratory and found 460 specimens. The mean age of the patients was 38 years and 62% of the lesions were discovered during the third to fifth decades of life. The mean age in similar studies, reported by Fierro-Garibay et al. 4 and Sixto-Requeijo et al. 25 were 54 and 51.8 years respectively. In addition, the mean age in the survey of Kniest et al. 11 was 47.2 years. It seems that oral lesions in our study revealed in lower age range in comparison with other surveys which may be related to younger population in our country. Although, Al-Khateeb 1 reported the mean age of 33 years for the patients, but their study was conducted only on benign oral masses excluding intra-osseous lesions. Luqman and Al Shabab 15 recorded 31 years for mean age in their study which is much similar to our results. Shahsavari et al. 23 analyzed oral mucosal lesions in an Iranian population and found that 90% of lesions were in 30-58 years old. Likely to most of the other studies 4,6,11,25, we found slightly more frequency of lesions in women, which may reflect attitude of women about their oral health. However, in a similar study conducted on a small population of Saudi patients, the majority of lesions were discovered in males 15. In addition, Jahanbani et al. 9 in a clinical based study on an Iranian population, revealed more frequency of lesions among men that may be a sign of different type of study design.
Concerning the anatomical location, about one third (32.6%) of lesions in our study were located in the mandible with statistical significant difference with other locations (p < 0.001). It was followed by gingiva (11.95%) pulp and periapical tissue (11.08%) and buccal mucosa (10.86%). In the study of Fierro-Garibay et al. 4, and Ibnerasa 7, mandible was also the most frequent location. On the other hand, Pour et al. 19 reported the gingiva as the most common location.
Similar to report of Fierro-Garibay et al. 4, intraosseous lesions were more frequent than peripheral lesions in the present study (56.4% Vs 43.6%). It may be interpreted by high frequency of cysts and odontogenic lesions in the present study. In addition, it shows that patients with more advanced and aggressive treatment plans are more referred to our academic oral pathology laboratory. However, in the other report of the Iranian population, peripheral lesions were more common than intraosseous lesions 6.
The most frequent category in this study was reactive lesions (21.52%), followed by odontogenic cysts (17.39%), similar to results of Jones and Franklin 10. However, we accounted the radicular cysts and residual cysts in the pulp and periapical lesion's category. Considering them in the odontogenic lesion's category will show odontogenic cysts as the most prevalent lesions and the results would be different.
Consistent with new WHO classification, odontogenic keratocyst is now considered as an odontogenic tumor named "keratocystic odontogenic tumor" 18. Considering the fact that most of the previous reports and data are according to former classification of WHO, we have used the earlier classification system for better comparison and assessment 14.
The most prevalent odontogenic cyst was radicular cyst and odontogenic keratocyst (keratocystic odontogenic tumor) (7.39% each one), followed by dentigerous cyst (5.43%). These results were different from the same studies which showed radicular cyst as the most prevalent odontogenic cyst. Daley et al. 3, Nakamura et al. 17 and Fierro-Garibay et al. 4, reported the radicular cyst as the most common cyst, followed by dentigerous cyst and odontogenic keratocyst (keratocystic odontogenic tumor). However, in the study of Ramachandra et al. 20 odontogenic keratocyst was the second most common odntogenic cyst after radicular cyst which was in agreement with the report of Koseoglu et al. 12. The high frequency of odontogenic keratocyst in the present study may be due to more recurrence of the cyst which leads to referral of the patients to academic centers. Notwithstanding, the etiological factors should be evaluated in other researches.
Considering the irritation fibroma as the most common lesion among reactive lesions (29.2%), findings are similar to the results of Pour et al. 19. The total frequency of fibromas in the other surveys was 10% 4, 11.4% 4, 5.5% 11 and 3.16% 16. Jones and Franklin 10 recorded a low percentage of fibromas and a high rate of squamous papillomas. These contradictory results are probably because of different classification systems and histopathological criteria used in different studies. Malignant lesions constituted 2.38% of the lesions in the present study similar to report of Kniest et al. 11 which accounted 2.4%.
Malignant lesions were composed of 7 cases (1.52%) of SCC and 4 cases (0.86%) of salivary gland malignancies. Sixto-Requeijo et al. 25, found the frequency of malignant lesions 3.9% and SCC 3.4% which is higher than our study as in the report of Jones and Franklin 10 which accounted malignant lesions 5.4%. On the other hand, malignant tumors were observed in 1.9% of cases studied by Mendez et al. 16. The total frequency of SCC in the reports of Fierro-Garibay et al. 4 and Franklin and Jones 5 were 0.4% and 0.1%, which are much lower than our assessment.
Conclusion
In general, the prevalence of oral lesions diagnosed in our oral pathology laboratory was relatively similar to other studies. However, odontogenic keratocyst (keratocystic odontogenic tumor) showed high frequency which needs further evaluation and assessment of etiological factors. Likewise, it is important to put emphasis on the specimen sources that vary significantly among oral pathology laboratories. For instance, 80% of specimens in the study conducted by Weir et al. 27 were obtained from a private office, which could shape the occurrence of oral lesions according to the favorite treatment plans of the clinicians. Moreover, diagnostic criteria and classification of lesions are considerably various in different studies which may hinder precise comparison with other studies.
References
1. Al-Khateeb TH. Benign oral masses in a Northern Jordanian population – a retrospective study. The Open Dent J. 2009;3:147-53.
2. Carvalho MV, Iglesias DP, do Nascimento GJ, Sobral A. P. Epidemiological study of 534 biopsies of oral mucosal lesions in elderly Brazilian patients. Gerodont. 2011;28(2):111-5.
3. Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994;77( 3):276-80.
4. Fierro-Garibay C, Almendros-Marqués N, Berini-Aytés L, Gay-Escoda C. Prevalence of biopsied oral lesions in a Department of Oral Surgery. J Clin Exp Dent. 2011;3(2):e73-7.
5. Franklin CD, Jones AV. A survey of oral and maxillofacial pathology specimens submitted by general dental practitioners over a 30-year period. Brit Dent J. 2006;200(8):447-50.
6. Ghasemi Moridani S, Mohtasham Z, Sazesh SF. Correlation between clinical and histopathological diagnosis of oral lesions surgery in the city of Rasht (2000-2002). J Islam Dent Assoc Ir. 2005;17(2):95-9.
7. Ibnerasa S. Retrospective study of variations in the microscopic morphology of dental biopsy specimens received in Pathology Department of Lahore. Pak J Medical Health Sci. 2011;5(3):497-500.
8. Jahanbani J, Morse DE, Alinejad H. Prevalence of oral lesions and normal variants of the oral mucosa in 12 to 15-year-old students in Tehran, Iran. Arch Iran Med. 2012;15(3):142-5.
9. Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. Open Dent J. 2009;(3):42-7.
10. Jones AV, Franklin CD. An analysis of oral and maxillofacial pathology found in adults over a 30-year period. J Oral Pathol & Med. 2006;35(7):392-401.
11. Kniest G, Stramandinoli RT, Avila LFDC, Izidoro AC. Frequency of oral lesions diagnosed at the Dental Specialties Center of Tubarao (SC). RSBO. 2011;8(1):13-8.
12. Koseoglu BG, Atalay B, Erdem MA. Odontogenic cysts: a clinical study of 90 cases. J Oral Sci. 2004;46(4):253-7.
13. Kramer IR, Pindborg JJ, Shear M. Histological typing of odontogenic tumors. 2. ed. Geneva: WHO; 1992.
14. Kramer IR, Pindborg Jr. J, Shear M. Histological typing of odontogenic tumours. Springer; 1992.
15. Luqman M, Al Shabab AZ. A 3 year study on the clinico-pathological attributes of oral lesions in Saudi patients. Inter J Contemp Dent. 2012;3(1):73-6.
16. Mendez M, Carrard VC, Haas AN, Lauxen IDS, Barbachan, Rados PV. A 10-year study of specimens submitted to oral pathology laboratory analysis: lesion occurrence and demographic features. Braz Oral Res. 2012;26(3):235-41.
17. Nakamura T, Ishida J, Nakano Y, Ishii T, Fukumoto M, Izumi H et al. A study of cysts in the oral region. Cysts of the jaw. J Nihon Univ Sch Dent. 1995;37(1):33-40.
18. Philipsen HP. Keratocystic odontogenic tumor. In: Barnes L, Eveson JW, Reichart PA, Sidransky D (eds). WHO classification of tumors; pathology and genetics of head and neck tumors. Lyon: IARC Press; 2005.
19. Pour MAH, Rad M, Mojtahedi A. A survey of soft tissue tumor-like lesions of oral cavity: a clinicopathological study. Iran J Pathol. 2008;3(2):81-7.
20. Ramachandra P, Maligi P, Raghuveer HP. A cumulative analysis of odontogenic cysts from major dental institutions of Bangalore city: a study of 252 cases. J Oral Maxillofac Pathol. 2011;15(1):1-5.
21. Seyedmajidi M, Hamzehpoor M, Bagherimoghaddam S. Localized lesions of oral cavity: a clinicopathologic study of 107 cases. Res J Med Scie. 2011;5(2):67-72.
22. Shahsavari F, Fereidouni F, Farzane Nejad R. The prevalence of oral mucosal lesions and associated factors in Pathology Department of Tehran Cancer Institute of Imam Khomeini Hospital since 2000 to 2010. J Res Dent Sci. 2012;9(2):111-5.
23. Shahsavari F, Khourkiaee SS, Ghasemi Moridani S. Epidemiologic study of benign soft tissue tumors of oral cavity in an Iranian population. J Dentomaxillofac Radiol Pathol Surg. 2012;1(1):10-4.
24. Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in US adults data from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Dent Assoc. 2004;135(9):1279-86.
25. Sixto-Requeijo R, Diniz-Freitas M, Torreira-Lorenzo JC, Garcia-Garcia A, Gandara-Rey JM. An analysis of oral biopsies extracted from 1995 to 2009, in an oral medicine and surgery unit in Galicia (Spain). Med Oral Patol Oral Cir Bucal. 2012;17(1):e16-22.
26. Splieth CH, Sumnig W, Bessel F, John U, Kocher T. Prevalence of oral mucosal lesions in a representative population. Quintessence Int. 2007;38(1):23-9.
27. Weir JC, Davenport WD, Skinner RL. A diagnostic and epidemiologic survey of 15,783 oral lesions. J Am Dent Assoc. 1987;115(3):439-42.
 Corresponding author:
Corresponding author:
Shila Ghasemi Moridani
Postal Address: No 2 – Kashani pour st.
Opposite of Barghe – Alestom – Satarkhan st. – Tehran – Iran
E-mail: smoridani2@yahoo.com
Received for publication: August 21, 2013
Accepted for publication: November 26, 2013
