










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRPG. Revista de Pós-Graduação
versão impressa ISSN 0104-5695
RPG, Rev. pós-grad. vol.18 no.1 São Paulo Jan./Mar. 2011
Efficacy of antimicrobial sprays for disinfection of children's toothbrushes – a randomized clinical trial
Eficácia de sprays antimicrobianos para desinfecção de escovas dentais de crianças – estudo clínico randomizado
Soraia MacariI; Izabel YokoII; Raquel Assed Bezerra da SilvaIII; Léa Assed Bezerra da SilvaIII; Francisco Wanderley Garcia de Paula-SilvaIV; Paulo Nelson-FilhoIII
IMSc Student from Department of Pediatric Clinics, Preventive and Social Dentistry, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto/SP, Brazil
IIPhD, Professor from Department of Clinical Analysis, Toxicology and Bromatology, School of Pharmaceutical Science of Ribeirão Preto, University of São Paulo, Ribeirão Preto/SP, Brazil
IIIPhD, Professor from Pediatric Clinics, Preventive and Social Dentistry, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto/SP, Brazil
IVPhD, Pedodontist, from Department of Pediatric Clinics, Preventive and Social Dentistry, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto/SP, Brazil
ABSTRACT
The objective of this study was to evaluate the efficacy of three spray antimicrobial solutions for the disinfection of children's toothbrushes. A 4-stage changeover system was used. The solutions studied were: BrushtoxTM (Spray 1), CosmocilTM + basic formula (Spray 2), basic formula (Spray 3), and control – sterile water (Spray 4). Forty children used the solutions in all stages. In each stage, the children received a new toothbrush and performed a single 1-min brushing. Thereafter, the solutions were sprayed six times at different positions on the toothbrush bristles. After four hours, microbiologic culture of the toothbrushes was performed. BrushtoxTM, CosmocilTM + basic formula, and basic formula presented a similar effect on prevention of cariogenic biofilm formation which was better than basic formula alone or sterile water. BrushtoxTM showed the best antimicrobial efficacy.
Descriptors: Disinfection. Dental devices, home care. Child. Biofilms.
RESUMO
O objetivo deste estudo foi avaliar a eficácia de três soluções antimicrobianas na forma de spray para a desinfecção de escovas dentais de crianças. As soluções estudadas foram: BrushtoxTM (Spray 1), CosmocilTM + fórmula básica (Spray 2), fórmula básica (Spray 3) e controle – água esterilizada (Spray 4). As soluções foram utilizadas em todas as fases por 40 crianças. Em cada fase, as crianças receberam uma nova escova de dentes e realizaram uma única escovação de um minuto. Em seguida, as soluções foram pulverizadas seis vezes, em diferentes posições, sobre as cerdas das escovas. Após quatro horas, foi realizada a cultura microbiológicas das escovas dentais. BrushtoxTM, CosmocilTM + fórmula básica e fórmula básica isoladamente apresentaram um efeito semelhante sobre a prevenção da formação de biofilme cariogênico, que foi melhor do que a água esterilizada. O BrushtoxTM mostrou a melhor eficácia antimicrobiana.
Descritores: Desinfecção. Dispositivos para o cuidado bucal domiciliar. Criança. Biofilmes.
INTRODUCTION
Toothbrushes harbor a high number of bacteria immediately after brushing2,6,21, including Streptococcus mutans8,10,17,18,20,23,24. Retention and survival of cariogenic microorganisms on toothbrushes represent a possible cause of recontamination of the mouth24.
Daily use of contaminated toothbrushes can contribute to disseminate microorganisms within the oral cavity of an individual or between different family members7,23. Occasionally, toothbrushes belonging to different members of the same family may contact directly themselves when stored in the holder or when stored together in bathroom drawers or cabinets19. In addition, toothbrush contact is unlikely controlled in day-care centers, kindergartens, and other institutions that shelter children at an early age, where toothbrushes can be inadvertently exchanged or shared12.
Antimicrobial solutions can be used for toothbrush disinfection, among them are chlorhexidine gluconate14,18, cetylpyridinium chloride4,13, triclosan and essential oils4. Similarly to chlorhexidine, CosmocilTM, also from biguanide group, is a broad-spectrum biocide acting against gram-positive and gram-negative bacteria, yeast, and fungi. This fast acting biocide is used for the preservation of personal-care products against microbial spoilage by the pharmaceutical industry in products such as pre-moistened wipes, contact lens solutions, band-aidTM, and experimentally for toothbrush disinfection18.
BrushtoxTM Antiseptic Toothbrush Cleanser (Dentox Limited, Warwick, England) is another disinfectant solution that was developed for toothbrush disinfection. Its formula is based on an activated ethanol solution (35–40%), associated with 4.5% biocides and a mixture of para-hydroxybenzoate. According to the manufacturer, BrushtoxTM spray is highly effective against a wide range of bacteria, fungi and virus, using both in vivo and simulated "usage" tests3,11,16,18.
OBJECTIVES
The aim of this study was to evaluate the efficacy of three spray antimicrobial solutions for the disinfection of children's toothbrushes, by microbial culture and cariogenic biofilm formation.
MATERIAL AND METHODS
Forty female children from a day-care center (aged 5–12 years) participated in this study after approval by the Ethics Committee of the School of Dentistry of Ribeirão Preto (SP, Brazil) (Process nº 2001.1.920.58.7). Written consent was obtained from the parents or guardians of the children. The children were not using antibiotics or antiseptics and did not have been submitted to dental treatment for at least three months.
One week prior to study commencement, the children received lectures about toothbrushing techniques and were motivated about the importance of oral health. At the end of the study, a lecture about dental caries prevention was given and each child received a new toothbrush and toothpaste.
A 4-stage changeover system was used with an interval of three to four days between each stage. Forty children were randomly assigned into four groups of ten children each (1, 2, 3, and 4). In each stage, the children received a new toothbrush (Magic Grip REACHTM, Johnson & Johnson, São José dos Campos, SP, Brazil). The fluoride toothpaste SorrisoTM (Kolynos do Brasil Ltda., São Bernardo do Campo, SP, Brazil) was applied to the toothbrush bristles by the transverse technique. The children made a single 1-min brushing and rinsed the toothbrush with tap water. After the children have rinsed the toothbrushes, a single professional removed the excess water from the bristles.
Subsequently, the following toothbrush solutions, supervised by the professional, were used: BrushtoxTM(Dentox Ltda., Warwick, England) – Spray 1;basic formula plus 1% CosmocilTM (Laboratory of Pharmacotechnical, School of Pharmaceutical Science of Ribeirão Preto, University of São Paulo, Ribeirão Preto/SP, Brazil) – Spray 2; basic formula (30% propylene glycol; 0.16% methylparaben; 0.02% propylparaben; 0.02% polyvinylpyrrolidone K30; 10 mL ethanol 96º GL; 100 mL distilled water) – Spray 3; sterile water (Control Group) – Spray 4.
The toothbrushes were held in a vertical position and, at 5 cm from the toothbrush, Sprays 1, 2, 3, or 4 were sprayed 6 times (approximately 0.6 mL of solution for each toothbrush) in different positions on the bristles: (1) right side, (2) left side, (3) above, (4) below, (5) in front of, and (6) behind the toothbrush head. Excess antimicrobial solution was removed from the bristles by gently hitting the toothbrush against the sink.
All solutions were used in each stage decreasing the possibility of variables that could interfere with the results of disinfectant solutions.
The toothbrushes were fixed vertically in a closed container and transported to the Laboratory of Microbiology where they remained for four hours at room temperature to simulate interval between toothbrushing. As an additional control, two unused toothbrushes were removed from their packages and were inserted in microbiologic culture media.
After four hours, all toothbrushes were introduced vertically (avoiding contact of the bristles with the test tube wall) into separate 25 x 150 mm test tubes, containing 10 mL CaSaB medium (Bacitracin Sucrose Broth), which is a selective enrichment broth prepared by the modification of Jensen and Bratthall9 and a medium specific for mutans streptococci (MS) without trypan blue5. They were incubated for three to four days at 37ºC. The toothbrushes were withdrawn and shaken gently to remove planktonic microbiota, leaving sessile bacteria adhered as "spike" or "mushroom-like" biofilm/colony. The toothbrush bristles were analyzed carefully from all sides and angles, and each sessile biofilm/colony, based on the colony morphology, was counted under aseptic conditions with a stereoscopic microscope (Nikon, Japan) and reflected light.
The toothbrushes without colony/biofilm developed on the bristles were kept in the medium broth and incubated for an additional 20 days to verify possible medium clouding. Recovery or confirmation of MS was assessed by transferring some biofilm/colonies from the bristles to tubes containing 2.0 mL phosphate buffered saline (PBS). The tubes were vortexed for 2 min and the solution was seeded on SB20 agar22.
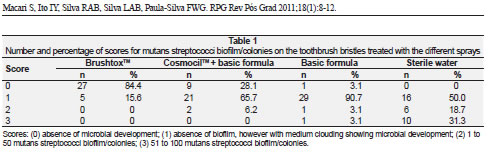
The results were expressed as scores: (0) absence of microbial development and absence of medium clouding; (1) absence of biofilm, however with medium clouding, showing microbial development; (2) 1 to 50 MS biofilm/colonies; (3) 51 to 100 MS biofilm/colonies. Friedman's test and Dunn's post-test were used to analyze cariogenic biofilm formation; Cochran's testand Wilcoxon's test were used to analyze antimicrobial efficacy of the solutions (α = 5%).
RESULTS
In total, 32 out of 40 children participated in all stages of this study. The number and percentage of MS biofilm/colonies on the bristles of the toothbrushes treated with the different sprays is shown in Tabela 1.
BrushtoxTM (Spray 1) inhibited microbial development in 27 cases (84.4%). Only 15.6% of the cases (n = 5) showed this development related to medium clouding, yet no biofilm formation was evident. Basic formula + CosmocilTM (Spray 2) inhibited microbial development in 9 cases (28.1%). When microbial development was observed, 65.7% were related to medium clouding and 6.2% to biofilm formation. Basic formula (Spray 3) did not inhibited microbial development, with 96.9% of the cases presenting microbial development, with medium clouding in 90.7% (n = 29) and biofilm formation in 6.2% (n = 2) of the cases. Following sterile water use (Spray 4), microbial development occurred in 100% (n = 32) of the cases, showed by medium clouding (50%) or by biofilm formation (50%). BrushtoxTM, basic formula + CosmocilTM and basic formula alone presented similar prevention of cariogenic biofilm formation, which was higher than sterile water (p < 0.01). BrushtoxTM showed higher antimicrobial efficacy followed by basic formula + CosmocilTM and basic formula alone, while sterile water showed low antimicrobial activity.
Transferring colonies from the toothbrush bristles seeded on SB20 agar resulted in MS biofilm/colonies. This indicated that the biofilm/colonies on the bristles were formed by MS. Incubating unused toothbrushes resulted in negative culture.
DISCUSSION
The present study is in agreement with previous investigations reporting toothbrush contamination by MS1,15,17,18,21,24, even after four hours of dry period, corroborating previous findings that MS remains viable on toothbrushes bristles until eight hours22.
Although disinfection of toothbrushes was done by immersion in different antimicrobial solutions in other studies4,17,25, in this study disinfection was achieved by spray according to the method of Meier et al.13. Spray solutions are economic, fast, easy, and practical for toothbrush disinfection, being also easily transported during travel.
An experimental CosmocilTM-based solution was evaluated by Nelson-Filho et al.18for disinfection after contamination of toothbrushes used by 24- to 48-month-old children. In the in vivo trial, children were randomly assigned to 4 groups and a 4-stage changeover system was used with a 1-week interval between each stage. Children were submitted to a 1-minute brushing (without toothpaste) performed by a single professional, followed by random spraying of the test solutions and microbiological analysis. The experimental solution reduced/prevented the formation of MS colonies/biofilms on the toothbrush bristles when compared to the sterile water (control). Although they verified in vitro that this antimicrobial solution was effective, there were no in vivo studies that evaluate CosmocilTM as a toothbrush disinfectant. Similarly, the present study demonstrated that CosmocilTM-based solution showed efficacy on the inhibition of the bacterial development on toothbrush bristles. We also showed that this inhibition was superior when compared to basic formula alone but less effective when compared to BrushtoxTM.
BrushtoxTM is an antiseptic toothbrush cleanser developed to kill most bacteria, fungi and virus that contaminate toothbrushes3,11. This in vivo study corroborated an in vitro study by Neal and Rippin16 reporting that BrushtoxTM is an effective disinfectant agent for bacteria and fungi on toothbrushes. Although there was no difference among Sprays 1, 2 and 3 in relation to the cariogenic biofilm formation, Spray 1 was the most effective antimicrobial solution for toothbrush disinfection. We are also in agreement with Nelson-Filho et al.18 which showed that this solution is effective against the bacterial contamination on the toothbrushes bristles.
According to current biological security concepts, health professionals are responsible to divulge and to practice infection control for their own and their patients' protection. Because the toothbrush is a personal instrument, each toilet should have its own antimicrobial spray bottle for toothbrush disinfection so that the toothbrush, mainly an instrument for the maintenance of oral health, would be a promoter of health and not a source of infection.
Other studies are necessary to find a formula that would be more efficient, more economical, easier to apply, and thus more assessable to the population. Meanwhile, toothbrush disinfection should be started and taught by health professionals, mainly by the dentist, making toothbrush disinfection a daily habit.
CONCLUSION
BrushtoxTM was effective for cariogenic biofilm inhibition and the basic formula and CosmocilTM + basic formula were effective for decreasing cariogenic biofilm formation. BrushtoxTM was the best antimicrobial solution for children's toothbrush disinfection. Antimicrobial sprays seem to be a practical, fast, easy and economical method for toothbrush disinfection. Health professionals, mainly dentists, should recommend toothbrush disinfection as a routine daily habit to control infection.
ACKNOWLEDGMENTS
This study was supported by fellowship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) to Soraia Macari.
REFERENCES
1. Ayşegül O, Elgin IE, Gulcin A, Nedim S. The efficacy of chlorhexidine spray vs mouthwash in the microbial contamination of child toothbrushes. J Dent Child (Chic) 2007;74(3):177-81. [ Links ]
2. Bunetel L, Tricot-Doleux S, Agnani G, Bonnaure-Mallet M. In vitro evaluation of the retention of three species of pathogenic microorganisms by three different types of toothbrush. Oral Microbiol Immunol 2000;15(5):313-6. [ Links ]
3. Carter JN, Paterson KMA. Brushtox®: evaluation of disinfectant efficacy [clinical note]. Warwick: Research Laboratory; 1998. p.6-18. [ Links ]
4. Caudry SD, Klitorinos A, Chan ECS. Contaminated toothbrushes and their disinfection. J Can Dent Assoc 1995;61(6):511-6. [ Links ]
5. Cesco RT, Bignelli P, Santos CP, Ito IY. Toothbrushes: evaluation of contamination level by streptococci of mutans group. In: World Congress on Preventive Dentistry, 5th, 1995, São Paulo. Proceedings. São Paulo/SP, Brazil, 1995. p. 103. [ Links ]
6. Efstratiou M, Papaioannou W, Nakou M, Ktenas E, Vrotsos IA, Pani V. Contamination of a toothbrush with antibacterial properties by oral microorganisms. J Dent 2007;35(4):331-7. [ Links ]
7. Glass RT, Jensen HG. More on the contaminated toothbrush: the viral story. Quintessence Int 1988;19(10):713-6. [ Links ]
8. Goldsmith RN, Shey Z, Houpt MI, Fine D, Schreiner H, Greenberg B. Toothbrush bristle wear and adherence of Streptococcus mutans. Pediatr Dent 2007;29(3):243-7. [ Links ]
9. Jensen B, Bratthall DA. A new method for the estimation of mutans estreptococci in human saliva. J Dent Res 1989;68(3):468-71. [ Links ]
10. Kozai K, Iwai T, Miura K. Residual contamination of toothbrushes by microorganisms. ASDC J Dent Child 1989;56(3):201-4. [ Links ]
11. Kurtz JB. Suspension biocide test against Echovirus 11 (Picornaviridae family) [clinical note]. Warwick: Oxford Radcliffe Hospital; 1998. [ Links ]
12. Malmberg E, Birkhed D, Norvenius G, Norén JG, Dahlén G. Microorganisms on toothbrushes at day-care centers. Acta Odont Scand 1994;52(2):93-8. [ Links ]
13. Meier S, Collier C, Scalleta MG, Stephens J, Kimbrough R, Kettering JD. An in vitro investigation of the efficacy of CPC for use in toothbrushes decontamination. J Dent Hyg 1996;70(4):161-5. [ Links ]
14. Mehta A, Sequeira PS, Bhat G. Bacterial contamination and decontamination of toothbrushes after use. NY State Dent J 2007;73(3):20-2. [ Links ]
15. Motzfeld R, Huerta J, Apip A, Araya E. Tipo y grado de contaminación por bacterias bucales y levaduras de cepillos dentales con uso habitual. Rev Facul Odont Univ Chile 1999;17(1):9-14. [ Links ]
16. Neal PR, Rippin JW. The efficacy of a toothbrush disinfectant spray – an in vitro study. J Dent 2003;31(2):153-7.
17. Nelson Filho P, Macari S, Faria G, Assed S, Ito IY. Microbial contamination of toothbrushes and their decontamination. Pediatr Dent 2000;22(5):381-4. [ Links ]
18. Nelson-Filho P, Faria G, da Silva RA, Rossi MA, Ito IY. Evaluation of the contamination and disinfection methods of toothbrushes used by 24- to 48-month-old children. J Dent Child (Chic) 2006;73(3):152-8. [ Links ]
19. Newbrun E. Preventing dental caries: current and prospective strategies. J Am Dent Assoc 1992;123(5):68-73. [ Links ]
20. Quirynen M, De Soete M, Pauwels M, Gizani S, Van Meerbeek B, van Steenberghe D. Can toothpaste or a toothbrush with antibacterial tufts prevent toothbrush contamination? J Periodontol 2003;74(3):312-22. [ Links ]
21. Saravia ME, Nelson-Filho P, da Silva RA, Faria G, Rossi MA, Ito IY. Viability of Streptococcus mutans toothbrush bristles. J Dent Child (Chic) 2008;75(1):29-32. [ Links ]
22. Saravia ME, Nelson-Filho P, Ito IY, Silva LAB, Silva RAB, Emilson CG. Morphological differentiation between S. mutans and S. sobrinus on modified SB-20 culture medium. Microbiol Res 2011;166(1):63-7. [ Links ]
23. Svanberg M. Contamination of toothpaste and toothbrush by Streptococcus mutans. Scand J Dent Res 1978;86(5):412-41. [ Links ]
24. Wetzel WE, Schaumburg C, Ansari F, Kroeger T, Sziegoleit A. Microbial contamination of toothbrushes with different principles of filament anchoring. J Am Dent Assoc 2005;136(6):758-65. [ Links ]
25. Whitley R, Gilmore E. Contaminated toothbrushes and their disinfection. J Dent Res 1973;52 Suppl 1:218. [ Links ]
 Correspondence to:
Correspondence to:
Prof. Dr. Paulo Nelson Filho
Department of Pediatric Clinics, Preventive and Social Dentistry. School of Dentistry of Ribeirao Preto, University of Sao Paulo
Avenida do Café w/o nº
CEP 14040-904 – Ribeirão Preto/SP, Brazil
Phone: (55) 16 3602-4099
e-mail: nelson@forp.usp.br
Received in: 11/2/11
Accepted in: 27/3/11
