










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.1 Joinville Jan./Mar. 2015
Literature Review Article
Developmental anomalies affecting the morphology of teeth – a review
Ashish ShresthaI; Vinay MarlaII; Sushmita ShresthaII; Iccha K MaharjanIII
I Department of Oral Histology and Pathology, College of Dental Surgery, B. P. Koirala Institute of Health Sciences – Dharan – Nepal
II Department of Conservative Dentistry and Endodontics, College of Dental Surgery, B. P. Koirala Institute of Health Sciences – Dharan – Nepal
III Department of Oral Medicine and Radiology, College of Dental Surgery, B. P. Koirala Institute of Health Sciences – Dharan – Nepal
ABSTRACT
Introduction:The development of tooth is a complex process wherein there is series of interactions between the ectoderm and ectomesenchyme. The role of genes in determining the shape and form of a specific tooth has already been defined, the alterations in which can lead to a variety of anomalies in regards to number, size, form, shape, structure, etc. Objective: To review the literature on the developmental anomalies of teeth. Literature review: The developmental anomalies affecting the morphology exists in both deciduous & permanent dentition and shows various forms such as gemination, fusion, concrescence, dilacerations, dens evaginatus, dens invaginatus, enamel pearls, taurodontism or peg laterals. These anomalies have clinical significance concerning esthetics, malocclusion and more importantly predisposing the development of dental caries and periodontal diseases. Conclusion: Knowledge of various diagnostic criteria for identification of these developmental anomalies is significant for early diagnosis and pertinent treatment.
Keywords: developmental anomaly, diagnostic criteria, tooth morphology.
Introduction
The tooth is a specialized part of the human body, understanding the development of which is enigmatic and still challenging. The successful development of tooth depends on a complex reciprocal interaction between the dental epithelium and underlying ectomesenchyme. The interaction involves a complex series of molecular signals, receptors and transcription control systems 73.
Anomaly (Gk, anomalos; irregular) is a deviation from what is regarded as normal 48. Disturbance of the epithelium and mesenchymal interactions can markedly alter the normal odontogenesis leading to the developmental anomaly of teeth. Depending on the developmental stage in which the alteration has taken place, different anomalies could take place e.g. anomalies of number, structure, size and/or shape 46.
Developmental dental anomalies are marked deviations from the normal color, contour, size, number, and degree of development of teeth. Local as well as systemic factors may be responsible for these developmental disturbances. Such influences may begin before or after birth, hence both the dentition might be affected 12.
More than 300 genes have been known to be expressed in teeth that are responsible for odontogenesis 72. Defects in these genes have been found to be one of the reasons for alteration of the morphology of tooth 72.
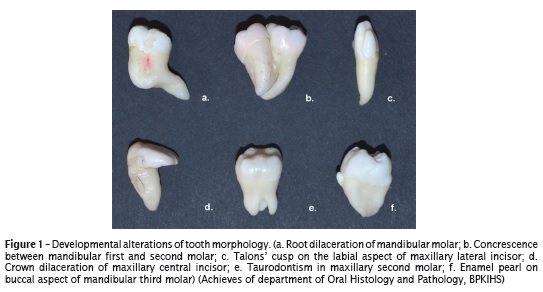
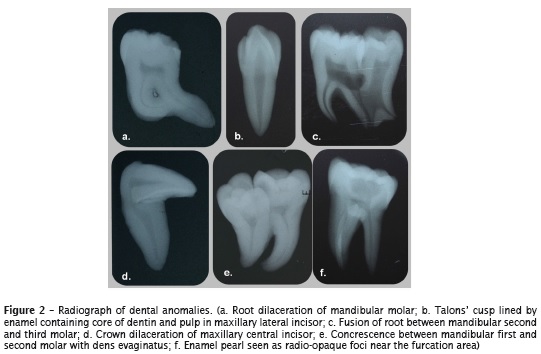
World Health Organization (WHO) has classified "the diseases of oral cavity, salivary glands and jaws" in WHO-International Classification of Disease -10 (WHO-ICD-10) (K00-K14) 23. The anomalies of tooth size and form has been listed under section WHO-ICD -10 (K00.2), which includes concrescence, fusion, gemination, dens evaginatus, dens in dente, dens invaginatus, enamel pearls, macrodontia, microdontia, peg-shaped teeth, taurodontism and tuberculum paramolare (figures 1 and 2).
Understanding the etiology of each dental anomaly is important not only in identification but also to determine the course of the treatment. So, we aim to review the literature regarding various anomalies affecting the tooth and the criteria laid down for its diagnosis.
Description of the anomalies
Gemination
Tannenbaun and Alling in 1963 defined gemination as the formation of equivalent of two teeth from the same follicle, with evidence of an attempt for the teeth to be completely separate 71.
Gemination also described as double teeth, double formations, joined teeth, fused teeth or dental twinning is commonly seen in the maxillary anterior region 17,62.
Geminated teeth arise from an attempt at division of a single tooth germ by invagination, resulting in a single tooth with two completely separated crowns; or a large, incompletely separated crown having single root and root canal 55, which can be confirmed radiographically 68. The anomalous tooth has a larger mesial-distal diameter than normal and is counted as one 33,68. However the total number of teeth in dental arch is otherwise normal 68.
The etiology of geminated teeth remains unknown but nutritional deficiency, endocrine inf luences, infectious/inf lammatory processes, excessive ingestion of medicines, hereditary or congenital diseases, local trauma and ionizing radiation are considered as causative factors 62.
Clinically, gemination occurring in the anterior tooth region causes esthetic problems related to tooth alignment, spacing and arch asymmetry. The presence of deep grooves on the surface makes it susceptible to caries and periodontal problems by facilitating bacterial plaque accumulation. The eruption of adjacent tooth may also be impeded 55.
Fusion
Pindborg defined fusion as the union between dent in and enamel of two or more separate developing teeth 54. There may be complete union to form one abnormally large tooth; union of crowns or union of roots only 47. This anatomic irregularity occurs more often in deciduous dentition with a predilection for the anterior region 68.
Fusion can be complete (total/true fusion) or incomplete (partial/late fusion), depending on stage of development 33,68. If fusion begins before calcification stage, the teeth unite completely and the crown incorporates enamel, dentin, cementum and pulp of both the teeth. Incomplete fusion occurs at a later stage and resultant tooth may exhibit separate crowns and limited to root alone with fused or separate pulp canals. The tooth count reveals a missing tooth where anomalous tooth is counted as one 68, unless where the fusion is occurring with a supernumerary tooth 47.
Various theories have been put forward to explain the etiology of fusion. It has been suggested that when the tooth germs are close together they come in contact and fuse as they develop due to the physical pressure or force generated during growth. Other theories suggested the use of thalidomide or occurrence of viral infection during pregnancy 32. A genetic etiology has also been considered 51. Fusion has been reported with congenital anomalies like cleft lip and also in Xlinked congenital conditions. Some dental and non dental abnormalities including supernumerary teeth, hypodontia, peg-shaped incisors, dens in dente, nail disorders, syndactyly, successional conical teeth, macrodontia and double permanent teeth have been associated with fusion 6,65.
Fusion may cause aesthetic problems and occlusal disturbances due to crowding and irregular morphology, respectively. The presence of deep grooves may predispose to caries or periodontal diseases and cause early pulp exposure. The greater root mass and increased surface area would result in delayed resorption and subsequently cause delayed or ectopic eruption of the permanent successors 47,68.
Concrescence
Concrescence is defined as the cemental union of two adjacent teeth without confluence of the underlying dentin showing independent pulp chambers and root canals 14,18. It may occur during or after the completion of root formation. If the condition occurs during development, it is called true/developmental concrescence and acquired/post inflammatory concrescence if after root formation 18,42.
Concrescence is seen frequently in the posterior maxillary region. The developmental pattern often involves a second molar tooth in which its roots closely approximate to the adjacent impacted third molar 70. Few cases have shown the concrescence of a third molar and a supernumerary tooth 18.
It is suspected that space restriction during development, local trauma, excessive occlusal force, or local infection after development play an important role in the occurrence of concrescence 18,31. True concrescence is attributed to the close proximity of developing roots of the adjacent teeth whereas acquired concrescence may result from a chronic inflammatory response to a non-vital tooth 42. The union may vary from one small site to a solid cemental mass along the entire extent of approximating root surfaces 18.
Radiographic examination is required when concrescence is suspected clinically. However in cases of superimposition of two closely approximated teeth, additional radiographic projections at different angulations may be required 18.
Concrescence should be carefully identified to reduce the risk of complications associated with surgical procedures 31. It may affect the extraction of an adjacent tooth and may fracture the tuberosity or f loor of the maxillary sinus. In such cases, sectioning of tooth should be considered to minimize adverse and unexpected outcomes 42.
Dilaceration
The term dilaceration was first used by Tomes 75 in 1848 and is defined as a deviation or bend in the linear relationship of crown of a tooth to its root 74. It has been listed under section K00.4 of WHO ICD-10 23.
Dilacerations usually occur in the apical third of the root when the anterior teeth are involved, middle third when first molars are involved and coronal third when third molars are involved 39.
Root dilacerations are common than crown dilacerations and occur usually in the posterior region of permanent dentition 25. However crown dilacerations are commonly observed in the permanent maxillary incisors followed by mandibular incisors. Clinically, the maxillary incisors show a lingual deviat ion while the mandibular incisors incline labially. Pulp necrosis and periapical inflammation may be a common finding even in the absence of decay because the bent portion acts as a nidus for bacterial entry due to defective enamel and dentin 3. Some syndromes and developmental anomalies such as Smith Magenis syndrome, hypermobility type of Ehlers-Danlos syndrome, Axenfeld-Rieger syndrome, and congenital ichthyosis have been associated with dilaceration 25,76.
Mechanical trauma (Eg: laryngoscopy and endotracheal intubation) to the primary predecessor tooth is thought to be the most probable cause which results in dilaceration of the crown of developing succedaneous permanent tooth 3,25. The calcified portion of the permanent tooth germ is displaced in such a way that the remainder of the tooth germ forms at an angle 78. Although the prevalence of traumatic injuries to the primary dentition ranges from 11-30%, the incidence of dilacerated permanent teeth is very low 25.
Other possible contributing factors that have been reported include scar formation, developmental anomaly of the primary tooth germ, facial clefting, advanced root canal infections, ectopic development of the tooth germ and lack of space, effect of anatomic structures (Eg. cortical bone of the maxillary sinus, mandibular canal, or nasal fossa, which might deflect the epithelial diaphragm), presence of an adjacent cyst, tumor, or odontogenic hamartoma, mechanical interference with eruption (Eg. from an ankylosed primary tooth that does not resorb), tooth transplantation, extraction of primary teeth, and hereditary factors 25,27,69,76.
There are varying schools of thoughts regarding the criteria for diagnosing root dilacerations. Hamasha et al have considered dilacerations of root toward the mesial or distal direction, if there is a 900 or greater deviation along the axis of the tooth or root, whereas Chohayeb et al have considered a deviation of 200 or more in the apical part of the root 8,21. Chohayeb et al in their study have reported maxillary lateral incisors to be the most commonly dilacerated tooth which could be due to the consideration of distal curvature of the apical third of root as dilaceration rather than a normal anatomy 8,25.
The recognition and diagnosis of dilaceration often requires radiographs taken at various angulations 26. Mesial or distal root curvatures of dilacerated roots are clearly discernible on periapical radiographs. However if the curvature lies in a labial-buccal direction, the central X-ray beam passes almost parallel to the deviating part of the root giving a ‘bulls eye' like appearance 76. Clinical recognition of dilaceration is important because it can lead to non eruption, longer retention of primary predecessor tooth or possible apical fenestration of the buccal or labial cortical plate 76. Dilaceration causes a challenge for endodontic or orthodontic treatment as well as difficulty in extraction 25,39,76.
Dens invaginatus
Dens invaginatus (DI) also known as the pregnant woman anomaly, extensive compound odontoma, and dens in dente, occurs as a consequence of an invagination on the external surface of the tooth crown before calcification 4,28. The invagination ranges from a short pit confined to the crown to a deep invagination into the root, at times extending to or beyond the root apex. The most severe forms are odontome-like and are often termed invaginated odontomes 37. Majority of the cases are encountered in maxilla with the maxillary lateral incisors being commonly affected, followed by central incisors, premolars, canines and molars 20,28. The classical radiographic appearance of coronal DI is a pear shaped invagination of enamel and dentin with a narrow constriction at the opening on the surface of the tooth. The infolding of the enamel lining is more radio-opaque than the surrounding tooth structure aiding easy identification 50.
Oehlers et al grouped coronal DI into three types according to the radiographic appearance 52:
• Type I: An enamel-lined minor form occurring within the confines of the crown not extending beyond the cemento-enamel junction;
• Type II: An enamel-lined form which invades the root but remains confined as a blind sac. It may or may not communicate with the dental pulp;
• Type III A: A form which penetrates through the root and communicates laterally with the periodontal ligament space through a pseudo-foramen. There is usually no communication with the pulp, which lies compressed within the root;
• TYPE III B: A form which penetrates through the root and perforating at the apical area through a pseudo-foramen. The invagination may be completely lined by enamel, but frequently cementum will be found lining the invagination.
A radicular form of dens invaginatus has also been described by Oehlers which is thought to arise due to the proliferation of Hertwig's root sheath. The root of such tooth is enlarged which can be demonstrated radiographically 53.
Infection, trauma or pressure from the growing dental arch is thought to be responsible for dens invaginatus 4,19. A focal failure of growth or a proliferation of a part of the inner enamel epithelium may be involved in the invagination 34,61. Ohlers suggested a distortion of the enamel organ and subsequent protrusion of a part of the enamel organ resulting in the formation of an enamel lined channel 52.
The invagination acts as a channel for entry of irritants and microorganisms; and predispose to the development of dental caries. Since the thickness of enamel is less, pulp necrosis occurs at an earlier age. Coronal DI can also lead to abscess formation, retention of neighboring teeth, cysts, internal resorption, cellulitis etc. 49.
Dens evaginatus
Dens evaginatus (DE) is a developmental aberration of a tooth resulting in formation of an accessory cusp whose morphology has been described as abnormal tubercle, elevation, protuberance, excrescence, extrusion, or a bulge 36. It is also referred to as tuberculated cusp, accessory tubercle, occlusal tuberculated premolar, Leong's premolar, evaginatus odontoma, and occlusal pearl 11,36. Currently, dens evaginatus is the preferred terminology and was first recommended by Oehlers in 1967 52. This uncommon anomaly projects above the adjacent tooth surface, exhibiting enamel covering a dentinal core that usually contains pulp tissue; occasionally having slender pulp horn which extends to various distances within the dentinal core 36,77. The tubercles of dens evaginatus has been differentiated from the cusp of carabelli which is a normal anatomical finding and is differentiated from DE by the absence of a pulp core 36.
A multifactorial etiology combining both genetics and environmental factors has been suggested for the formation of dens evaginatus. Mutations in the human EDA1, EDAR, and EDARADD genes often result in more severe phenotypes resulting in tooth loss and malformation 44. It occurs during the bell stage and is characterized by abnormal proliferation of inner enamel epithelium into the stellate reticulum of the enamel organ 11.
The occurrence of dens evaginatus shows great racial differences with a higher prevalence among people of Mongoloid origin 81. It is commonly associated with the occlusal surface of premolars. Schulze (1987) distinguished the following five types of DE for posterior teeth by the location of the tubercle 36,64.
1. A cone-like enlargement of the lingual cusp;
2. A tubercle on the inclined plane of the lingual cusp;
3. A cone-like enlargement of the buccal cusp;
4. A tubercle on the inclined plane of the buccal cusp;
5. A tubercle arising from the occlusal surface obliterating the central groove.
When dens evaginatus appears in the anterior region, it is usually observed on the lingual surface and is described as a Talon's cusp 36. Mitchell was the first to recognize this anomaly in 1892, which was later named talon by Mellor and Ripa due to its resemblance to an eagle's talon 43,45. It is commonly seen in the maxillary lateral incisors and has been associated with syndromes such as Rubinstein and Taybi, Berardinelli-Seip, Mohr, Ellis-van Creveld, Sturge-Weber and incontinentia pigmenti achromians 67. It varies in size, shape, length and mode of attachment to the crown and ranges from an enlarged cingulum to a large, welldelineated cusp extending beyond the incisal edge of the tooth 37. The cusp is composed of normal enamel and dentin containing varying extensions of pulp tissue. It may connect with the incisal edge to produce a T-form or, if more cervical, a Y-shaped crown contour 20.
Hattab et al classified talons' cusps into three types based on the degree of cusp formation and extension 22:
• Type 1: Talon – refers to a morphologically well-delineated additional cusp that prominently projects from the palatal (or facial) surface of a primary or permanent anterior tooth and extends at least half the distance from cemento-enamel junction to the incisal edge;
•Type 2: Semi talon – refers to an additional cusp of a millimeter or more extending less than half the distance from cemento-enamel junction to the incisal edge. It may blend with the palatal surface or stand away from the rest of the crown;
•Type 3: Trace talon – an enlarged or prominent cingula and their variations, i.e. conical, bifid or tubercle-like. The dens evaginatus or talons cusp may fracture or be abraded as soon as the tooth comes into occlusion, exposing the pulp 11. Hence early recognition of this anomaly and prompt treatment should be instituted to prevent endodontic complications.
Enamel pearls
Enamel which is normally restricted to the anatomic crowns of human teeth may be foundectopically on the root, either as cervical enamel projections or enamel pearls 59,60. Enamel pearl is defined as an ectopic globule of enamel that is firmly attached to the tooth root 9. According to Kupietzky and Rozenfarb (1993) the enamel pearl anomaly was first described in 1824 by Linder and Linder 35. It has been referred to as an enameloma, enamel droplet, enamel nodule, enamel exostoses and enamel globule. It is found commonly on the roots of maxillary molars, especially the third molars adjacent to the furcation or furrow of the root 60.
The structure of the enamel in ectopic enamel projections are characterized as normal, but with considerable variations and irregular features that are most likely related to its ectopic development 58. During normal tooth development, ameloblasts lose their activity after crown formation and become part of Hertwig's epithelial root sheath. Occasionally for unknown reasons, ameloblasts retain their enamel competence, resulting in prolonged (cervical enamel projections) or delayed (enamel pearls) ectopic enamel production 15.
Advanced localized periodontal destruction has been associated with cervical enamel projections and enamel pearl, predisposing to attachment loss 2.
Taurodontism
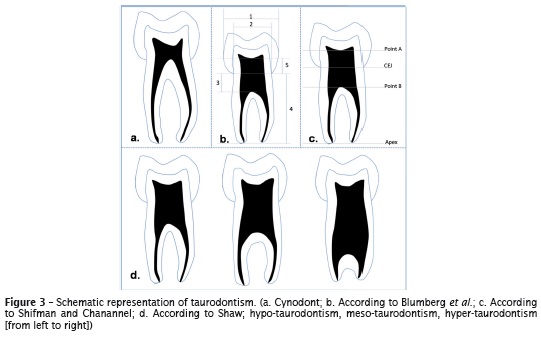
Witkop defined taurodontism as teeth with large pulp chambers in which the bifurcation or trifurcation are displaced apically, so that the chamber has greater apical-occlusal height than in normal teeth and lacks the constriction at the level of cemento-enamel junction (CEJ). The distance from the trifurcation or bifurcation of the root to the CEJ is greater than the occlusal-cervical distance 79.
This anomaly was first reported in the remnants of prehistoric hominids by de Terra in 1903 and by Gorjanovic - Kramberger and Aldoff in 1907 16. Pickerill in 1909 noted this in modern man 41. However the term "taurodontism" was first used by Sir Arthur Keith in 1913 to describe the teeth of prehistoric people, the Neanderthals and Heidelberg 30. He coined this term from the Latin word tauro (for bull) and Greek term dont (for tooth) because of the morphological resemblance of affected tooth to the tooth of ungulates or cud chewing animals.
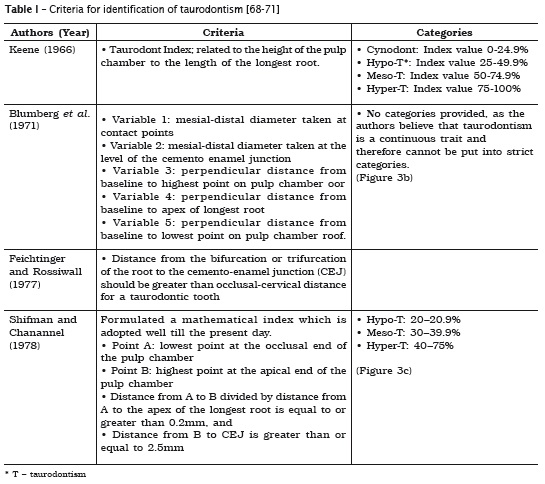
Shaw (1928) has classified taurodontism arbitrarily based on relative degree of apical displacement of floor of pulp chamber into hypo, meso and hyper-taurodontism (figure 3) 66. Various diagnostic criteria have been put forward for the identification of taurodontism which has been summarized in table I5,13,29,63.
Taurodontism primarily affects the molar teeth 38. It occurs as isolated cases but also has been associated with other anomalies. It has been reported in Klinefelter's syndrome, Down's syndrome, Trichodento osseous syndrome, orofacial digital syndrome, Mohr Syndrome or ectodermal dysplasia. It has also been associated with amelogenesis imperfecta, cleft palate, microdontia and dens invaginatus 24,26,41,80.
The etiology of taurodontism is still uncertain, but it is thought to be caused by the failure of Hertwig's sheath to invaginate at the proper horizontal level but other possible etiologies have to be considered including spontaneous mutation and the influence of additional factors such as infection, on the developing tooth 40,57.
Several clinical considerations would be associated with the management of teeth with taurodontism. Extensive length of pulp chambers might create difficulty in location of root canals. Taurodontic molars are suggested to have less resistance to lateral displacing forces compared to cynodont due its smaller surface area and hence are not used as an abutment 40.
Taurodontism
A peg lateral is an undersized, tapered, maxillary lateral incisor 10. The tooth is conical in shape; broadest cervically and tapers incisally to a blunt point. An unusual occurrence is that of a peg-shaped maxillary central incisor. Peg-shaped teeth develop from a single lobe instead of four. The peg-shaped laterals are predominantly genetically determined and can also be caused due to endocrinal disturbances 7. Peg-shaped laterals may be associated with other dental anomalies such as tooth agenesis, canine transposition and overretained deciduous teeth. Studies of identical twins have indicated that missing teeth and peg-shaped lateral incisor might be a varied expression of the same genetic trait 1,10. Early management of the peg-shaped laterals is necessary due to psychological problems in children as well as for the proper development of the stomatognathic system 7.
Conclusion
Although asymptomatic, these dental anomalies can lead to clinical problems which include delayed or incomplete eruption of the normal series of teeth, attrition, compromised esthetics, occlusal interference, accidental cusp fracture, interference with tongue space causing difficulty in speech and mastication, temporomandibular joint pain and dysfunction, malocclusion, periodontal problems and increased susceptibility to caries. The developmental anomalies of teeth show variations and no two anomalies of the same type are alike. So knowledge of various criteria which have been put forward for the identification and classification of the different anomalies is essential to diagnose the condition and institute appropriate treatment.
References
1. Amin F, Asif J, Akber S. Prevalence of peg laterals and small size lateral incisors in orthodontic patients-a study. Pakistan Oral and Dental Journal. 2011;31:88-91. [ Links ]
2. Askenas BG, Fry HR, Davis JW. Cervical enamel projection with gingival fenestration in a maxillary central incisor: report of a case. Quintessence Int. 1992;23:103-7.
3. Asokan S, Rayen R, Muthu M, Sivakumar N. Crown dilacerations of maxillary right permanent central incisor – a case report. J Indian Soc Pedo Prev Dent. 2004;22:197-200.
4. Atkinson SR. The permanent maxillary lateral incisor. Am J Orthod. 1943;29:685-98.
5. Blumberg JE, Hylander WL, Goepp RA. Taurodontism: a biometric study. Am J Phys Anthropol. 1971;34:243-55.
6. Brook AH, Winter GB. Double teeth. A retrospective study of "geminated" and "fused" teeth in children. Br Dent J. 1970;129:123-30.
7. Chanchala HP, Nandlal B. Coexistent peg shaped mandibular central incisors along with maxillary lateral incisors: a rare case. International Journal of Oral & Maxillofacial Pathology. 2012;3:65-8.
8. Chohayeb AA. Dilaceration of permanent upper lateral incisors: frequency, direction, and endodontic treatment implications. Oral Surg Oral Med Oral Pathol. 1983;55:519-20.
9. Darwazeh A, Hamasha AA. Radiographic evidence of enamel pearls in Jordanian dental patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:255-8.
10. Deshpande A, Macwan C. Clinical management of rudimentary supernumerary tooth and pegshaped lateral incisor: a case report. RRJDS. 2013;1:1-4.
11. Echeverri EA, Wang MM, Chavaria C, Taylor DL. Multiple dens evaginatus: diagnosis, management, and complications: case report. Pediatr Dent. 1994;16:314-7.
12. Ezoddini AF, Sheikhha MH, Ahmadi H. The prevalence of dental developmental anomalies: a radiographic study. Community Dent Health. 2007;24:140-4.
13. Feichtinger C, Rossiwall B. Taurodontism in human sex chromosome aneuploidy. Arch Oral Biol. 1977;22:327-9.
14. Foran D, Komabayashi T, Lin LM. Concrescence of permanent maxillary second and third molars: case report of non-surgical root canal treatment. J Oral Sci. 2012;54:133-6.
15. Goldstein AR. Enamel pearls as contributing factor in periodontal breakdown. J Am Dent Assoc. 1979;99:210-1.
16. Gorjanovic-Kramberger K. Uber prismatische molarwurzeln rezenter und diluvialer Menschem. Anat Anz. 1908;32:401-30.
17. Guimarães CLA, Firoozmand LM, Dias Almeida J. Double teeth in primary dentition: report of two clinical cases. Med Oral Patol Oral Cir Bucal. 2008;13:E77-E80.
18. Gunduz K, Sumer M, Sumer AP, Gunhan O. Concrescence of a mandibular third molar and a supernumerary fourth molar: report of a rare case. Br Dent J. 2006;200:141-2.
19. Gustafson G, Sundberg S. Dens in dente. Br Dent J. 1950;8:83-8,111-22,144-6.
20. Guttal KS, Naikmasur VG, Bhargava P, Bathi RJ. Frequency of developmental dental anomalies in the Indian population. European Journal of Dentistry. 2010;4:263-9.
21. Hamasha AA, Al-Khateeb T, Darwazeh A. Prevalence of dilaceration in Jordanian adults. Int Endod J. 2002;35:910-2.
22. Hattab FN, Yassin OM, Al-Nimri KS. Talon cusp in the permanent dentition associated with other dental anomalies: Review of literature and reports of seven cases. J Dent Child. 1996;63:368-76.
23. International Statistical Classification of Diseases and Related Health Problems. 10th Revision (ICD-10). Version for 2010. Available from: URL:http://apps.who.int/classifications/ icd10/browse/2010/en#/K07.3.
24. Ireland EJ, Black JP, Scures CC. Short root, taurodontia and multiple dens invaginatus. J Pedod. 1987;11:164-75.
25. Jafarzadeh H, Abbott PV. Dilaceration: review of an endodontic challenge. J Endod. 2007;33:1025-30.
26. Jafarzadeh H, Azarpazhooh A, Mayhall JT. Taurodontism: a review of the condition and endodontic treatment challenges. Int Endod J. 2008;41:375-88.
27. Kalra N, Sushma K, Mahapatra GK. Changes in developing succedaneous teeth as a consequence of infected deciduous molars. J Indian Soc Pedod Prev Dent. 2000;18:90-4.
28. Karjodkar FR, Mali S, Sontakke S, Sansare K, Patil DJ. Five developmental anomalies in a single patient: a rare case report. Journal of Clinical and Diagnostic Research. 2012;6:1603-5.
29. Keene HJ. A morphologic and biometric study of taurodontism in a contemporary population. Am J Phys Anthropol. 1966;25:208-9.
30. Keith A. Problems relating to the teeth of the earlier forms of prehistoric man. Proc R Soc Med. 1913;6:103-10.
31. Khanna S, Sandhu SV, Bansal H, Khanna V. Concrescence – a report of two cases. International Journal of Dental Clinics. 2011;3:75-6.
32. Kjaer I, Daugaard-Jensen J. Interrelation between fusions in the primary dentition and agencies in the succedaneous permanent dentition seen from an embryological point of view. J Craniofac Genet Dev Biol. 2000;20:193-7.
33. Knezevic A, Travan S, Tarle Z, Sutalo J, Jankovic B, Ciglar I. Double tooth. Coll Antropol. 2002;26:667-72.
34. Kronfeld R. Dens in dente. J Dent Res. 1934;14:49-66.
35. Kupietzky A, Rozenfarb N. Enamel pearls in the primary dentition: report of two cases. ASDC J Dent Child. 1993;60:63-6.
36. Levitan ME, Himel VT. Dens evaginatus: literature review, pathophysiology, and comprehensive treatment regimen. J Endod. 2006;32:1-9.
37. Lorena SC, Oliveira DT, Odellt EW. Multiple dental anomalies in the maxillary incisor region. J Oral Sci. 2003;45:47-50.
38. Madeira MC, Leite HF, Niccoli Filho WD, Simoes S. Prevalence of taurodontism in premolars. Oral Surg Oral Med Oral Patol. 1986;61:158-62.
39. Malcic A, Jukic S, Brzovic V, Miletic I, Pelivan I, Anic I. Prevalence of root dilacerations in adult dental patients in Croatia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:104-9.
40. Mangion JJ. Two cases of taurodontism in modern human jaws. Br Dent J. 1962;113:309- 12.
41. Mark T Jaspers. Taurodontism in Down's syndrome. Oral Surg. 1981;51:632-6.
42. Meer Z, Rakesh N. Concrescence in primary dentition: a case report. IJCDS. 2011;2:19-21.
43. Mellor JK, Ripa LW. Talon cusp: a clinically significant anomaly. Oral Surg Oral Med Oral Pathol. 1970;29:225-8.
44. Miletich I, Sharpe PT. Normal and abnormal dental development. Hum Mol Genet. 2003;12(Spec No 1):R69-73.
45. Mitchell WH. Case report. Dental Cosmos. 1982;34:1036.
46. Mohapatra A, Prabhakar A, Raju O. An unusual triplication of primary teeth: a rare case report. Quintessence Int. 2010;41:815-20.
47. More CB, Tailor MN. Tooth fusion, a rare dental anomaly: analysis of six cases. International Journal of Oral and Maxillofacial Pathology. 2012;4:50-3.
48. Mosby's Medical Dictionary. 8. ed. Elsevier; 2009.
49. Munir B, Tirmazi SM, Majeed HA, Khan AM, Iqbalbangash N. Dens invaginatus: aetiology, classification, prevalence, diagnosis and treatment considerations. Pakistan Oral and Dental Journal. 2011;31:191-8.
50. Mupparapu M, Singer SR. A rare presentation of dens invaginatus in a mandibular lateral incisor occurring concurrently with bilateral maxillary dens invaginatus: case report and review of literature. Aust Dent J. 2004;49:90-3.
51. Nik-Hussein NN, Abdul Majid Z. Dental anomalies in the primary dentition: distribution and correlation with the permanent dentition. J Clin Pediatr Dent. 1996;21:15-9.
52. Oehlers FA, Lee KW, Lee EC. Dens evaginatus, its structure and responses to external stimuli. Dent Pract. 1967;17:239-44.
53. Oehlers FA. The radicular variety of dens invaginatus. Oral Surg Oral Med Oral Pathol. 1958;11:1251-60.
54. Pindborg JJ. Pathology of the dental hard tissues. Philadelphia: W.B. Saunders; 1970.
55. Rajeshwari MR, Ananthalakshmi R. Gemination – case report and review. Indian Journal of Multidisciplinary Dentistry. 2011;1:355-6.
56. Rao PK, Veena KM, Chatra L, Shenai P. Twins on either side – a case report of bilateral gemination. Open Access Scientific Reports. 2012;1:1-2.
57. Reichart P, Quast U. Mandibular infection as a possible aetiogical factor in taurodontism. J Dent. 1975;3:198-202.
58. Risnes S. Ectopic tooth enamel. An SEM study of the structure of enamel in enamel pearls. Adv Dent Res. 1989;3:258-64.
59. Risnes S. The prevalence and distribution of cervical enamel projections reaching into the furcation on human molars. Scand J Dent Res. 1974;82:413-9.
60. Risnes S. The prevalence, location, and size of enamel pearls on human molars. Scand J Dent Res. 1974;82:403-12.
61. Rushton MA. A collection of dilated composite odontomas. Br Dent J. 1937;63:65-85.
62. Santos KSA, Lins CCSA, Almeida-Gomes F, Travassos RMC, Santos RA. Anatomical aspects of permanent geminate superior central incisives. Int J Morphol. 2009;27(2):515-7.
63. Schifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1200 young adult Israeli patients. Community Dent Oral Epidemiol. 1978;6:200-3.
64. Schulze Ch. Anomalien und Missbildungen der menschlichen. Zähne Quintessenz Verlags GmbH. 1987:94-101.
65. Sekerci AE, Sisman Y, Yasa Y, Sahman H, Ekizer A. Prevalence of fusion and gemination in permanent teeth in Coppadocia region in Turkey. Pakistan Oral & Dental Journal. 2011;31:17-22.
66. Shaw JC. Taurodont teeth in South African races. J Anat. 1928;62:476-98.
67. Shirazi AS, Rezaiefar M, Forghani M. A rare case of multiple talon cusps in three siblings. Braz Dent J. 2010;21:463-6.
68. Shrivastava S, Tijare M, Singh S. Fusion/double teeth. JIAOMR. 2011;23:468-70.
69. Stewart DJ. Dilacerate unerupted maxillary central incisors. Br Dent J. 1978;145:229-33.
70. Strecha J, Jurkovic R, Siebert T. Fusion of the 2nd maxillary molar with the impacted 3rd molar. Bratisl Lek Listy. 2012;113:569-71.
71. Tannenbaum KA, Alling EE. Anomalous tooth development: case report of gemination and twinning. Oral Surg Oral Med Oral Pathol. 1963;16:883-8.
72. Thesleff I, Keranen S, Jernvall J. Enamel knots as signaling centers linking tooth morphogenesis and odontoblast differentiation. Adv Dent Res. 2001;15:14-8.
73. Thesleff I. Epithelial–mesenchymal signaling regulating tooth morphogenesis. J Cell Sci. 2003;116:1647-8.
74. Tiecke RW. Pathologic physiology of oral disease. St Louis: Mosby; 1959.
75. Tomes J. A course of lectures on dental physiology and surgery (lectures I-XV). London; 1846-1848.
76. Topouzelis N, Tsaousoglou P, Pisoka V, Zouloumis L. Dilaceration of maxillary central incisor: a literature review. Dental Traumatology. 2010;26:427-33.
77. Vishwanathan S, Nagaraj V, Adimoulame S, Kumar S, Khemaria G. Dens evaginatus in proximal surface of mandibular premolar: A rare presentation. Case Reports in Dentistry. 2012;1-3.
78. Von Gool AV. Injury to the permanent tooth germ after trauma to the deciduous predecessor. Oral Surg Oral Med Oral Pathol. 1973;35:2-12.
79. Witkop CJ Jr. Manifestations of genetic diseases s in human pulp. Oral Surg. 1971;32:278-83.
80. Witkop CJ. Clinical aspects of dental anomalies. Int Dent J. 1976;26:378-90.
81. Yip WK. The prevalence of evaginatus dens. Oral Surg Oral Med Oral Pathol. 1974 Jul;38(1):80-7.
 Corresponding author:
Corresponding author:
Adilson Yoshio Furuse
Al. Dr. Octávio Pinheiro Brisolla, 9-75 – Bauru
CEP 17012-901 – Bauru – SP – Brasil
E-mail: furuse@usp.br
Received for publication: December 1, 2014
Accepted for publication: December 22, 2014
