










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Brasileira de Odontologia
versão On-line ISSN 1984-3747versão impressa ISSN 0034-7272
Rev. Bras. Odontol. vol.73 no.4 Rio de Janeiro Out./Dez. 2016
Original Article/Operative Dentistry
Dental bleaching with and without LED/Laser association: a split-mouth controlled study
André Manoel Lima da Fonseca,I; Inger Campos TuñasII; Fábio VidalI; Fábio Ramôa PiresI; Lucio Souza GonçalvesI
I Post graduation program in Dentistry, Faculty of Dentistry, Estácio de Sá University, Rio de Janeiro/RJ, Brazil
II Department of Preventive and Social Dentistry, Faculty of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro/RJ, Brazil
ABSTRACT
Objective: The aim of this study was to compare dental color changes after a one-session tooth bleaching procedure using 35% hydrogen peroxide with and without hybrid light (LED/diode laser) activation. Material and Methods: 20 volunteers were included in a split-mouth controlled clinical trial. A 35% hydrogen peroxide gel was applied directly on the buccal surface and adjacent areas of all upper anterior teeth. The six teeth were divided into two groups: the upper right incisors and canine were submitted to the tooth bleaching with the gel and the hybrid light (LED/diode laser) while the left incisors and canine were submitted to tooth bleaching with only the gel. Dental color was measured with a visual color scale and a spectrophotometer at five different moments: initial appointment, immediately after prophylaxis, and 14, 30 and 180 days after bleaching. Results: The comparison between the results of both treatments (with and without LED/laser) did not show any statistically significant differences (p > 0.05; Wilcoxon test) neither for objective (spectrophotometer) nor for subjective evaluations (visual color scale). Conclusion: The results of the present study showed that there are no differences in dental color changes between dental bleaching with gel and LED/Laser activation and dental bleaching with only gel.
Descriptors: Hydrogen peroxide; Tooth bleaching; Laser; Clinical trials as topic.
Introduction
Although the use of light sources to enhance the effects of tooth bleaching has been suggested over the years, there is no consensus on its effectiveness.1 In fact, when it comes to bleaching and color stability, recent evidence has shown that light activation produces results similar to those obtained with only chemical activation, regardless of the bleaching protocol tested.2-5 Current research has also shown some controversy when it comes to how different wave lengths,6 light sources,3,2,7 gel concentrations1,8,9 and bleaching techniques10,11 influence the color alterations and whether there is a recommended protocol that stands out among the many bleaching techniques available.12,13
Dental bleaching studies is commonly performed using split-mouth design, which divide the mouth within a patient.14-16 This study design was introduced by Ramfjord et al.17 evaluated the efficacy of two periodontal procedure randomly allocating the methods in half of each patient's dentition. Generally, randomized controlled trials have as the unit of randomization the individual. However the split-mouth trials utilize body parts as the unit of randomization, such as the hemi-arch of each patient. Split mouth design has as main advantage the patients act as their own controls, excluding inter-subject variability.18
The aim of this split-mouth study was to compare the color changes after a one session tooth bleaching protocol with 35% hydrogen peroxide with and without hybrid light (LED/diode laser) treatment.
Material and Methods
The study was previously approved by the local ethics committee (project number 0031.0.308.000-10). All participants were informed about the objectives and possible risks and/or adverse effects of the study and signed a consent form.
Twenty volunteers, 4 males and 16 females, aged between 18 and 30 years-old, participated in the study. Inclusion criteria were: absence of caries, dental fillings, dentin hypersensitivity, cervical lesions, clinically visible periodontal disease and periradicular lesions on the teeth involved in the study; VPI (visible plaque index) and GBI (gingival bleeding index) values lower than 25%; absence of heavy discoloration on the studied teeth, such as those associated with exogenous substances (medications, fluorosis and endodontic treatment); without submission to any other dental bleaching protocol in the previous 2 years and absence of any previous history of allergic reactions related to substances used in tooth bleaching. Smokers and former smokers, as well as, women that were pregnant or breastfeeding were not included in the study.
Each subject underwent one 45-minute in-office tooth bleaching session right after dental prophylaxis. A split-mouth design was chosen and the dental arch was divided into two groups: RS (right side group – included the right central incisor, lateral incisor and canine) and LS (left side group – included the left central incisor, lateral incisor and canine). The isolation technique included the use of cotton rolls, lip retractors (Arcflex™, FGM, Joinville, Brazil), gauze above the dorsum of the tongue and disposable saliva ejector and the gingival tissue were isolated with the use of a blue-colored light-cured composite (Top Dam™, FGM, Joinville, Brazil). The 35% hydrogen peroxide bleaching gel (Whiteness HP Maxx™, FGM, Joinville, Brazil) was applied over the buccal, proximal and occlusal enamel from the right second bicuspid to the left second bicuspid with the aid of a small brush (Microbrush®, Vigodent, Rio de Janeiro, Brazil). The gel was left on the dental surfaces for 15 minutes and during this period it was re-brushed 3 or 4 times to release any possible oxygen bubbles and to allow maximum contact with the dental surface. After this period the gel was removed with the aid of a disposable saliva ejector and the dental surface was cleaned with gauze. This process was repeated 3 times, totaling 45 minutes of bleaching therapy.
A hybrid light system (Whitening Lase II®, DMC, São Paulo, Brazil) was used to activate the bleaching gel, but only on the right arch. The LED/LASER system was composed of a LED unit (470nm wave length), an infrared laser (808nm wave length), and InGaAIP (indium gallium aluminum phosphide), a semi-conductive material. The light was applied for a total of 3 minutes (1 minute light activation for each of the 3 applications of the bleaching gel), according to the manufacture's recommendation.
In order to avoid any unwanted light activation of the gel on the left side, a customized protection barrier made of dental impression material (Optosil™, Haraeus Kulzer, Germany) was applied over the left arch during light activation. The barrier stretched from the central incisor to the second bicuspid. Also a piece of aluminum sheet was trimmed and placed over the silicon barrier, to ensure that the light would only activate the gel on the right side.
Tooth shade was registered, by 2 different methods, subjective and objective, at 5 different moments: initial appointment; after dental prophylaxis and 14, 30 and 180 days after bleaching. The subjective method included the use of a dental color scale (VITA classic™, Vita Zahnfabrik, Sackingen, Germany). The first two color registers (initial appointment and after prophylaxis) were performed by the main researcher (AMLF) while the post bleaching evaluations were made by two other calibrated professionals, blinded to the bleaching technique was used in each dental arch. The subjective color analysis was done with the dental color scale prearranged from lighter to darker shades (B1, A1, B2, D2, A2, C1, C2, D4, A3, D3, B3, A3,5, B4, C3, A4, C4) and positioned about 1 cm from the buccal surface of the upper anterior teeth and about 40 cm from the observer. The teeth were evaluated following a standard sequence (right canine, right lateral incisor, right central incisor, left central incisor, left lateral incisor and left canine) for a maximum of 10 seconds for each tooth. Patients were scheduled for the appointments in the same dental office with adequate light and were asked to wear a neutral grey bib during the appointment.
The objective dental color evaluation was performed with a spectrophotometer (Vita Easyshade™, Vita-Zahnfabrik, Germany) previously calibrated for the colors of the VITA classical™ shade scale. In order to standardize the points of interest for color register, a silicon impression was taken and used as a positioning guide for the spectrophotometer tips. The six upper anterior teeth were submitted to silicon precision impression (Optosil®, Haraeus Kulzer, Germany) and six holes with the same diameter as the spectrophotometer tip (6 mm) were made with the use of a circular blade similar to the ones used for soft tissue biopsies (soft tissue punch). The orientation guides were made in the medium third of the buccal surface of the studied teeth according to the protocol previously described.19 The spectrophotometer collects information about luminosity, chroma and shade, converting them into numeric values. The difference between the values obtained before and after tooth bleaching (ΔE) at the 5 different predetermined moments allowed the comparison between the techniques. The equipment was calibrated before each measurement.
Descriptive statistics were used to compare the ΔE values between groups. Paired t tests were performed for the analysis of the differences in ΔE means between groups, within groups and between the 5 different moments of the measurements. The effect of the bleaching according to both subjective and objective evaluations was compared by means of Wilcoxon test. Significance level was set at 5% and the confidence interval for the estimates was set at 95%. Bonferroni's test was used for the adjustment of multiple comparisons among different periods. All statistical tests were performed using the Statistical Package for the Social Sciences (SPSS) software, version 17.0 (IBM, Chicago, IL, USA).
Results
None of the 20 patients presented any side effects or abnormal reaction during tooth bleaching. Five patients complained of transitory dental sensitivity after bleaching and those were successfully managed with topical fluoride gel and mouthwashes with 0.05% sodium fluoride.
The comparison between the results of both treatments (with and without LED/laser) did not show any statistically significant differences (p > 0.05; Wilcoxon test) neither for the objective nor for the subjective evaluations.
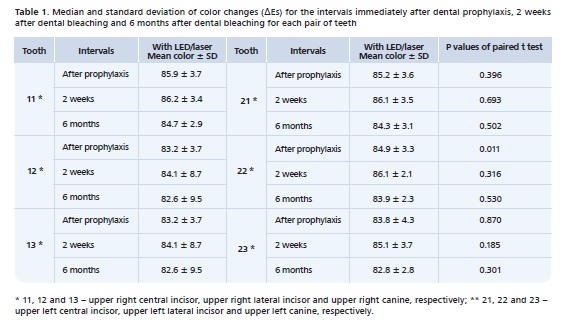
Table 1 shows a summary of the measures observed in the RS (with LED/laser) and LS (without LED/laser) groups for central incisors, lateral incisors and canines, comparing values of color change, for each tooth pair at the following evaluations: after prophylaxis, two weeks and 6 months after tooth bleaching. Comparison between the two groups in each individual evaluation, showed that there was a significant statistical difference between the means of the lateral incisors after prophylaxis (p = 0.011; paired t test). There were no statistical significant differences in the remaining comparisons of ΔEs means (p > 0.05; paired t test).
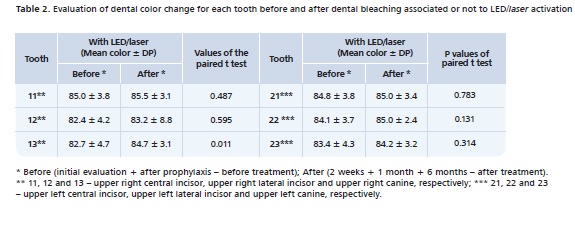
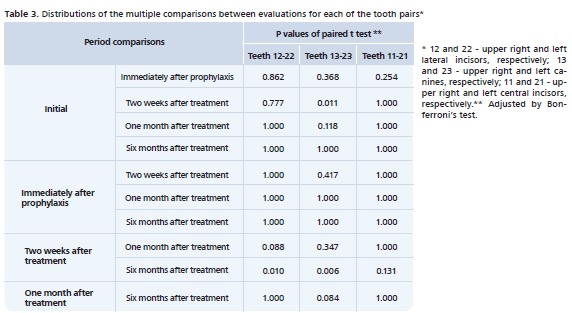
Comparative analysis of the means within each group (with and without LED/laser), before (initial + after prophylaxis) and after (2 weeks + 1 month + 6 months) treatment were performed for all studied teeth. Statistically significant differences were found only for the upper right canine (p = 0.011; paired t test) (Table 2). Multiple comparisons were also performed among all evaluations for each pair of teeth. We observed a statistically significant difference for the lateral incisors between 2 weeks and 6 months after treatment (p = 0.01; paired t test) and for the canines between initial evaluation and 2 weeks after treatment (p = 0.011) and between 2 weeks and 6 months after treatment (p = 0.006) (Table 3). There were no statistical significant differences for the central incisors (Table 3).
Discussion
Clinical and experimental studies using light sources in tooth bleaching have shown conflicting results, especially due to differences in methodological assays.1,7 Selection of adequate methods for the comparative analysis and the dental color change analysis is essential to allow the comparison between different products and techniques. Split mouth studies seem to be the most adequate study design to evaluate in-office tooth bleaching and have frequently been used in recently published clinical trials.4,10,20 In the present study the same subject received both techniques (with and without LED/laser activation) in the same session according to the study protocol previously described.
Dental color changes are mainly evaluated using the direct visual inspection method with the aid of a color scale, due to its simplicity and practicality.21 However, since dental color evaluation is sensitive to multiple factors such as: the type and intensity of the light source available; the selected teeth and the experience and calibration of the observer, standardization is essential and non-subjective methods should be prioritized.22 To minimize the impact of such factors, in the present study, all the subjective evaluations were performed by 2 calibrated researchers in the same dental office with adequate light.
In order to allow a more accurate color change evaluation, an objective method was also used to measure any color alterations. The use of spectrophotometers, colorimeters and computed-based image analysis can be preferred to subjective methods, as they reduce inter-individual variability, allow standardization and offer the possibility of quantitative analysis.8,21 In this study, the spectrophotometer Easyshade™ was used due to the fact that this equipment is pre-calibrated to be used with the Vita classic scale, the same color scale used for the subjective evaluations. Therefore, a comparison between the results obtained by both methods was possible. A silicon guide with an opening in the medium third of the coronary portion was used to allow the operators to reproduce precisely the color evaluation process in every tooth involved in the study in each follow up session. We believe that previously published studies that did not use any guide make them more susceptible to inaccurate results when it comes to color change evaluations.20,23,24
Light activated sources for in-office dental bleaching of vital teeth have been used aiming to accelerate the oxidation- reduction reaction of the bleaching gel.6,25 However, there are still several questions about the real effectiveness of these auxiliary methods, including light/heat sources (such as LED or laser).1-3,5,7,11,20,26 The lack of consensus in the literature about the most effective wave length and the controversies about the heating produced by high potency lasers and LEDs, confirm the need for more studies about the effects of light sources.13 Recently published experimental studies (in vitro and clinical studies) have shown that there does not seems to be any statistically significant advantages in using light sources when it comes to bleaching effectiveness.3,5,11,20,27 Another recently published study concluded that light activation sources are unnecessary to bleach teeth.2 On the other hand, there is evidence that light sources, especially infrared light and CO2 laser, can improve the efficacy of different bleaching agents.4,6,28
Clinical Significance
The results of the present study suggest that the use of light sources during in-office dental bleaching with 35% hydrogen peroxide does not lead to better results regarding color changes when compared to chemical activation only. Thus, a simpler operative protocol should be recommended for clinicians.
Conclusion
The results of the present study showed that there were no differences, regarding dental color changes, after dental bleaching using light sources (LED/Laser) in comparison with dental bleaching using only the gel.
References
1. He LB, Shao MY, Tan K, Xu X, Li JY. The effect of light on bleaching and tooth sensitivity during in-office vital bleaching: a systematic review and meta-analysis. J Dent. 2012;40(8):644-53. [ Links ]
2. Almeida LC, Riehl H, Santos PH, Sundfeld ML, Briso AL. Clinical evaluation of the effectiveness of dif/ferent bleaching therapies in vital teeth. Int J Periodontics Restorative Dent. 2012;32(3):303-9.
3. Polydorou O, Wirsching M, Wokewitz M, Hahn P. Three-month evaluation of vital tooth bleaching using light units-a randomized clinical study. Oper Dent. 2013;38(1):21-32.
4. Henry RK, Bauchmoyer SM, Moore W, Rashid RG. The effect of light on tooth whitening: a split-mouth design. Int J Dent Hyg. 2013;11(2):151-4.
5. Nutter BJ, Sharif MO, Smith AB, Brunton PA. A clinical study comparing the efficacy of light activated in-surgery whitening versus in-surgery whitening without light activation. J Dent. 2013;41(Suppl 5):3-7.
6. Luk K, Tam L, Hubert M. Effect of light energy on peroxide tooth bleaching. J Am Dent Assoc. 2004;135(2):194-201.
7. Hein DK, Ploeger BJ, Hartup JK, Wagstaff RS, Palmer TM, Hansen LD. In-office vital tooth bleaching - what do lights add? Compend Contin Educ Dent. 2003;24(4A):340-52.
8. Joiner A. The bleaching of teeth - a review of the literature. J Dent. 2006;34(7):412-9.
9. Ritter AV. In-office tooth bleaching. J Esthet Restor Dent. 2006;18(3):168-9.
10. Zhao K, Zong L, Zhang Q, Att W. Clinical comparison between two bleaching techniques: a 180-day follow-up study. Quintessence Int. 2013;44(8):601-7.
11. Auschill TM, Schneider-Del Savio T, Hellwig E, Arweiler NB. Randomized clinical trial of the efficacy, tolerability, and long-term color stability of two bleaching techniques: 18-month follow-up. Quintessence Int. 2012;43(8):683-94.
12. Kugel G, Papathanasiou A, Williams AJ 3rd, Anderson C, Ferreira S. Clinical evaluation of chemical and light-activated tooth whitening systems. Compend Contin Educ Dent. 2006;27(1):54-62.
13. Buchalla W, Attin T. External bleaching therapy with activation by heat, light or laser - a systematic review. Dent Mater. 2007;23(5):586-96.
14. Machado LS, Anchieta RB, dos Santos PH, Briso AL, Tovar N, Janal MN, Coelho PG, Sundfeld RH. Clinical comparison of at-home and in office dental bleaching procedures: a randomized trial of a split-mouth design. Int J Periodontics Restorative Dent. 2016;36(2):251-60.
15. Bernardon JK, Ferrari P, Baratieri LN, Rauber GB. Comparison of treatment time versus patient satisfaction in at-home and in office tooth bleaching therapy. J Prosthet Dent. 2015;114(6):826-30.
16.de Freitas PM, Menezes AN, da Mota AC, Simões A, Mendes FM, Lago AD, et al. Does the hybrid light source (LED/laser) influence temperature variation on the enamel surface during 35% hydrogen peroxide bleaching? A randomized clinical trial. Quintessence Int. 2016;47(1):61-73.
17. Ramfjord SP, Nissle RR, Shick RA, Cooper H, Jr. Subgingival curettage versus surgical elimination of periodontal pockets. J Periodontol. 1968; 39(3):167-75.
18. Lesaffre E, Philstrom B, Needleman I, Worthington H. The design and analysis of splitmouth studies: what statisticians and clinicians should know. Stat Med. 2009;28(28):3470-82.
19. Marson FC, Sensi LG, Vieira LCC, Araújo E. Clinical evaluation of in-office dental bleaching treatments with and without the use of light-activation sources. Oper Dent 2008;33(1):15-22.
20. Mondelli RF, Azevedo JF, Francisconi AC, Almeida CM, Ishikiriama SK. Comparative clinical study of the effectiveness of different dental bleaching methods -two year follow-up. J Appl Oral Sci. 2012;20(4):435-43.
21. Guan YH, Lath DL, Lilley TH, Willmot DR, Marlow I, Brook AH. The measurement of tooth whiteness by image analysis and spectrophotometry: a comparison. J Oral Rehabil. 2005;32(1):7-15.
22. Watts A, Addy M. Tooth discolouration and staining: a review of the literature. Br Dent J. 2001;190(6):309-16.
23. Al Shethri S, Matis BA, Cochran MA, Zekonis R, Stropes M. Clinical evaluation of two in-office bleaching products. Oper Dent.2003; 28(5):488- 95.
24. Zekonis R, Matis BA, Cochran MA, Al Shetri SE, Eckert GJ, Carlson TJ. Clinical evaluation of in-office and at-home bleaching treatments. Oper Dent. 2003;28(2):114-21.
25. Wetter NU, Barroso MC, Pelino JE. Dental bleaching efficacy with diode laser and LED irradiation: an in vitro study. Lasers Surg Med. 2004;35(4):254-8.
26. Mena-Serrano AP, Garcia E, Luque-Martinez I, Grande R, Loguercio AD, Reis A. A Single-Blind Randomized Trial About the Effect of Hydrogen Peroxide Concentration on Light-Activated Bleaching. Oper Dent. 2016 (in press).
27. Soares DG, Basso FG, Hebling J, de Souza Costa CA. Concentrations of and application protocols for hydrogen peroxide bleaching gels: Effects on pulp cell viability and whitening efficacy. J Dent. 2014;42(2):185-98.
28. Tavares M, Stultz J, Newman M, Smith V, Kent R, Carpino E, et al. Light augments tooth whitening with peroxide. J Am Dent Assoc. 2003;134(2):167-75.
 Endereço para correspondência:
Endereço para correspondência:
Lucio Souza Gonçalves
e-mail: luciogoncalves@yahoo.com.br
Recebido: 08/01/2016
Aceito: 09/09/2016
