










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.4 Joinville Out./Dez. 2014
Case Report Article
Multiple fourth molars: surgical treatment in young patient
Franciele Elias Delgado I; Alan Diego Mtanyous Youssef I; Tiago Jonasson I; Alex Landucci I; Lucienne Miranda Ulbrich I; Melissa Rodrigues de Araujo I
I Positivo University – Curitiba – PR – Brazil
ABSTRACT
Introduction: The abnormal development of one or more teeth exceeding the number considered normal is defined as hyperdontia, or supernumerary teeth. Supernumerary teeth are usually diagnosed by routine radiographs, because in most cases they are asymptomatic and do not erupt. The prevalence of supernumerary teeth is low, ranging between 0.1 and 3.8%. Objective: To report a case of multiple non-erupted fourth molars. Case report: Patient M.N.S, 16 years old, female, leucoderma, in good health status attended the dental clinic referred by the orthodontist. On panoramic radiography, the germs of the teeth #18, #28, #38 and #48 were detected and retained. Also, the presence of three forth molars distally to the teeth #18, #28 and #38 were observed. The surgical removal of all third and fourth molars was performed under local anesthesia, in two steps: left and right sides. The patient has been followed for 1 year. Fourth molar prevalence is higher in males (2:1), differing from the patient of this case report. A few cases of multiple supernumerary teeth in non-syndromic patients are reported in the literature. Conclusion: Both early diagnosis and treatment are important to prevent crowding, failure of eruption, displacement of teeth, impairment of orthodontic treatment, gingivitis, and formation of abscess, cysts, and odontogenic tumors.
Keywords: fourth molar; diagnosis; surgical treatment.
Introduction
Hyperdont ia is a development anomaly const ituted by one or more teeth exceeding the norma l tooth number, a lso so-called supernumerary teeth 17,20,22. This alteration affects both the mandible and maxilla 25. The etiology is not fully clarified, and many theories have been proposed. The most accepted theory is that of dental lamina hyperactivity at the initiation phase, producing a greater number of tooth buds 7,21,23,25. The division theory states that a new tooth is formed, known as dichotomy 18,21,28. Other theories cited by literature are: format ion through dental lamina remnants, resulting in extra tooth 28; atavist ic theory (regression to the primary ancestral of Homo sapiens) 7,17; association with disturbs such as Gardner syndrome, cleidocranial dysostosis and cleft lip and palate 19,25; heredity 5,6,21; and inf luence of local factors in odontogenesis such as trauma and inf lammation 7,12,21.
The prevalence of supernumerary teeth ranges from 0.1 and 3.8% in general population 11,13,20,26, with low frequency in primary teeth, around 0.03 to 1.9%. The male/female ratio is 2:1 3,26, evidence gender predominance. The maxilla/ mandible ratio is up to 9:1, mostly in anterior area 21,26. The most frequent tooth areas are: maxillary central incisor, followed by molar (mainly maxillary), pre-molars, lateral incisor, and canine. Also, supernumerary teeth can be classified according to these aforementioned areas. The teeth located at maxillary central incisor area are so-called mesiodens; fourth molars are also called distomolars; the supernumerary tooth located close to molars is called paramolar 17,21. Concerning to shape, the supernumerary can be normal- or conical-shaped (primary teeth), conical-shaped or tuberculate shape (permanent teeth) 16.
The supernumerary teeth are normal ly found by routine radiograph because they are mostly asymptomatic and do not erupt. When erupted (25%), they are promptly diagnosed, and many times, they altered the patient's occlusion 11. The panoramic radiograph is very used for supernumerary diagnosis, mainly in cases of fourth molars 9. Hyperdontia may cause the following problems: crowding, erupt ion failures, tooth displacement, impairment of alveolar bone grafts and implants, impairment of orthodontic treatment, associated pathologies, pericoronarit is, gingivit is, and format ion of odontogenic abscesses, cysts, and tumors 8. The early diagnosis leads to a good prognosis, aiming to avoid worse problems in the surrounding teeth, such as bone resorption 21.
The treatment planning varies according to the patient's condition and tooth position. In most cases, the supernumerary tooth is extracted. Some authors have recommended that it is more favorable to wait the complete root formation of the adjacent teeth, to extract supernumera r y teeth, unless the lat ter i s interfering in the erupt ion chronolog y 7. Accordingly, the interference in tooth chronology demands the immediate extraction 8. Both the removal and maintenance of supernumerary tooth will depend on the cost-benefit ratio for each patient 5.
Case report
Pat ient M.N.S, female, leucoderma, aged 16 years, attended clinical practice referred by the orthodontist to undergo retained third and fourth molars. At anamnesis, the patient did not report any systemic alteration.
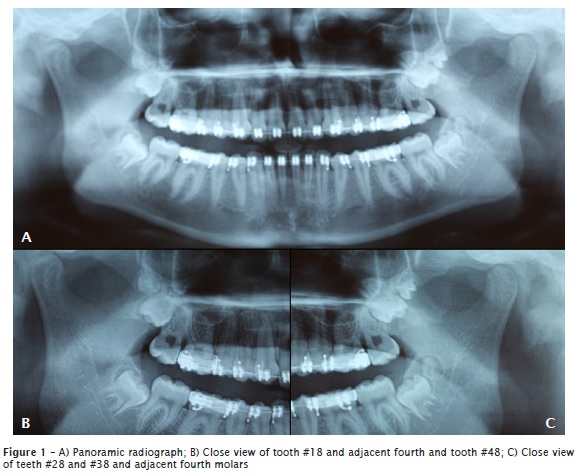
The panoramic radiog raph (figure 1A) showed the teeth #18, #28, #38, and #48 ret a ined, and the presence of the four t h molars retained distally to teeth #18 (figure 1B), #28, and #38 (figure 1C). The surgical planning comprised the extraction of all third and fourth molars at two phases under local anesthesia.
At the first surgical stage the left side third and fourth molars were extracted; at the second stage, the right side third and fourth molars were extracted.
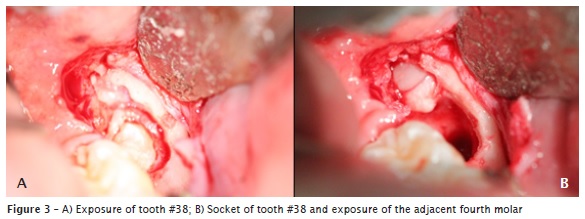
Previous to the surgical procedure, all vital signs of the patient were assessed and were normal. Next, intraoral asepsis was performed with 0.12% chlorhexidine and extraoral asepsis with topical povidone-iodine. Following, local infiltrative subperiostal anesthesia of posterior superior alveolar nerves; local infiltrative submucous anesthesia of greater palatine nerve; anesthesia of inferior alveolar, lingual and buccal nerves were executed. After the incision, a mucoperiosteal flap was raised and osteotomy was performed with the aid of no. 4 round bur at low speed straight handpiece under copious irrigation with 0.9% saline solution (figures 2A and 3A). Third molars were extracted with the aid of dental surgical levers through type II technique.
The third molar sockets allowed seeing the fourth molars and their extraction (figure 2B and 3B). After that, the cavities were cleaned and sutured by simple sutures with nylon thread 4.0. Amoxicillin 875 mg (at every 12 hours for seven days) and ibuprofen 600 mg (at every 8 hours for three days) were prescribed. The suture was removed after seven days and the soft tissues presented good healing, compatible to that of the period.

Discussion
The prevalence of supernumerary molars is 1% according to Stafne 24, 1.9% according to Backman and Wahlin 2, and: two in the maxilla and one in the mandible. Most of the authors reported that supernumerary molars are more frequently found in the maxilla than in mandible, with a percentage of 79% according to Grimanis et al. 9, 88.9% according to Stafne 24, and 91% according to Spauge 23. Cassetta et al. 4 reported that among maxillary supernumerary teeth, 75% are molars.
In this case report, the fourth molars had a smaller size than that of the third molars. Although most of maxillary fourth molars had a size smaller than that of maxillary third molars, a normal size could occur 24. Supernumerary fourth molars may exhibit different shapes. Casseta et al. 4 described a case in which eight out of 13 supernumerary molars had tuberculate shape, while the other five had conical shape.
Some hyperdontia cases are related with syndromes, differently from this case report. Concerning to gender, Watanabe et al. 26 affirmed that male/female ratio is 2:1; according to Yusuf 27 is 9:2. Unlikely, the patient of this case report is female.
Treatment type is based on the patient's clinical condition. Lima et al. 12 stated that the supernumerary treatment options – either surgical or conservative – are based on some parameters, such as age and systemic conditions. Thus, some professionals prefer to follow-up the case, because they have close relationship with the alveolar inferior nerve 1. Notwithstanding, the authors have also indicated the surgical removal with favorable conditions 7,12,13.
Concerning the surgical technique, Kruger 10 cited that fourth molar removal demands the same cautions that of retained third molar because they also cause odontogenic cysts and tumors 17,21, once they occur after the last molar tooth 15. Still, according to Garvey et al. 8, treatment is guided by the location, type, and tooth position. In this present case report, due to the orthodontic need, the fourth molars were extracted together with the third molars at the same surgical step.
Conclusion
Most of supernumerary cases are retained, so that the diagnosis is through routine radiographs. The early diagnosis and treatment are important to prevent problems, such as crowding, eruption failure, tooth displacement, damaging to alveolar bone grafts and implants, associated pathologies, gingivitis, abscesses, and odontogenic cysts and tumors.
Treatment should be tailored according to each case. For the patient of this case report, surgical treatment was referred by the orthodontist, so that both the third and fourth molars did not interfere in tooth movement. All characteristics were favorable for surgical intervention because patient did not exhibit contributory diseases.
References
1. Alvarez LC. Curso de radiologia em odontologia. 4. ed. São Paulo: Santos; 1998. [ Links ]
2. Backman B, Wahlin YB. Variations in number and morphology of permanent teeth in 7- year old Swedish children. Int J Paediatry Dent. 2001 Jan;11(1):11-7.
3. Berthold T, Benemann E. Anomalia no número de dentes: anodontia e supranumerário. Rev Odonto Ciênc. 1996;11(22):101-9.
4. Casetta M, Pompa G, Stella R. Hyperdontia: an epidemiological survey. J Dent Res. 2001 Apr;80(4):1295.
5. Cancio AV, Farias JG, Rodrigues AAA, Gonçalves FMQ, Santos RM. Quarto molar retido: revisão de literatura e relato de casos clínicos. Rev Int Cir Traumatol Bucomaxilofacial. 2004;2:225-9.
6. Cecchi P. Prevalência de anomalias dentárias de desenvolvimento através de radiografias panorâmicas para documentação ortodôntica de pacientes na faixa etária de 8 a 20 anos na cidade do Rio de Janeiro. Rio de Janeiro. Dissertação [Mestrado] – Faculdade de Medicina, Universidade Federal do Rio de Janeiro; 2003.
7. Couto Filho LEG. Supranumerários: revisão de literatura – relato de casos clínicos. BCI Rev Bras Cir Implantod. 2002;9(34):150-5.
8. Garvey MT, Barry HJ, Blake M. Supernumerary teeth-an overview of classification, diagnosis and management. J Can Dent Assoc. 1999;65:612-6.
9. Grimanis GA, Kyriakides AT, Spyropoulos ND. A survey a supernumerary molars. Quintessence Int. 1991 Dec;22(12):989-95.
10. Kruger GO. Cirurgia bucal e maxilo-facial. 5. ed. Rio de Janeiro: Guanabara Koogan; 1984.
11. Kokten G, Balcioglu H, Buyukertan M. Supernumerary fourth and fifth molars: a report of two cases. The Journal of Contemporary Dental Practice. 2003 Nov;4(4).
12. Lima FA, Motisuki C, Bordin MM. Mesiodens: detecção e intervenção cirúrgica precoce. RGO. 2002 Apr-Jun;50(2):69-73.
13. Liu JF. Characteristics of premaxillary supernumerary teeth: a survey of 112 cases. ASDCJ Dent Child. 1995;62:262-5.
14. Luten JR. The prevalance of supernunerary teeth in primary and mixed dentitions. J Dent Child. 1967;34:346-53.
15. Martins Filho PRS, Pereira JC, Piva MR, Ribeiro AO, Dantas LP. Contribuição ao estudo dos quartos molares. Relato de Caso. Rev Port Estomatol Cir Maxilofac. 2008;49:149-52.
16. Mitchel L. An introduction to orthodontics. Oxford: Oxford University Press; 1996.
17. Neville BW, Damm DD, Allen CM, Bouquot JE. Patologia oral e maxilofacial. 2. ed. 2004.
18. Pindborg JF. Pathology of the dental hard tissues. Philadelphia: WB Saunders; 1970.
19. Rocha AML, Columbano Neto J, Souza MMG. Hiperdontia na região de incisivos superiores. J Bras Ortodon Ortop Facial. 2002;7:389-96.
20. Scheiner MA, Sampson WJ. Supernumerary teeth: a review of the literature and four case report. Aust Dent J. 1997;3(4):160-5.
21. Shafer WG, Hine MK, Levy BM. Tratado de patologia bucal. 4. ed. Rio de Janeiro: Guanabara Koogan; 1987.
22. Silva CJ, Santana SI, Silva MCP, Castro MAR. Quarto molar: relato de caso clínico. Rev Bra CIF Periodontia. 2003:1(3):197-200.
23. Spauge JD. Oral pathology. St Louis: Mosby Co.; 1973.
24. Stafne EC. Stafne's oral radiografic diagnosis. 5. ed. Philadelphia: WB. Saunders Co.; 1985.
25. Tommasi AF. Diagnóstico em patologia bucal. 3. ed. São Paulo: Pancast; 2002.
26. Watanabe PCA, Souza JG, Almeida SM, Montebelo Filho A. Estudo radiográfico (ortopantomográfico) da incidência das anomalias dentais de número na região de Piracicaba-SP. Robrac. 1997;6(21):32-8.
27. Yusuf WZ. Non-syndromal multiple supernumerary teeth: literature review. J Can Dent Assoc. 1990;56:417-9.
28. Zhu JF, Marcushamer M, King DL, Henry RJ. Supernumerary and congenitally absent teeth: A literature review. J Clin Pediatr Dent. 1996;20(2):87-95.
 Corresponding author:
Corresponding author:
Melissa Rodrigues de Araujo
Mestrado em Odontologia Clínica – Universidade Positivo
Rua Professor Pedro Viriato Parigot de Souza, n. 5.300 – Campo Comprido
CEP 81280-330 – Curitiba – PR – Brasil
E-mail: melissararaujo@hotmail.com
Received for publication: September 30, 2013
Accepted for publication: November 20, 2013
