










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRPG. Revista de Pós-Graduação
versão impressa ISSN 0104-5695
RPG, Rev. pós-grad. vol.18 no.1 São Paulo Jan./Mar. 2011
ORIGINAL ARTICLE
Long-term success of immediately restored single implant-supported prosthesis in reconstructed cleft maxilla
Sucesso em longo prazo de próteses unitárias implanto-suportadas imediatamente restauradas em maxilas fissuradas reconstruídas
Priscila GarciaI; Maria Lúcia Rubo de RezendeII; Flávio Monteiro AmadoIII; Samira SalmeronIV; Adriana Campos Passanezi Sant'anaII; Sebastião Luiz Aguiar GreghiII; Euloir PassaneziV
IDoctor of Dental Surgery; Private practitioner – São Paulo/SP, Brazil
IIDoctor of Dental Surgery; PhD Professor from Department of Periodontology, School of Dentistry of Bauru, University of São Paulo – Bauru/SP, Brazil
IIIDoctor of Dental Surgery; PhD Professor from Department of Implantology of the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo – Bauru/SP, Brazil
IVDoctor of Dental Surgery; Post-graduation student from Department of Periodontology, School of Dentistry of Bauru, University of São Paulo – Bauru/SP, Brazil
VDoctor of Dental Surgery; PhD Professor and Head from Department of Periodontology, School of Dentistry of Bauru, University of São Paulo – Bauru/SP, Brazil
ABSTRACT
The purposes of this study were to evaluate the rate of success of immediate or early loaded implants placed in congenital cleft alveolus in a reference Brazilian Public Service, and to investigate the probable causes of failures. All the immediately restored osseointegrated implants installed from 1991 to 2010 at the Hospital for Rehabilitation of Craniofacial Anomalies (Bauru, SP, Brazil) were investigated. This search resulted in 281 patients, in whom 573 implants were installed. Only 10 fulfilled the following criteria: 1) single implants installed at the cleft alveolus (grafted or not) at least two years before the beginning of the study; 2) implants that had undergone to immediate or early load. Data about the patients and implants were collected from records of the patients and presented as percentage of well succeeded and failed implants. None of the implants failed. The implants have been in function for at least 58 months. Nine implants are in function for at least 5 years and one, for at least 10 years. It was concluded that rough surfaced titanium implants with proper dimensions installed in low density bone at the cleft region can receive immediate non functional provisional restoration with satisfactory prognosis at medium and long-term as long as strict criteria is followed for case selection.
Descriptors: Dental implantation. Cleft palate. Dental prosthesis.
RESUMO
Os objetivos deste estudo foram avaliar a taxa de sucesso de implantes imediatamente ou precocemente instalados em fissura alveolar congenital em um Serviço Público de Referência brasileiro e investigar as prováveis causas de fracassos. Todos os implantes osseointegrados imediatamente restaurados, instalados entre 1991 e 2010, no Hospital de Reabilitação de Anomalias Craniofaciais (Bauru, SP, Brazil), foram investigados. Esta busca resultou em 281 pacientes, nos quais 573 implantes foram instalados. Apenas 10 preencheram os seguintes critérios: 1) implantes unitários instalados na área de fissura alveolar (enxertada ou não) pelo menos dois anos antes do início deste estudo; 2) implantes que foram submetidos à carga precoce ou imediata. Os dados dos pacientes e dos implantes foram coletados dos prontuários e apresentados como porcentagem de implantes bem-sucedidos ou fracassados. Nenhum dos implantes fracassou. Os implantes estiveram em função por pelo menos 58 meses, sendo que 9 deles estão em função por pelo menos 5 anos e um, por pelo menos 10 anos. Concluiu-se que implantes de titânio de superfície rugosa com dimensões adequadas instalados em osso de baixa densidade na região da fissura alveolar podem receber provisionalização imediata não funcional com prognóstico favorável a médio e longo prazo desde que sejam seguidos rigorosos critérios para a seleção dos casos.
Descritores: Implantes dentários. Fissura palatina. Prótese dental.
INTRODUCTION
The success of the treatment in cleft palate patients is dependant of the efforts of a team of specialists including plastic surgeon, speech therapist, orthodontist, prosthodontist, among others. Orthodontics takes active part in the multidisciplinary process of the cleft rehabilitation associated or not to alveolar bone grafts aiming at a non-prosthetic result4,17. Nevertheless, when the orthodontic treatment ends with an edentulous space at the cleft region, osseointegrated implants installation may be the election procedure16,18 once they have widened the clinical perspectives and favored the esthetical outcomes10,16,17,21.
Implant-supported restoration in cleft alveolus was first published by Verdi et al.26 who presented a satisfactory result with the placement of a single implant at the cleft region 18 months after autogenous bone grafting. Since then, several studies have attested the high predictability of the procedure7,10,13,15,16,19,22,23,25. On the other hand, in a recent investigation about failures and complication in patients with birth defects restored with single crowns on teeth and/or implants, Krieger et al.18 found that up to five years of function, despite of the low incidences of failures, a considerable percentage of the patients experienced at least one biological and/or a technical complication.
Implants installed in two-stage procedure ad modum Brånemark et al.5 have high rates of success and are considered reference for researchers1. According to traditional literature, a submersion period without loading of six months for the maxilla and three to four months for the mandible is necessary for osseointegration to occur5,6. Nevertheless, results of reliable studies have attested the feasibility of the immediate load on implants in well controlled conditions: good oral hygiene, enough bone quality and quantity, biomechanicaly proper surgical and prosthetic procedures, fitness of a fixed prosthetic suprastructure, patient selection, rigid connection among the implants and maintenance of the splinted condition until four months after implants installation9.
Many authors have reported efficiency and predictability of immediate loaded implants in non-cleft maxillas3,8,12,14,24. Due to the high expectations of the patients for functionality and esthetics of the prosthetic rehabilitation, long-term information on tangible outcomes is needed11. However, there is scarce or nonexistent information about the long-term success of immediate or early loaded implant-supported prosthesis placed in cleft maxilla.
OBJECTIVES
This investigation aimed at surveying the success rate of immediately restored implants placed in cleft patients at the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo, in Bauru, Brazil, as well as to investigate the causes of eventual failures.
MATERIAL AND METHODS
This study was approved by the Ethical Committee of the Hospital for Rehabilitation of Craniofacial Anomalies (HRAC), University of São Paulo, Bauru, Brazil. The medical records of the patients who underwent to osseointegrated implants therapy between 1991 and 2010 at the HRAC were evaluated and analyzed retrospectively. This search resulted in 281 patients, in whom 573 implants were installed. Only ten implants installed in nine patients fulfilled the rigid inclusion criteria established for this study: 1) single implants installed at the grafted cleft alveolus at least two years before the beginning of the study; 2) implants that had received immediate or early load. The exclusion criteria were: syndromic patients, handicapped individuals unable to realize oral hygiene, patients with systemic diseases that interfere on tissue repair, immunologically depressed patients or those who were taking drugs with the same effect. Files, photographs and radiographs of the patients were used to classify the implants as well succeeded or failed, according to the criteria of success proposed by Albrektsson et al.2
RESULTS
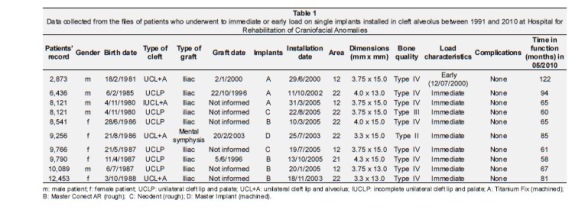
Very few patients fulfilled the inclusion criteria, in part due to the high incidence of systemic diseases and genetic syndromes among the cleft patients attended at HRAC. General information about the patients (age, gender, type of cleft, bone quality and habits) and concerning the implants (surface characteristics, grafting data, prosthetic restoration and time elapsed in function) obtained from files of the patients are seen at Tabela 1. They were 4 male and 5 female patients with average age of 18 years and 5 months (ranging from 15 years and 1 month to 24 years and 4 months) at the moment of the implant installation. The implants have been in function, osseointegrated and without signs of failure or significant radiographic bone loss for the mean time of 75.8 ± 20.2 months (6 years approximately), varying from 58 months (4 years and 10 months) to 122 months (10 years and 2 months).
Only one implant presented machined surface (Master Implant, Conexão Sistemas de Prótese, São Paulo, Brazil) and all the others had either sand blasted/acid etched surfaces (Titanium Fix, AS Technology, Sao Jose dos Campos, SP, Brazil) or acid etched surfaces (Master Conect AR, Conexão Sistemas de Prótese, São Paulo, Brazil and Neodent, Curitiba, PR, Brazil). The smallest implant measured 3.3 x 13.0 mm (1 implant) and the biggest one measured 4.0 x 15.0 mm (1 implant). Most of them measured 3.75 x 15.0 mm (4 implants).
The photographs and records on the files of the patients allowed us to verify that none of the 10 studied implants received true immediate load as classified by Misch et al.20. According to this classification, one of the implants received early non functional restoration 13 days after its insertion. All the other 9 implants received immediate nonfunctional restoration. Eight implants (80%) were installed in type IV bone; 1 (10%) was inserted in type III iliac bone transplanted to the cleft area; and 1 implant (10%) was inserted in type II bone harvested from de mental symphysis and grafted to the cleft area. The bone type was detected at the moment of the surgery and registered on the patients' files.
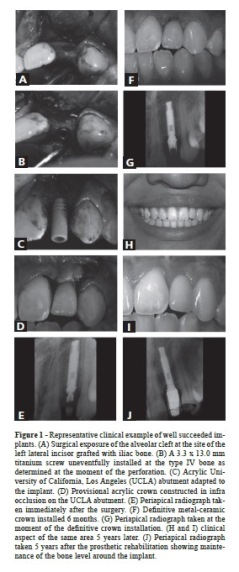
A representative clinical example of the well succeeded implants is shown in Figure 1. The patient was a 15-year-old girl whose incomplete unilateral left cleft was grafted with iliac bone at an unknown data about three years before (according to the patients' mother). A titanium screw – 3.3 x 13.0 mm – (Master Porous, Conexão Sistemas de Prótese, São Paulo, Brazil) was inserted at the partially resorbed type IV bone site of the left lateral incisor and immediately restored with an acrylic provisional crown constructed in infra occlusion on an acrylic UCLA abutment. Six months later, a screwed metal-ceramic crown was installed. Radiographs taken at the day of implant installation, six months, and five years later show little bone loss around the implant and until the moment this manuscript was concluded (six years and six months after the implant installation) there were no clinical signs and symptoms of failure or lack of osseointegration.
DISCUSSION
This study has demonstrated medium and long-term success in ten single immediately restored implants installed at cleft alveolus. This result is in accordance to many reports from two stage implants placed non cleft and non grafted areas3,8,12,14,24. Even though Krieger et al.18 have found that, up to five years in function, a considerable percentage of patients with birth defects restored with single crowns on teeth and/or implants experiences at least one biological and/or a technical complication, this could not be observed in our study.
High rates of long-term success have been reported for implants placed in grafted cleft alveolus7,10,13,15,19,22,23,25 and the length of the implants is proven to be related to survival rate25. Nevertheless, Kramer et al.17 have observed that implant survival was less in cleft lip and palate patients when compared to a non-cleft control group, but improved when compared to patients with bone grafting for other indications. It has also been stated that bone quality can be crucial for the survival rate of the implants25 and, when cleft alveolus are grafted with type IV iliac bone, a period of no less than six months is recommended for uncovering the implants16.
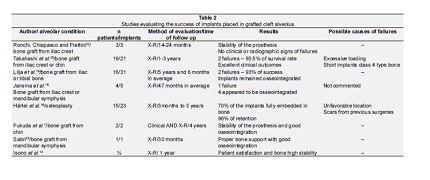
Some representative studies evaluating the outcomes of congenital clefts rehabilitation can be seen at Tabela 2. It can be noticed that even though the samples are relatively small, there is certain homogeneity of procedures and methods of evaluation which makes possible the comparison among them. The implants were generally placed at cleft alveolus grafted with bone from iliac crest, mandible or tibia. All the studies related good results and high rates of success. Nevertheless, none of them dealt with immediately restored implants. In this study the percentage of success was as high as those found for two stage implants.
A more specific analysis from the data evidenced that even though the majority of the implants (9; 90%) have been inserted in low quality bone (types III and IV) and restored with non splinted single crowns, they succeeded, counteracting two of the established and widely accepted criteria for immediate load: high density bone and rigid connection among multiple implants6. Nevertheless, it must be emphasized that other relevant aspect was considered and respected when indicating of each of the immediate restorations carried out, i.e., implants presenting proper dimensions (from 13 mm to 15 mm in length). In a series of cases, Takahashi et al.25 showed that although two implants were lost, bone grafted alveoli were suitable for the placement of endosseous implants. The failures were attributed to the length of the implants (both 7 mm long), bone quality (class IV type bone), location and loading (canine region). Those authors stated that implants placed in bone grafted alveoli should have a length of at least 10 mm, and that a length of more than 13 mm is recommended in class IV type bone. In our study, when implants of reduced diameter were employed (3.3 mm), their lengths (13 mm and 15 mm) or the bone quality at the area of their insertion (type II) compensated this disadvantage (Tabela 1).
CONCLUSIONS
Based on the collected data and within the limits imposed by the sample size, it was concluded that even when installed in low density bone, rough surfaced osseointegrated implants of proper dimensions can be provisionally restored under non functional load at the moment of its insertion with satisfactory prognosis at medium and long-term. This statement is supported by the high rate of success compatible with existent data from literature for two stage implants placed at areas presenting appropriate bone quantity and quality. It must be emphasized that adequate implant dimensions, minimally traumatic surgical technique, as well as absence of direct occlusal contacts on the implant-supported restoration may represent the principles the indication for this procedure is based on.
ACKNOWLEDGMENTS
This study was supported by the Foundation for Support of Research of the State of São Paulo (FAPESP), Grant nº 2007/06659-3.
REFERENCES
1. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10(6):387-416. [ Links ]
2. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants:a review and proposed criteria of success. Int J Oral Maxillofac Implants 1986;1(1):11-25. [ Links ]
3. Balshi JT, Wolfinger JG. Immediate loading of Brånemark implants in edentulous mandibles: a preliminary report. Implant Dent 1997;6(2):83-8. [ Links ]
4. Bergland O, Semb G, Abyholm F, Borchgrevink H, Eskeland G. Secondary bone grafting and orthodontic treatment in patients with bilateral complete clefts of the lip and palate. Ann Plast Surg 1986;17(6):460-74. [ Links ]
5. Brånemark PI, Hansson BO, Adell T, Breine U, Lindström J, Hallén O, et al. Osseointegrated implants in the treatment of edentulous jaw: experience from a 10 year period. Scand J Plast Reconstr Surg 1977;16(Suppl):1-132. [ Links ]
6. Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent 1983;50(3):399-410. [ Links ]
7. Fukuda M, Takahashi T, Yamaguchi T, Kochi S, Inai T, Watanabe M, et al. Dental rehabilitation using endosseous implants and orthognathic surgery in patients with cleft lip and palate: report of two cases. J Oral Rehabil 2000;27(6):546-51. [ Links ]
8. Ganeles J, Rosenberg MM, Holt RL, Reichman LH. Immediate loading of implants with fixed restorations in the completely edentulous mandible: report of 27 patients from a private practice. Int J Oral Maxillofac Implants. 2001;16(3):418-26. [ Links ]
9. Hansson HA, Albrektsson T, Brånemark PI. Structural aspects of the interface between tissue and titanium implants. J Prosthet Dent 1983;50(1):108-13. [ Links ]
10. Härtel J, Pögl C, Henkel KO, Gundlach KK. Dental implants in alveolar cleft patients: a retrospective study. J Craniomaxillofac Surg 1999;27(6):354-7. [ Links ]
11. Holm-Pedersen P, Lang NP, Müller F. What are the longevities of teeth and oral implants? Clin Oral Implants Res 2007;18 Suppl 3:15-9. [ Links ]
12. Horiuchi K, Uchida H, Yamamoto K, Sugimura M. Immediate loading of Brånemark system implants following placement in edentulous patients: A clinical report. Int J Oral Maxillofac Implants 2000;15(6):824-30. [ Links ]
13. Isono H, Kaida K, Hamada Y, Kokubo Y, Ishihara M, Hirashita A, et al. The reconstruction of bilateral clefts using endosseous implants after bone grafting. Am J Orthod Dentofacial Orthop 2002;121(4):403-10. [ Links ]
14. Jaffin AR, Kumar A, Berman LC. Immediate loading of implants in partially and fully edentulous jaws: a series of 27 case reports. J Periodontol 2000;71(5):833-8. [ Links ]
15. Jansma J, Raghoebar GM, Batenburg RH, Stellingsma C, van Oort RP. Bone grafting of cleft lip and palate patients for placement of endosseous implants. Cleft Palate Craniofac J 1999;36(1):67-72. [ Links ]
16. Kearns G, Perrott DH, Sharma A, Kaban LB, Vargervik K. Placement of endosseous implants in grafted alveolar clefts. Cleft Palate Craniofac J 1997;34(6):520-5. [ Links ]
17. Kramer FJ, Baethge C, Swennen G, Bremer B, Schwestka-Polly R, Dempf R. Dental implants in patients with orofacial clefts: a long-term follow-up study. Int J Oral Maxillofac Surg 2005;34(7):715-21. [ Links ]
18. Krieger O, Matuliene G, Hüsler J, Salvi GE, Pjetursson B, Brägger U. Failures and complications in patients with birth defects restored with fixed dental prostheses and single crowns on teeth and/or implants. Clin Oral Impl Res 2009;20(8): 809-16. [ Links ]
19. Lilja J, Yontchev E, Friede H, Elander A. Use of titanium dental implants as an integrated part of a CLP protocol. Scand J Plast Reconstr Surg Hand Surg 1998;32(2):213-9. [ Links ]
20. Misch CE, Wang HL, Misch CM, Sharawy M, Lemons J, Judy KW. Rationale for the application of immediate load in implant dentistry: part I. Implant Dentistry 2004;13(3): 207-17. [ Links ]
21. Rezende ML, Amado FM .Osseointegrated implants in the rehabilitation of a patient with cleft palate and ectodermal dysplasia: a case report. Int J of Oral Maxillofac Implants 2004;19(6):896-900. [ Links ]
22. Ronchi P, Chiapasco M, Frattini D. Endosseous implants for prosthetic rehabilitation in bone grafted alveolar clefts. J Craniomaxillofac Surg 1995;23(6):382-6. [ Links ]
23. Sabri R. Cleft lip and palate management with maxillary expansion and space opening for a single tooth implant. Am J Orthod Dentofacial Orthop 2000;117(2):148-55. [ Links ]
24. Schnitman PA, Wöhrle PS, Rubenstein JE, DaSilva JD, Wang NH. Ten-year results for Brånemark implants immediately loaded with fixed prostheses at implant placement. Int J Oral Maxillofac Implants 1997;12(4):495-503. [ Links ]
25. Takahashi T, Fukuda M, Yamaguchi T, Kochi S. Use of endosseous implants for dental reconstruction of patients for dental reconstruction of patients with grafted alveolar clefts. J Oral Maxillofac Surg 1997;55(6):576-83. [ Links ]
26. Verdi FJ Jr, SLanzi GL, Cohen SR, Powell R. Use of the Brånemark implant in the cleft patient. Cleft Palate Craniofac J 1991;28(3):301-4. [ Links ]
 Corresponding Address:
Corresponding Address:
Maria Lúcia Rubo de Rezende
Alameda Dr. Octávio Pinheiro Brisolla, 9-75
CEP 17012-901 – Bauru/SP, Brazil
Phone: (55) 14 3235-8278
E-mail: malurezende@usp.br
Received in:8/2/11
Accepted in: 30/3/11
