










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Brasileira de Odontologia
versão On-line ISSN 1984-3747versão impressa ISSN 0034-7272
Rev. Bras. Odontol. vol.74 no.1 Rio de Janeiro Jan./Mar. 2017
Original Article/Hospital Dentistry
Dental surgeons' perceptions of hospital dentistry
Constanza MarínI; Michelly Herika Nunes dos SantosII; Elisabete Rabaldo BottanII
I Dentistry course - University of Itajaí Valey - Univali, Itajai, SC, Brazil; Dentistry Department - University of the Region of Joinville - Univille, Joinville, SC, Brazil
II Dentistry Course - University of Itajaí Valey - Univali, Itajai, SC, Brazil
ABSTRACT
Objective: to analyze the dental surgeons' perceptions of their professional practice in the hospital environment. Material and Methods: an exploratory study, using qualitative and quantitative approaches. The study population consisted of 72 dentists registered with the Associação Brasileira de Odontologia do Alto Vale do Itajaí (Brazilian Dentistry Association of the Alto Vale do Itajaí) - ABOAVI. The data collection was carried out using a script-guided interview. The data were then analyzed by creating categories based on the interviewees' responses. Results: 47 evocations were considered, distributed into three categories. The two categories most frequently cited to justify the importance of the dental surgeon's (DS) practice in the hospital environment were: prevention of onset and/or aggravation of pathologies, and integrality of patient care. Conclusion: for this group of professionals, the practice of the DS in the hospital environment is perceived as positive, and is in accordance with the vision of integral care that will contribute to improving the health of hospitalized patients.
Keywords: Human resources in dentistry; Oral health; Dental hospital unit.
Introduction
H ospital dentistry is defined as a set of preventive, diagnostic, therapeutic and palliative actions in oral health, which are carried out in hospital institutions within the context of a multidisciplinary team. The treatment of hospitalized patients, within an integral approach, requires a multiprofessional team, and this conduct favors the improvement of the patient's clinical status.1-7
Dental treatment can generate better conditions for hospitalized patients, resulting in shorter hospitalization times and a reduction of costs for the health services. This professional therefore assumes a new role in the challenge to combine efforts, working effectively within the hospital environment.2,3,7-10
However, the performance of the DS in the hospital environment is still incipient.4,5 Among the possible reasons for this low level of participation, two factors stand out. On one hand, there is a lack of information from health professionals about the practice of the DS in the hospital.5,11 On the other, there is the temerarious attitude among dental surgeons to take on the routine activities of the hospital environment, which are more complex than those required in the dental office.11
In order to broaden the field of discussions on hospital dentistry, this study analyzes the perceptions of DS on their professional practice in the hospital environment.
Material and Methods
The study was characterized as an exploratory investigation, using qualitative and quantitative approaches.
The study population was comprised of 72 dental surgeons registered with the Associação Brasileira de Odontologia do Alto Vale do Itajaí (Brazilian Dentistry Association of the Alto Vale do Itajaí) - ABOAVI. The sampling plan was non-probabilistic and the sampling was done by convenience, the sole inclusion criteria being the DS's willingness to participate, by signing of the Informed Consent Form.
The data collection took place in July 2016. To obtain the data, a single interviewer made the initial contact with the professionals in their work environments, explaining the objectives and methodology of the research, and asking for their agreement to participate in the study. Those who agreed signed an Informed Consent Form (ICF), and an appointment was scheduled for the interview.
The interview consisted of a guiding question: What is your opinion of the practice of the DS in the hospital environment? The participants were also asked their age, area of expertise, and length of time in the career.
The data were recorded anonymously, to maintain the confidentiality of the interviewees' identities. The data were organized using the following procedures: a preliminary reading, which consisted of skimming the twenty-eight documents produced by the participants. This aim of this phase was to identify the evocations expressed by the respondents. For this, all the expressions compatible with the study were marked. Confused or non-pertinent ideas were discarded. Next, a new reading was carried out, grouping the evocations by similarity of meaning. This resulted in a total of fifty evocations, which were distributed in categories. The analysis was carried out by three researchers, in consensual form.
The respondent's views were then drawn up in a table, and the frequency of occurrence of each category was calculated.
The project was submitted to and approved by CEP/UNIVALI under Opinion 1,224,541 (CAAE 47435215.9.0000.0120) and all the ethical research precepts were followed.
Results
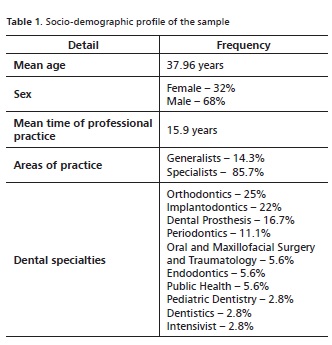
Of the 72 DSs registered in the ABOAVI, 28 participated in this study, i.e., 39%. The sociodemographic profile of the sample is shown in Table 1.
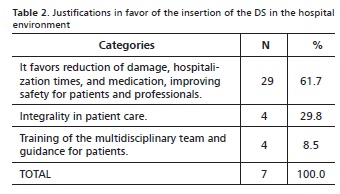
The participants' opinions were analyzed based on 47 evocations that expressed a positive idea in relation to the participation of the DS in hospital teams in carrying out procedures beyond those related to Oral and Maxillofacial Surgery and Traumatology. Three other evocations were also identified that referred to the difficulties faced in this insertion process. These related to aspects of the integration of the DS with the hospital teams, and patients' acceptance of them. The need for and importance of the insertion of the DS in the hospital environment were justified by the study participants, as shown in Table 2.
Discussion
This exploratory study analyzes perceptions of the DS's in relation to their professional practice in the hospital environment. Discussion of this subject in Brazil, in the last fifteen years, has been systematic and continuous. The insertion of the DS in the hospital environment is the result of a new paradigm in the profession.
Historically, from the time Dom Pedro II, through an Imperial Government decree, created the first course in Dentistry on October 25, 1884, the work of the DS focused on the treatment of diseases, such as caries and periodontal disease, with procedures carried out at dental offices. Later, in 1968, with the activities of the Brazilian Society of Oral and Maxillofacial Surgery and Traumatology, this branch of dentistry was recognized by the National Dentistry Surveillance Service (SNFO), leading to the creation of a new working space, besides the dental office, for dentists specializing in Oral and Maxillofacial Surgery. Holders of this qualification became part of clinical teams of hospitals, albeit using a different approach from that currently sought in Hospital Dentistry.12
Later, in the 21st century, the Code of Dental Ethics, approved by Resolution CFO-42, on May 20th, 2003, in its article 18, chapter IX, discusses hospital dentistry. However, what we have seen in practice is that hospitals, as well as many professionals, are not able to fulfil this goal.2,10,13,14 This failure is partly because the legal resolutions that define the concept of Hospital Dentistry, and the attributions of the DS, are very recent.15,16
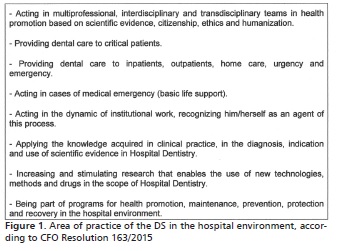
In 2015, CFO Resolution 162 was published, which recognizes the practice of hospital dentistry by the DS, and CFO Resolution 163, which defines Hospital Dentistry and the role of the dental surgeon. Thus, it was only recently that the competences required of a qualified professional were defined, and only then did courses in Hospital Dentistry and Hospital Management begin to adapt accordingly, producing a guideline for the recruitment of these professionals. Thus, based on Resolution 163 of the CFO16, it can be affirmed that DSs who are qualified to work in the hospital setting now have wide range of opportunities available to them (Figure 1).
The discussions on the need to include the DS in multiprofessional teams in the hospital environment have been largely based on two main streams of clinical evidence. One indicates that the patient may present gram-negative bacteria in the oral cavity due to periodontal disease or extensive caries, which can lead to various systemic complications. The other view is that that the patient's general health conditions may affect their oral conditions during hospitalization.2-5,9,14,17,18
For the participants of this study, the justifications given for the inclusion of the DC in the hospital environment included aspects related to clinical evidence that are consistent with some of the items set forth in CFO Resolution 163/2015, which outlines areas of practice of the DC with qualification in Hospital Dentistry.16 Various participants stated that monitoring the patient's oral condition throughout the hospitalization period is fundamental for the quality of life of these subjects. The following excerpts from the transcription of the interviews show the respondents' views. In order to maintain the anonymity of the subjects, at the end of each transcribed evocation were annotated the letter S (Subject) and the number corresponding to the analyzed document (for example S1).
"It is very important, because it brings more comfort to the patient in cases of oral lesions, pain, scratches and traumas in intubation, etc. The performance of the dental surgeon in the hospital environment reduces the prevalence of pneumonia in these cases, decreasing hospitalization times spending on antibiotics." (S1)
"Their practice is very important, because there are various diseases that can worsen if the oral health is not in good condition, especially in patients in ICUs, whose immunity is low. Oral bacteria can cause systemic problems." (S5)
"I'm in favor, as it adds more knowledge about the oral diseases that a hospitalized patient can present." (S17)
"It's of the utmost importance. The occurrence of tooth avulsions during intubations or prosthesis fractures, the appearance or worsening of periodontal diseases and lacerations of the tongue and mucous membranes are not uncommon. I believe it is a great advance and a necessity that needs to be put into practice." (S21)
In addition to the aspects directly related to the clinical approach, the other series of justifications cited by the participants of this research related to the vision of health care in the integral sense. The care of a hospitalized patient requires a holistic approach that, in order to be put into practice, requires the combined action of various professionals. It is believed that the DSs participating in this research, when referring to the integrality of the inpatient care, were basing their views on article 2, item a, of CFO Resolution 163/2015, where it defines that the DS may "work in multiprofessional, Interdisciplinary and transdisciplinary teams in health promotion, based on scientific evidence, citizenship, ethics and humanized care".16
Thus, it is important to emphasize that the integrality of health care, as a principle of the Unified Health System (SUS), requires democratic interactions on the part of the subjects, which must be based on autonomy, the exercise of solidarity, and the recognition of freedom of choice.19 It is therefore necessary to reflect on the true sense of integrality, in which the actions go beyond the sum of the individual work of each professional.
Working as part of a multiprofessional health team means overcoming the fragmentation of actions. However, it is known that the exercise of this practice, in the daily routine, is complex. The incorporation of knowledge from other fields, the integration of different areas of knowledge, and the need to act from an interdisciplinary perspective, whether in the hospital or in other spaces of health care, are goals that are under development, and that still face many obstacles. This difficulty was identified in three of the respondents' evocations, which referred to the problems of integration between the DS and the hospital teams. It can be inferred that these dental surgeons perceive this to be a practice that requires a sharing of actions, knowledge and responsibilities, but that also faces various obstacles. Some respondents pointed out a possible resistance, among the medical profession, towards the practice of the dental surgeon as a member of the multidisciplinary team. This situation corroborates the findings of Marín et al.,1 who investigated the opinions of different health professionals relating to the participating of the DS in multiprofessional teams in the hospital environment.
Based on the literature, it can be emphasized that the participation of the DS in the hospital team, even with the growing recognition of public policies regarding the importance of his/her integration in the different levels of health care, is still incipient. 4-11,13,18,20,21 Among the possible causes of this restricted performance are the lack of information given to health professionals, and the lack of a suitable structure in hospitals.10,11,21
On the other hand, there is also the courageous attitude of some DSs to take up the challenge of practicing in the hospital setting. In order to work in this environment, besides having an excellent general clinical training, the DS mas also have an indepth knowledge of clinical medicine, general diseases, diagnoses, and the treatments applied, and must be willing to work in conjunction with other professionals, adopting principles of multiprofessional work.1,5-7,13
To minimize these barriers, it is essential that approaches be established between different categories of health professionals, for further discussions on the meaning of teamwork at different levels of health care. In addition, it is necessary, during the academic training, for the future DS to be encouraged to consider practicing in the hospital setting. Professional bodies should also promote symposia colloquiums addressing aspects of Hospital Dentistry, in order to broaden understanding of this area of practice of the DS.
Favorable attitudes towards the inclusion of the DS as a proactive member of the health team in the hospital environment demonstrate that the respondents had knowledge of hospital dentistry. The members of the research understood that those qualified in Hospital Dentistry can perform various clinical procedures, as well as guiding patients and health professionals in oral health care. However, despite the positive view of the practice of the dentist in the hospital, the interviewees were still not clear as to the need for the DS to be involved in the areas of critical care, basic life support, and research.
The need for and importance of hospital dentistry, at the present stage of the discussions, is unquestionable. However, as in any process of change or innovation, the concrete experience of this role of the DS still generates a series of questions, and faces a number of barriers. We therefore believe that study contributes to disseminating the vision of dentistry professionals on this theme, and encouraging the expansion of these discussions into different spaces and with different subjects.
It should be pointed out that the small number of participants does not undermine the validity of this study. According to Marconi and Lakatos22, the low return is a disadvantage that is common with this type of research. However, this does not remove from the investigation its internal validity, i.e. its results are reliable, but should not be extrapolated beyond the group investigated. It should also be kept in mind that this research is exploratory, and that the principles of qualitative research were adopted for the data collection and analysis. These characteristics allow us to affirm that despite the limited sample, the results can clarify relevant aspects of this theme.
Conclusion
Based on the data analyzed, and on the study proposal, it can be affirmed that for this group of professionals, the performance of the DS in the hospital environment is perceived in a positive way, which is in line with the vision of integral health care for hospitalized people. The respondents evidenced forms of practice of the DS that correspond to what is set forth in CFO Resolution 163/2015.
Acknowledgment
To the ProBIC (Scientific Initiation Scholarship Program).
References
1. Marín C, Bottan ER, Maçaneiro CAR. Visão de profissionais da saúde sobre a inserção do cirurgião-dentista no ambiente hospitalar. Rev Pesq Saúde [online] 2015;16(1):24-8. Disponível em:< http://www.periodicoseletronicos.ufma.br/index. php/revistahuufma/article/view/4072/2154>. Acesso em: 26 set. 2016. [ Links ]
2. Batista AS, Siqueira JSS, Silva Jr. A, Ferreira MF, Agostini M, Torres SR. Alterações orais em pacientes internados em unidades de terapia intensiva. Rev Bras Odontol. 2014;71(2):156-9.
3. Pinheiro TS, Almeida TF. A saúde bucal em pacientes de UTI. Revista Bahiana de Odontologia 2014; 5(2):94-103. Disponível em: < https: //www5.bahiana.edu.br/index.php/odontologia/article/viewFile/367/325>. Acesso em: 14 out. 2016.
4. Rocha AL, Ferreira EF. Odontologia hospitalar: a atuação do cirurgião-dentista em equipe multiprofissional na atenção terciária. Arq Odontol. 2014;50(4):154-60.
5. Sousa LVS, Pereira AFV, Silva NBS. A atuação do cirurgião-dentista no atendimento hospitalar. Rev. Ciênc. Saúde [online] 2014;16(1):39-45. Disponível em:< http:// www.periodicoseletronicos.ufma.br/index.php/ rcisaude/article/view/3406/2845>. Acesso em: 14 out. 2016.
6. Euzébio LF, Viana KA, Cortines AAO, Costa LR. Atuação do residente cirurgião- dentista em equipe multiprofissional de atenção hospitalar à saúde materno- infantil. ROBRAC. 2013; 21(60):16-20.
7. Schmitt BHE, Lazzari JM, Dona KC, Marín C. Condición oral de los pacientes cardiopatas hospitalizados y la importância de um odontólogo en el hospital. Rev. Fac. Odontol. UNNE [online] 2011;IV(1):11-8. Disponível em:<http://odn. unne.edu.ar/revfounne/V4N12011/index.html>. Acesso em: 17 out. 2016.
8. Albuquerque DMS, Bedran NR, Queiroz TF, Salomão Neto T, Senna MAA. A importância da presença do cirurgião-dentista na equipe multidisciplinar das unidades de tratamento intensivo. Revista Fluminense de Odontologia [online]. 2016 [acesso 29 Set. 2016]; XXII(45). Disponível em: <http://www.ijosd.uff.br/index. php/n37/article/view/330/212>.
9. Gaetti-Jardim E, Setti JS, Cheade MFM, Mendonça JCG Atenção odontológica a pacientes hospitalizados: revisão da literatura e proposta de protocolo de higiene oral. RBCS. 2013;11(35):31-6.
10. Aranega AM, Bassi APF, Wayama MT, Esteves JC, Junior IRG. Qual a importância da Odontologia Hospitalar? Rev Bras Odontol. 2012;69(1): 90-3
11. Wayama TM, Aranega AM, Bassi APF, Ponzoni D, Garcia Jr IR. Grau de conhecimento dos cirurgiões-dentistas sobre Odontologia Hospitalar. Rev Bras Odontol. 2014;71(1):48-52.
12. França, S. CTBMF: praticada desde os tempos mais remotos. Jornal APCD [online]. Jan. 2016[acesso 21 Out. 2016]50(705):16-7. Disponível em:<http:// www.apcd.org.br/jornal/Jornal_2016_01/index.html>.
13. Silva Junior MF, Gonçalves CL, Côco LSA, Miclos PV, Oliveira MA, Gomes MJ. A organização da Odontologia no contexto hospitalar da região metropolitana da Grande Vitória/ES. Rev Bras Pesqui Saúde. 2013;15(2):104-11.
14. Gomes SF, Esteves MCL. Atuação do cirurgião dentista na UTI: um novo paradigma. Rev Bras Odontol. 2012; 69(1):67-70.
15. Conselho Federal de Odontologia. Resolução nº 162, de 03 de novembro de 2015. Reconhece o exercício da Odontologia Hospitalar pelo CD. Diário Oficial da União, Brasília, seção 1, p.167; 16 novembro de 2015.
16. Conselho Federal de Odontologia. Resolução nº 163, de 09 de novembro de 2015. Conceitua a Odontologia Hospitalar e define a atuação do cirurgião-dentista habilitado a exercê-la. Rio de Janeiro: CFO; 09 novembro de 2015.
17. Nunes RJA, Arruda FP, Lima Junior JL. Análise da redução de pneumonia nosocomial no CTI após inclusão do cirurgião dentista na equipe multidisciplinar. Rev Odontologia (ATO). 2014;14(1):28-35.
18. Freitas AR, Xavier A, Sales-Peres A, Sales-Peres SHC. Análise de ensaios clínicos randomizados e a relação entre doença periodontal e diabetes mellitus. Rev Odontol UNESP. 2010;39(5):299-304.
19. Pires VMMM, Rodrigues VP, Nascimento MAA. Sentidos da integralidade do cuidado na saúde da família. Rev Enferm UERJ. 2010;18(4):622-7.
20. Schmitt BHE, Damos MN, Guzzi SH. Demanda do serviço de odontologia clínica do hospital Santa Catarina de Blumenau - SC. Salusvita. 2012;31(3):203- 12.
21. Amaral COF, Marques JA, Bovolato MC, Parizi AGS, Oliveira A, Straioto FG. Importância do cirurgião-dentista em Unidade de Terapia Intensiva: avaliação multidisciplinar. Rev Assoc Paul Cir Dent. 2013;67(2):107-11.
22. Marconi MDA, Lakatos EM. Técnicas de pesquisa: planejamento e execução de pesquisas, amostragens e técnicas de pesquisas, elaboração, análise e interpretação de dados. São Paulo: Atlas; 2012.
 Endereço para correspondência:
Endereço para correspondência:
Constanza Marín
e-mail: constanzamarin4@gmail.com
Recebido: 16/11/2016
Aceito: 01/31/2017
