










Serviços Personalizados
Artigo
 pdf em Português
pdf em Português Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Brasileira de Odontologia
versão On-line ISSN 1984-3747versão impressa ISSN 0034-7272
Rev. Bras. Odontol. vol.73 no.1 Rio de Janeiro Jan./Mar. 2016
ARTIGO ORIGINAL/ESTOMATOLOGIA
Avaliação do traço e estado de ansiedade em pacientes com Glossite Migratória Benigna
Evaluation of trait and state anxiety in patients with Benign Migratory Glossitis
Heron Fernando Souza GonzagaI; Francisco Carlos A. AguiarII; Maria Augusta JorgeIII; Sílvia Angélica JorgeIV; Bruna L. S. PiccianiV; Eliane Pedra DiasVI; Thays Teixeira-SouzaVII Jane TomimoriVIII
I PhD / Discipline of Dermatology, Medical School, UNIMAR, Marília, São Paulo, Brazil
II PhD Department of Oral Pathology, School of Dentistry, UNICAMP, Piracicaba, SP, Brazil
III PhD / Research Center of Association of Education and Culture of Vilhena (Associação Vilhenense de Educação e Cultura - AVEC), Vilhena, RO, Brazil
IV PhD / Department of Nursing, Hospital das Clínicas, UNICAMP, Campinas, SP, Brazil
V PhD, Department of Pathology, Fluminense Federal University, Rio de Janeiro, Brazil
VI PhD, Department of Pathology, Fluminense Federal University, Rio de Janeiro, Brazil
VII Esp, Department of Pathology, Fluminense Federal University, Rio de Janeiro, Brazil
VIII PhD / Department of Dermatology – Escola Paulista de Medicina – UNIFESP, São Paulo, SP, Brazil
RESUMO
Objetivo: avaliar estado e traço de ansiedade em pacientes com glossite migratória benigna (GMB). O estudo consistiu de 78 pacientes com GMB, apresentando ou não ocorrência simultânea de língua fissurada. Um grupo controle de 48 pacientes, sem lesões orais e/ou cutâneas, também foi incluído no estudo. Foi aplicado o Inventário de Traço-Estado de Ansiedade (STAI). Resultados: estado moderado e pontuações de ansiedade-traço foram observados nos grupos. Não houve diferenças estatisticamente significativas nos escores de ansiedade entre os grupos GMB e controle. Conclusão: a ansiedade não parece desempenhar um papel significativo na GMB, apesar dos níveis moderados observados em pacientes com GMB. No entanto, o estado emocional pode ser um fator determinante para as diferentes formas de manifestações de GMB.
Descritores: ansiedade; glossite migratória benigna; língua fissurada.
ABSTRACT
Objective: To assess state and trait anxiety in patients with benign migratory glossitis (GMB). The study consisted of 78 patients with GMB, presenting or not simultaneous occurrence of fissured tongue. A control group of 48 patients without oral lesions and / or skin, was also included in the study. Inventory -Trait State Anxiety (STAI) was applied. Results: moderate state and trait anxiety scores were observed in groups. There were no statistically significant differences in anxiety scores between the GMB and control groups. Conclusion: The anxiety seems to play a significant role in the GMB, despite moderate levels observed in patients with GMB. However, the emotional state can be a determining factor for the different forms of manifestations of GMB.
Descriptors: anxiety; benign migratory glossitis; fissured tongue.
Introduction
Benign migratory glossitis (BMG), also termed as geographic tongue, is a chronic, inflammatory, and immune-mediated oral lesion manifested as irregular areas of filiform papillae loss, circumscribed by whitish, slightly elevated margins 1. The appearance of the tongue in this condition may rapidly vary from red patches of glossitis to healed areas 1. While most epidemiological studies report a mean prevalence of 0.78 to 6.8% 2-5, the etiology and pathogenesis of BMG remain obscure. In addition to psoriasis, it has been implied that BMG is an oral manifestation of this cutaneous disease 6-9, and several authors have suggested the presence of a relationship between psoriasis and BMG, fissured tongue, and geographic stomatitis 6-9. Emotional stress has been reported to be a triggering factor in these conditions. Both psoriasis and BMG have been associated with psychosomatic diseases 1,9,10,11. In 1966, Spielberg developed a self-evaluation scale of anxiety, the State-Trait Anxiety Inventory (STAI), consisting of two distinct scales: Trait-Anxiety and State-Anxiety 12. This instrument was translated and adapted for use in Brazil, by BIAGGIO et al. (1977) 13. The state of anxiety is conceptualized as a transitory emotional state or a condition of the human organism characterized by a consciously noticed unpleasant feeling of tension and apprehension, and an increase in autonomous nervous system activity. This state may vary in time and intensity. The anxiety trait refers to relatively stable individual differences in anxiety, i.e., differences in the tendency to react to situations perceived as threatening, with the elevation of intensity depending on the state of anxiety 12. Several authors have applied STAI to study the relationship between anxiety and diseases and have reported associations with surgical infections, repercussions on fetal circulation during pregnancy, and allergic rhinitis 15,17. To the best of our knowledge, only one study of STAI in patients with BMG has been found in the literature. Therefore, the present study proposed to use STAI to evaluate an association between anxiety and BMG.
Material e Methods
This study included 78 patients with BMG and a control group of 48 individuals without BMG treated at the Dermatological Consultation of Beneficent Association at the University Hospital of Unimar, Marília, São Paulo, Brazil. The protocol was approved by the Ethics Committee, and an informed consent form was signed by each participant. The patients with BMG presented with or without the simultaneous occurrence of fissured tongue, and without the presence of psoriasis. The control group had neither BMG nor fissured tongue or psoriasis, but the most common diseases in this group were acne, ringworm infections, seborrhoeic keratosis, and warts. Of the 78 patients with BMG, there were 47 females (60.2%) and 31 males (39.8%), with an average age of 30.6 (range 12-83). The control group composed of 26 males (54.2%) and 22 females (45.8%), with an average age of 30 (range 11–70). All patients underwent oral mucosal and dermatological examinations performed by an examiner under artificial light conditions. BMG was diagnosed according to the clinical description proposed by BANOCZY et al. 14, while fissured tongue was diagnosed using the clinical description proposed by Redman 5. Anxiety levels were measured using the STAI, which is made up of two distinct scales to measure two distinct concepts of anxiety: state and trait. Each scale contains 20 items having 4 alternatives to each answer. The scale for state anxiety is as follows: 1- almost never; 2- some times; 3- very much; 4- almost always. The scale for trait anxiety is 1-absolutely not; 2- a little; 3- very much; 4- an awful lot. Both, state and trail anxiety scales have items indicating opposite states of anxiety; therefore, these are inverted to count the scores of anxiety, in order words, they are codified to show the 1 = 4; 2 = 3; 3 = 2; 4 = 1. The trait anxiety scale requires individuals to indicate how they generally feel by marking one of the 4 alternatives, whereas the state anxiety scale requires individuals to indicate how they feel at a given time by selecting one of the 4 alternatives 12. Statistical analysis was conducted using the Mann-Whitney test in order to assess differences between state and trait anxiety scores between the two groups. A p value of <0.05 was considered statistically significant.
Results
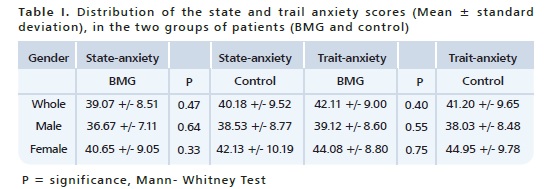
Moderate scores of state and trait anxiety were determined in each group. Statistical significance notwithstanding a slight score correlation was observed between state and trait anxiety and age in the control and BMG groups. The average scores obtained for state and trait anxiety were higher in females in both groups. No statistically significant differences in state and trait anxiety scores were found between the BMG group and the control group (Table I). A total of 50 out of 78 (64%) patients in the BMG group presented with fissured tongues along with BMG, one of who also had with migratory stomatitis. Twenty-eight patients presented with BMG only. The state and trait anxiety scores in the groups of patients with BMG and fissured tongue as well as the group with BMG only, were not significantly different compared with those in the control group. State anxiety scores were lower, while trait anxiety scores were higher in patients with BMG and fissured tongue compared with those in the control group; however, the differences between the two groups were not statistically significant. The scores of state and trait anxiety were higher in the group with BMG and fissured tongue than those in the group with BMG only. In addition, the difference between the two groups was not statistically significant. The condition was asymptomatic in 56 patients (75%), while 19 patients (25%) reported burning sensation triggered by the intake of spicy, hot, or citric foods. The scores of state anxiety in the symptomatic patients were lower than those in the asymptomatic patients, while trait anxiety scores were higher in the symptomatic patients than those in the asymptomatic patients. However, no statistically significant differences were observed in the scores between the groups. A total of 53 patients (68%) were unaware of the presence of an oral lesion, while 25 patients (32%) reported as having knowledge of the presence of an oral lesion. State and the trait anxiety scores were higher, albeit not significantly, in the group with BMG, but unaware of the presence of a lesion, compared to the group that was aware of the presence of the lesion.
Discussion
Several studies have demonstrated associations between BMG and psoriasis, suggesting that BMG is a form of oral psoriasis 6-8. Emotional stress and other environmental factors may be responsible for different types of diseases. To the best of our knowledge, only one study has identified anxiety in patients with BMG. Hence, this study aimed at evaluating the association between anxiety and BMG, using STAI. Data from both males and females were considered, in this study, based on reports from other studies in the literature demonstrating the influence of gender on anxiety.
In accordance with the findings reported by BIAGGIO et al. 13, the state and trait anxiety scores in the present study were found to be higher in the females than in males. Although moderate scores of state and trait anxiety were observed in both groups in the present study, no statistically significant differences were noted. The same was true when comparing scores between the control group, and the 2 groups of patients with BMG presenting with and without fissured tongue, respectively. A study by Alikhani et al. (2014) reported positive correlations between BMG, and psychological or physiologic factors of anxiety, using STAI and salivary cortisol levels 11. Gonzaga et al. (2014) showed that emotional stress was an environmental factor contributing to the occurrence of psoriasis and BMG 10. These data reinforce the role of emotional stress as a triggering factor for both diseases, and the authors have indicated that it would have been interesting to have submitted these patients to a full emotional evaluation with psychological tests. A disease is considered multifactorial when the phenotype results from the interaction of multiple genes (polygenes) placed in different loci along with the environment 18. BMG is considered as a multifactorial disease, which needs a genetic component to express itself. Both psoriasis and BMG have been classified as polygenic diseases. In the case of psoriasis, the involvement of a genetic loci was determined in chromosomes 6p, 17q, 4q, 2p, 8q, and 20p 19-20, whereas in BMG, investigations have been performed in locus 6p only 7. Environmental factors may have a role in the expression of these diseases. Although anxiety does not seem to play a predominant role, it could be one of the factors triggering this condition.
In the present study, the control group also presented with moderate anxiety scores, but probably did not possess the genetic predisposition for the diseases. The oral condition mostly associated with BMG, is fissured tongue 3,19. Sixty-four percent of the BMG patients, in this study, presented with this condition. The scores of state and trait anxiety, in the group with BMG and fissured tongue, were higher than those in the group with BMG only; however the difference was not statistically significant. Genetic and environmental facts have been known to contribute to the "transformation" of BMG to fissured tongue 20. However, some authors suggest that the fissured tongue is a permanent form of GMB, those proposed by CHOSACK et al. 2, who suggested that fissured tongue develops more as sequel to than simultaneously with the development of BMG. Although stress and anxiety could be important factors for the development of this condition, we did not observe any such associations in the present study, due to the lack of significant differences in the state and trait anxiety scores between patients with and without the presence of symptoms. Similarly, no significant differences in anxiety scores were observed between patients who were aware of having lesion and those who were not. BMG is a benign disease, and contrary to psoriasis, it is asymptomatic most of the time.
Conclusion
In conclusion, the results of the present study show that anxiety, as an environmental factor, may not play a significant role in the development of BMG, despite the fact that moderate scores levels of anxiety were observed in patients with BMG. However, emotional state may be a determining factor in the occurrence of different manifestations of psoriasis and BMG. Therefore, understanding the effect of emotional state may aid in determining different approaches in managing patients with BMG and psoriasis.
Referências
1. Goswami M, Verma A, Verma M. Benign migratory glossitis with fissured tongue. J Indian Soc Ped od Prev Dent. 2012;30:173-5. [ Links ]
2. Chosack A, Zadik D, Eidelman E. The prevalence of scrotal tongue and geographic tongue in 70, 359 israeli school children. Community Dent Oral Epidemiol. 1974;2:253-7.
3. Darwazeh AMG, Pillai K. Prevalence of tongue lesions in 1013 Jordanian dental outpatients. Community Dent Oral Epidemiol. 1993;21:323-4.
4. Gonzaga HFS, Costa CAS, Oliveira MRB, et al. Estudo da prevalência da língua geográfica e fissurada em escolares de Araraquara. Rev Odontol UNESP. 1994;23:339-46.
5. Honarmand M, Farhad-Mollashahi L, Shirzaiy M, et al. Geographic Tongue and Associated Risk Factors among Iranian Dental Patients. Iran J Public Health. 2013;42:215-9.
6. Femiano F. Geographic tongue (migrant glossitis) and psoriasis. Minerva Stomatol. 2001;50:213-7.
7. Gonzaga HF, Torres EA, Alchorne MMA, et al. Both psoriasis and benign migratory glossitis are associated with HLA-Cw6. Brit J Dermatol. 1996;135:368-70.
8. Picciani BL, Carneiro S, Sampaio AL, et al. A possible relationship of human leucocyte antigens with psoriasis vulgaris and geographic tongue. J Eur Acad Dermatol Venereol. 2014 Aug 29. doi: 10.1111/jdv.12691. [Epub ahead of print]
9. Picciani B, Silva-Junior G, Carneiro S, et al. Geographic stomatitis: an oral manifestation of psoriasis? J Dermatol Case Rep. 2012;6:113-6.
10. Gonzaga HF, Chaves MD, Gonzaga LH, et al. Environmental factors in benign migratory glossitis and psoriasis: Retrospective study of the association of emotional stress and alcohol and tobacco consumption with benign migratory glossitis and cutaneous psoriasis. J Eur Acad Dermatol Venereol. 2014; Jul 30. doi: 10.1111/jdv.12616 [Epub ahead of print].
11. Alikhani M, Khalighinejad N, Ghalaiani P, et al. Immunologic and psychologic parameters associated with geographic tongue. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118:68-71.
12. Spielberger CD. Anxiety and behavior. 1st ed. New York: Academic Press; 1966.
13. Biaggio AMB, Natalício L, Spielberger CD. Desenvolvimento da forma experimental em português do inventário de ansiedade traço-estado (IDATE) de Spielberger. Arq Bras Psicol Apl. 1977;29:31-4.
14. Banoczy J, Szabo L, Csiba A. Migratory glossitis: a clinical – histologic review of seventy cases. Oral Surg 1975;39:113-21.
15. Andrade TGCS, Caron-Ruffino M, Ruffino-Neto A. Ansiedade e infecções cirúrgicas. Medicina. 1994;27:233-41.
16. Sjöström K, Valentin L, Thelin T. Maternal anxiety in late pregnancy and fetal hemodynamics. Eur J Obs Gynecol and Reprod Biol. 1997; 74:149-55.
17. Addolorato CA, Ancova C, Capristo E. State and trait anxiety in women affected by allergic and vasomotor rhinitis. J Psych Res. 1999;46:282-9.
18. Elder JT, Nair RP, Henseler T. The genetics of psoriasis 2001: the odyssey continues. Arch Dermatol. 2001;137:1447-54.
19. Kovac-Kavcic M, Skaleric U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. J Oral Pathol Med. 2000;29:331-5.
20. Kulla-Mikkonen A. A familial study of fissured tongue. Scand. J Dent Res. 1988;96:366-75.
 Endereço para correspondência:
Endereço para correspondência:
Heron Fernando de Sousa Gonzaga
Av. Rio Branco, 1132, Sala 122
Marília/SP, Brasil - CEP:175002-000
e-mail: herongonzaga@yahoo.com.br
Recebido: 18/09/2015
Aceito: 26/10/2015
