










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Brasileira de Odontologia
versão On-line ISSN 1984-3747versão impressa ISSN 0034-7272
Rev. Bras. Odontol. vol.74 no.1 Rio de Janeiro Jan./Mar. 2017
Literature Review/Oral Surgery
Prophylactic removal of unerupted asymptomatic third molars: is it justifiable?
Marlus da Silva PedrosaI; Evelyn Bianca Soares SilvaI; Thais Oliveira CordeiroI; Luiz Gustavo Fernandes Lima OliveiraII; Rodrigo Richard da SilveiraIII; Cláudio Heliomar Vicente da SilvaIV; José Guilherme Férrer PompeuV
I Department of Dentistry, DeVry Facid – DeVry Education Group, Terezina, PI, Brazil
II Private Practice, Luiz Gustavo Aesthetic Dentistry and Oral Implantology, Terezina, PI, Brazil
III Department of Restorative Dentistry, Federal University of Minas Gerais – UFMG, Belo Horizonte, MG, Brazil
IV Department of Prosthetic Dentistry and Maxillofacial Surgery, Federal University of Pernambuco – UFPE, Recife, PE, Brazil
V Department of Restorative Dentistry, Federal University of Piauí – UFPI, Terezina, PI, Brazil
ABSTRACT
Objective: to review the literature currently available on the evidence that does or does not justify the prophylactic extraction of unerupted asymptomatic third molars. Material and Methods: the electronic databases PubMed, Capes Periodicals, Web of Science and Scopus were searched from November to December 2016 by two authors, simultaneously, using as search terms: Terceiro Molar/Molar, Third AND Extração Profilática/Prophylatic Removal OR Prophylatic Extraction. We included articles from original research and clinical trials published in English and Portuguese. No limits were applied to the date of publication. Review articles and clinical case reports were removed. Results: we identified 13 studies that addressed, at some aspect, the prophylactic removal of unerupted asymptomatic third molars. The results of this literature review which alluded to the potential for the formation of pathological alterations in asymptomatic third molars are conflicting; While some justifies the prophylactic procedure based on the possible formation of associated lesions, other scientific evidence does not support such practice. Conclusion: in view of the conflicting viewpoints found in the literature, the prophylactic removal of asymptomatic third molars requires case-by-case evaluation of each patient, and the decision-making process, regarding the retention versus the prophylactic removal of these teeth should be based on scientific evidence combined with the clinical experience of the professional.
Keywords: Oral surgery; Third molar; Unerupted tooth; Disease prevention.
Introduction
The extraction of third molars is one of the most common procedures in the clinical practice of dentists worldwide. It is estimated that, in the United States, approximately 10 million impacted teeth are extracted annually from approximately 5 million individuals, generating a revenue of 3 billion dollars.1,2 In England and Wales, extractions of third molars between 1995 and 1996 totaled approximately 5.2 million pounds.3
Prophylactic extraction, the most common reason for extraction of third molars,4 is widely recognized by a considerable number of dental surgeons.2,5 This fact is based on the association of these teeth with oral pathological changes such as pericoronitis, periodontal problems, caries in third or second molars, different types of odontogenic cysts and tumors as well as crowding of the lower incisors.6-14
The scientific literature also mentions other reasons to justify this procedure, considering the fact that these teeth do not always play a functional role in the oral cavity as well as an increased risk for postoperative complications, pain and discomfort when their surgical removal is performed in more advanced aged patients.15-21 However, other studies suggest that the lower third molars should not be removed prophylactically in some cases2,14,22-23 and vigilant monitoring of these teeth is more appropriate strategy.24
Debate about indications for prophylactic removal of impacted third molars remains heated.11 The decision-making process regarding retention versus prophylactic removal of these teeth should be based on the available scientific evidence.25 However, the literature is lacking in studies to support adequate clinical decision-making regarding prophylactic extraction of third molars.14 This study aimed to review the literature currently available on scientific evidence that does or does not justify the prophylactic extraction of unerupted asymptomatic third molars.
Material and Methods
For the purpose of this study, we followed guidelines provided by Moher et al.26 in Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement.
Identification and Selection of Relevant Research
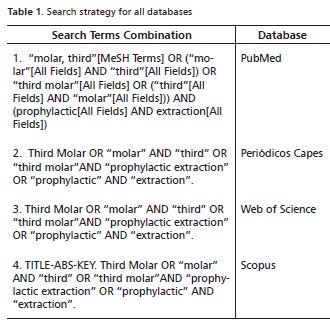
An exploratory bibliographic search was conducted from January to February of 2017 using the electronic databases: Public Medline (PubMed), Periódicos da Capes, Web of Science and Scopus. Two authors performed the search employing the term Third Molar in combination with Prophylactic removal OR Prophylactic Extraction (Table 1). Inclusion criteria were: original research articles and clinical trials published in Portuguese and English. No limits were applied to the year of publication.
Studies were identified and duplicates were removed. Subsequently, titles and abstracts were screened for relevance, considering the exclusion criteria. Next, the remaining studies were obtained in full-text and were screened using the self-same criteria, the eligible the ones being included in this review. We removed review studies, clinical case reports, articles not available in fulltext, and publications that did not address the prophylactic removal of unerupted asymptomatic third molars. Eligible studies also had their reference lists screened following the specified criteria for the eligible ones.
Data Collection and Analyses
All the selected articles addressed the relationship between third molars and pathological changes and included the following parameters: authorship, year of publication, country of publication, type of study, sample size (and age), outcomes measured, relevant data and results, and study considerations.
Based on the findings of the studies, we determined the following themes for critical analysis of the results: characteristics of the studies, prophylactic removal of third molars and implications for practice. Yet, considering our study design and its findings, we presented the section "study limitations".
Results
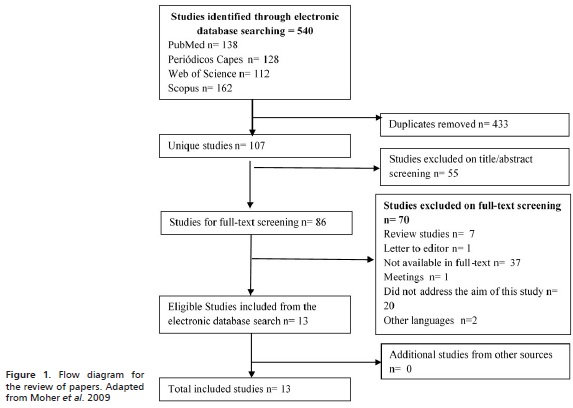
For this systematic review, the initial electronic search yielded a total of 540 titles found in the databases: PubMed, Periódicos da Capes, Web of Science and Scopus. 433 studies were excluded for duplication and the remaining 107 unique papers were screened for relevance to this study. 55 publications were excluded after reading their titles and abstracts. Then, the 52 remaining documents were obtained in full-text and assessed for eligibility in consideration of the prophylactic removal of unerupted asymptomatic third molars. After reading the documents in full text, 13 studies were included (Figure 1 and Table 2). No studies from reference lists were added due to their either not being eligible or not having come up on the database search.
Characteristics of the Studies
We identified 13 studies that addressed, in some respect, the prophylactic removal of asymptomatic third molars. The 13 documents fell into several different categories: retrospective (n = 5), prospective (n = 4), histopathological (n = 2), cross-sectional (n = 1), and histologic and immunohistochemical (n = 2).
According to our findings, we identified only six studies published at sporadic intervals within a ten-year time frame: 2001 (n = 1), 2005 (n = 1), 2006 (n = 1), 2008 (n = 2), e 2009 (n = 1). In the last six years, seven studies were published: 2011 (n = 2), 2013 (n = 2), 2015 (n = 1) and 2016 (n = 2) The results indicated the need for future research on the prophylactic extraction of unerupted asymptomatic third molars.
Prophylactic Removal of Unerupted Asymptomatic Third Molars
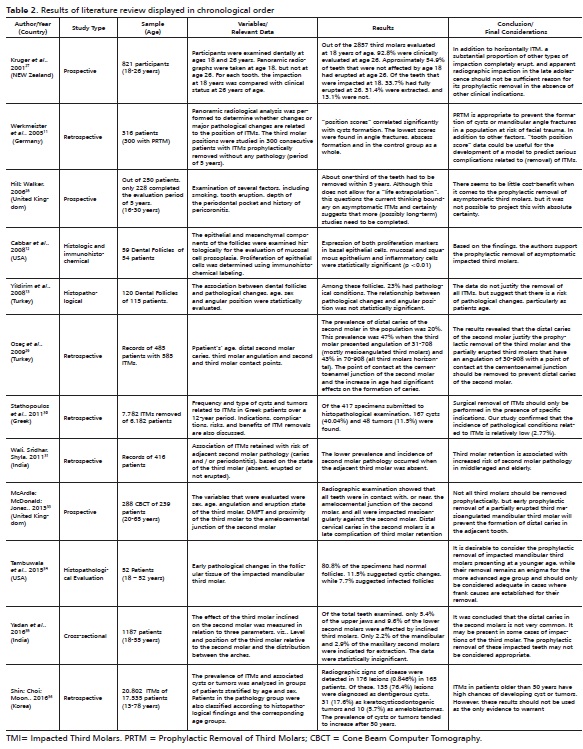
Table 2 presents the main findings of all the 13 selected articles that addressed the prophylactic removal of unerupted asymptomatic third molars and included the following parameters: authorship, year of publication, country of publication, type of study, sample size (and age), outcomes measured, relevant data and results, and study considerations.
Implications for Practice
In recent years, the shift in emphasis to nonintervention in patients with asymptomatic impacted third molars has been accompanied by a considerable debate.37 The supporters of prophylactic removal argue that the benefits outweigh the risks. Nonetheless, the scientific evidence is too inconclusive to support prophylactic removal. Unfortunately, most of the clinical research has failed, leading to contradictory interpretations that have not completely clarified the relative risks and benefits of early intervention.38
Conflicting reports persists surrounding to the incidence of pathological conditions associated with impacted third molars, and the subsequent need for prophylactic removal. The data remain limited regarding the long-term effects of unerupted third molars on adjacent teeth.32 According to Hicks,38 unreliable data would serve only to fuel this debate and the controversy over proper protocols.
It is likely that disagreements persists on which clinical recommendations should be followed when considering the prophylactic removal of asymptomatic third molars.39 Therefore, the decision to perform prophylactic removal of these teeth should be based on the probability of retained third molars causing future problems.30
Thus, the prophylactic removal of asymptomatic third molars requires individual care and case-by-case evaluation of each patient and the decision-making process regarding the retention versus prophylactic removal of these teeth should be based on the available scientific evidence combined with the professional's clinical experience.
Study Limitations
This literature review has some limitations given that the literature is lacking in randomized clinical trials regarding of the prophylactic removal of unerupted asymptomatic third molars. Other limitation found by the authors was the lacking in some full texts publications. However, available scientific evidence were included in order to better work on the subject. Sample sizes found in most studies were acceptable.
Discussion
Prophylactic removal of unerupted asymptomatic third molars is defined as a surgical procedure in which the patient does not present or has not presented any symptoms or pathologies associated with unerupted third molars.29 Currently, there is no general agreement as far as the necessity of surgical removal of asymptomatic third molars is concerned.
In order to minimize the risk of disease associated with these teeth30 or to avoid complications at more advanced ages, due to the risk of trauma or mandibular fractures,11,40 development of cysts and tumors,36 patient's recovery and prognosis,41 some authors believe that all unerupted third molars should be removed. Nevertheless, in this sense, there is still a need to compare the morbidity rates of tooth removal in people of several age groups.37
Occasionally, orthodontists propose the removal of asymptomatic third molars to complete orthodontic therapy.30Despite the fact that the role of third molars has been the subject of research, clinical interest, and debate for years, there is still a lack of scientific evidence from high-quality clinical studies on this subject.42 However, Normando et al.43 suggest that, in general, the best clinical conduct is not to proceed with the prophylactic extraction of third molars, except in situations where removal of a third molar is mandatory from the beginning of treatment.
The studies addressed in this literature review alluded to the potential for development of pathological alterations in unerupted asymptomatic third molars.11-13,27-36 Some evidence shows a greater risk in the occurrence of mandibular fractures11or associated lesions such as cysts,11,12 especially dentigerous ones,31,36 suggesting the prophylactic extraction of unerupted third asymptomatic molars might be a treatment option worth considering.
Other studies do not support such clinical conduct,17 considering that, even with the risk of occurrence of lesions13, which was relatively low,30 the relationship between pathological changes and dental position was not statistically significant, and that it was not possible to come up with a significant cost-benefit relationship.28
According to some authors,28,32 caries in the distal region of the second molar seem to be a factor that justifies the extraction of asymptomatic third molars, especially if the tooth is mesiongulated. 32 However, given that distal caries in the second molars is not very common in cases of third molar impactions, the prophylactic removal of these impacted teeth may not be considered appropriate.35
In this sense, in the absence of any other indication, the presence of radiologically diagnosable retention is not sufficient indication for the prophylactic removal of an asymptomatic third molar.27 This is specially true given the lack of evidence from randomized clinical trials that this procedure would avoid painful or infectious pathological complications due to its retention.25
Conclusion
There is some disagreement regarding the prophylactic extraction of unerupted asymptomatic third molars. Some authors justify the prophylactic removal based on the potential of development of pathological changes while other available scientific evidence does not support such conduct.
The routine removal of unerupted asymptomatic or disease- free third molars will require individual care and assessment. A case-by-case management protocol is needed. The close monitoring of these teeth may be an acceptable option.
The decision-making process regarding the retention versus prophylactic removal of unerupted asymptomatic third molars should be based on the available scientific evidences combined with the professional's clinical experience.
Acknowledgment
We thank Kevan Self from the Center for English as a Second Language at Southern Illinois University Carbondale for editing and proofreading this paper.
References
1. American Dental Association. 1999 survey of dental services rendered. ADA Catalog SDSR-1999. American Dental Association. 1999. [ Links ]
2. Friedman JW. The prophylactic extraction of third molars: a public health hazard. Am J Public Health. 2007;97(9):1554-9.
3. Song F, O'Meara S, Wilson P, Golder S, Kleijnen J. The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth. Health Technol Assess. 2000;4(15):1-55.
4. Torres MAF, Albiol JG, Aytés LB, Escoda CG. Evaluation of the indication for surgical extraction of third molars according to the oral surgeon and the primary care dentist. Experience in the Master of Oral Surgery and Implantology at Barcelona University Dental School. Med Oral Patol Oral Cir Bucal. 2008;13(8):E499-504.
5. American Association of Oral and Maxillofacial Surgeons (AAOMS). Statements by the AAOMS concerning the management of selected clinical conditions and associated clinical procedures: The management of impacted third molar teeth. American Association of Oral and Maxillofacial Surgeons, 2007.
6. Laskin DM. Evaluation of the third molar problem. J Am Dent Assoc. 1971;82(4):824-8.
7. Schulhof RJ. Third molars and orthodontic diagnosis. J Clin Orthod 1976;10:272-81.
8. Lysell L, Rohlin M. A study of indications used for removal of the mandibular third molar. Int J Oral Maxillofac Surg. 1988;17(3):161-4.
9. Stanley HR, Alattar M, Collett WK, Stringfellow HR Jr, Spiegel EH. Pathological sequelae of "neglected" impacted third molars. J Oral Pathol. 1988;17(3):113-7.
10. Al-Khateeb TL, El-Marsafi AI, Butler NP. The relationship between the indications for the surgical removal of impacted third molars and the incidence of alveolar osteitis. J Oral Maxillofac Surg. 1991;49(2):141-5.
11. Werkmeister R, Fillies T, Joos U, Smolka K. Relationship between lower wisdom tooth position and cyst development, deep abscess formation and mandibular angle fracture. J Craniomaxillofac Surg. 2005;33(3):164-8.
12. Cabbar F, Güler N, Comunoğlu N, Sençift K, Cöloğlu S. Determination of potential cellular proliferation in the odontogenic epithelia of the dental follicle of the asymptomatic impacted third molars. J Oral Maxillofac Surg. 2008;66(10):2004-11.
13. Yildirim G, Ataoğlu H, Mihmanli A, Kiziloğlu D, Avunduk MC. Pathologic changes in soft tissues associated with asymptomatic impacted third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(1):14- 8.
14. Costa MG, Pazzini CA, Pantuzo MC, Jorge ML, Marques LS. Is there justification for prophylactic extraction of third molars? A systematic review. Braz Oral Res. 2013;27(2):183-8.
15. Brokaw WC. The third molar question: when and why should we recommend removal?. Virginia Dental Journal; 1991;68(4):18-21.
16. Mercier P, Precious D. Risks and benefits of removal of impacted third molars. International Journal of Oral and Maxillofacial Surgery. 1992;21(1):17- 27.
17. Chuang SK, Perrott DH, Susarla SM, Dodson TB. Age as a risk factor for third molar surgery complications. Journal of Oral and Maxillofacial Surgery. 2007;65(9):1685-92.
18. Stavisky E. Clinical justification for the prophylactic removal of impacted third molars. Pennsylvania Dental Journal. 1989;56(3):8-9.
19. Tate TE. Impactions: observe or treat?. Journal of Californian Dental Association. 1994;22(6):59-64.
20. Baqain ZH, Karaky AA, Sawair F, Khraisat A, Duaibis R, Rajab LD. Frequency estimates and risk factors for postoperative morbidity after third molar removal: a prospective cohort study. J Oral Maxillofac Surg. 2008 Nov;66(11):2276-83.
21. Chuang Sk, Perrott DH, Susarla SM, Dodson TB. Risk Factors for Inflammatory Complications Following Third Molar Surgery in Adults. Journal of Oral and Maxillofacial Surgery. 2008;66(11):2213-8.
22. Brickley M, Kay E, Shepherd JP, Armstrong RA. Decision Analysis for lower-third-molar Surgery. Medical Decision Making. 1995;15(2):143-51.
23. Weyant R. No Evidence to Support Removal of Asymptomatic Impacted Third Molars in Adolescents or Adults. Journal of Evidence-Based Dental Practice. 2007;7(3):108-9.
24. Mettes TG, Nienhuijs ME, van der Sanden WJ, Verdonschot EH, Plass-chaert AJ. Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults. Cochrane Database Syst Rev. 2005;18:(2).
25. Mettes TG, Ghaeminia H, Nienhuijs ME, Perry J, van der Sanden WJ, Plass-chaert AJ. Surgical removal versus retention for the management of asymptomatic impacted wisdom teeth. Cochrane Database Syst Rev. 2012;13(6).
26. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLos Med. 2009;6(7):264-9.
27. Kruger E, Thomson WM, Konthasinghe P. Third molar outcomes from age 18 to 26: findings from a population-based New Zealand longitudinal study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(2):150-5.
28. Hill CM, Walker RV. Conservative, non-surgical management of patients presenting with impacted lower third molars: a 5-year study. Br J Oral Maxillofac Surg. 2006;44(5):347-50.
29. Ozeç I, Hergüner Siso S, Taşdemir U, Ezirganli S, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. Int J Oral Maxillofac Surg. 2009;38(12):1279-82.
30. Stathopoulos P, Mezitis M, Kappatos C, Titsinides S, Stylogianni E. Cysts and tumors associated with impacted third molars: is prophylactic removal justified? J Oral Maxillofac Surg. 2011;69(2):405-8.
31. Wali GG, Sridhar V, Shyla HN. A study on dentigerous cystic changes with radiographically normal impacted mandibular third molars. J Maxillofac Oral Surg. 2012;11(4):458-65.
32. Nunn ME, Fish MD, Garcia RI, Kaye EK, Figueroa R, Gohel A, et al. Retained asymptomatic third molars and risk for second molar pathology. J Dent Res. 2013;92(12):1095-9.
33. Mcardle LW, Mcdonald F, Jones J. Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of third molar teeth? Update. Br J Oral Maxillofac Surg. 2014;52(2):185-9.
34. Tambuwala AA, Oswal RG, Desale RS, Oswal NP, Mall PE, Sayed AR, et al. An evaluation of pathologic changes in the follicle of impacted mandibular third molars. J Int Oral Health. 2015;7(4):58-62.
35. Yadav P, Pruthi PJ, Nawal RR, Talwar S, Verma M. Saving the 2nd Molar from the 3rd Is it Really the Guilt of the Tilt? Journal of Clinical and Diagnostic Research. 2016;10(5).
36. Shin SM, Choi EJ, Moon S-Y. Prevalence of pathologies related to impacted mandibular third molars. SpringerPlus. 2016;5(1):915.
37. Hill CM, Walker RV. Conservative, non-surgical management of patients presenting with impacted lower third molars: a 5-year study. Br J Oral Maxillofac Surg. 2006;44(5):347-50.
38. Hicks EP. Third molar management: a case against routine removal in adolescent and young adult orthodontic patients. J Oral Maxillofac Surg. 1999;57(7):831-6.
39. Godfrey K. Prophylactic removal of asymptomatic third molars: a review. Aust Dent J. 1999;44(4):233-7.
40. Duarte BG, Assis D, Ribeiro-Júnior P, Gonçales ES. Does the Relationship between Retained Mandibular Third Molar and Mandibular Angle Fracture Exist? An Assessment of Three Possible Causes. Craniomaxillofacial Trauma & Reconstruction. 2012;5(3):127-36.
41. Zhang QB, Zhang ZQ. Early extraction: a silver bullet to avoid nerve injury in lower third molar removal? Int J Oral Maxillofac Surg 2012;18;41(10):1280-3.
42. Almpani K, Kolokitha O-E. Role of third molars in orthodontics. World Journal of Clinical Cases. 2015;3(2):132-40.
43. Normando D. Third molars: To extract or not to extract? Dental Press Journal of Orthodontics. 2015;20(4):17-8.
 Endereço para correspondência:
Endereço para correspondência:
Marlus da Silva Pedrosa
e-mail: marluspedrosa@gmail.com
Recebido: 01/26/2017
Aceito: 03/06/2017
