










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRPG. Revista de Pós-Graduação
versão impressa ISSN 0104-5695
RPG, Rev. pós-grad. vol.18 no.1 São Paulo Jan./Mar. 2011
ORIGINAL ARTICLE
Relationship between quality of water supply and extrinsic dental color
Relação da qualidade da água de abastecimento público e manchas dentárias
Kathleen Rebelo de SousaI; Maria Eliana Cruz de AlmeidaII; Cristiane Santos da SilvaIII; Maria da Luz Rosário de SousaIV
IPhD in Public Health, University of Campinas (UNICAMP) – Piracicaba/SP, Brazil.
IIPhD in Pediatric Dentisty, University of Campinas (UNICAMP) – Piracicaba/SP, Brazil.
IIIPDDS, Pediatric Dentisty, University of Amazonas (UEA) – Manaus/AM, Brazil.
IVPhD in Public Health, University of São Paulo – São Paulo/SP; Full Professor, University of Campinas (UNICAMP) – Campinas/SP, Brazil.
ABSTRACT
Changes in tooth color are a common esthetic problem in patients exposed to certain extrinsic or intrinsic factors. Among the extrinsic factors, the heavy metals deserve highlighting. Therefore, this study aimed to verify if there is association between the water consumed by residents from Caapiranga, Amazonas (Brazil) and changes in tooth color. This is a cross-sectional descriptive study. The calculated sample size (n = 350) was based on the prevalence of the phenomenon would be the maximum possible (50%) in a city not to exceed 100,000 people. Residents were examined by a dental surgeon from the Family Health Program staff in regular home visits. The clinical examination was carried out with a wood spatula under natural light. The water samples were collected in resistant plastic bottles. There were three collections in each well, with minimum volume of water (500 mL) to perform the analysis and then assess all metals of the study. There were 30 collections, since 10 wells were analyzed. The analyzed metals were: aluminum, antimony, arsenic, cadmium, lead, copper, cobalt, chromium, iron, magnesium, mercury, nickel, selenium, and zinc. Descriptive statistics were used and the measure of Odds Ratio (OR) for association checking. It was found that the only metal in excess was iron (0.4 to 4.3 mg/L) in water samples and 16.9% of staining in the teeth of residents of this sample (n = 332). There was an association between the staining and the presence of iron in the supply water (p = 0.015), presenting OR = 2.16(1.10 – 4.23). The quality of the water supply in some points of Caapiranga was in disagreement with the tolerable level for the presence of iron in water (0.33 mg Fe/L). As for the other metal the levels were within the limits of tolerance. It is suggested that teeth stain needs further studies because they can be an important indicator of the presence of iron and/or other metals in the water.
Descriptors: Oral health. Dental enamel. Water supply.
RESUMO
Mudanças na cor do dente são um problema estético comum em pacientes expostos a determinados fatores extrínsecos ou intrínsecos. Entre os fatores extrínsecos, os metais pesados merecem destaque. Assim, este estudo teve como objetivo verificar se existe associação entre a água consumida por moradores de Caapiranga, Amazonas (Brasil) e mudanças na cor do dente. Este é um estudo descritivo transversal. O cálculo do tamanho da amostra (n = 350) foi baseado na prevalência do fenômeno como sendo o máximo possível (50%) em uma cidade não superior a 100.000 pessoas. Moradores foram examinados por um cirurgião-dentista da equipe do Programa Saúde da Família em visitas domiciliares regulares. O exame clínico foi realizado com uma espátula de madeira, sob luz natural. As amostras de água foram coletadas em garrafas de plástico resistente. Foram realizadas três coletas em cada poço, com volume mínimo de água (500 mL) para realizar a análise e avaliação de todos os metais do estudo. Havia 30 amostras, já que 10 poços foram analisados. Os metais analisados foram: alumínio, antimônio, arsênio, cádmio, chumbo, cobre, cobalto, cromo, ferro, magnésio, mercúrio, níquel, selênio e zinco. A estatística descritiva utilizada foi a medida de Odds Ratio (OR) para verificar associação. Verificou-se que o único metal em excesso era o ferro (0,4 a 4,3 mg/L) em amostras de água e 16,9% de coloração nos dentes dos moradores desta amostra (n = 332). Houve associação entre a coloração e a presença de ferro na água de abastecimento (p = 0,015), apresentando OR = 2,16 (1,10 – 4,23). A qualidade do abastecimento de água em alguns pontos de Caapiranga estava em desacordo com o nível tolerável para a presença de ferro na água (0,33 mg Fe/L). Quanto aos outros metais os níveis estavam dentro dos limites de tolerância. Sugere-se que a mancha dental necessita de mais estudos, pois pode ser um importante indicador da presença de ferro e/ou outros metais na água.
Descritores: Saúde bucal. Esmalte dentário. Abastecimento de água.
INTRODUCTION
Brazil is considered a privileged country in terms of water resources availability, because it has a great reserve of the fresh water available in the world. Even though, until the end of the past century, water was considered as an abundant and practically inexhaustible resource13, perhaps containing organisms, substances, compounds and elements that were detrimental to health4.
The chemical quality of the water is closely associated to the natural environment and to the human actions2. Therefore, the term “heavy metals” is used for chemical elements that contaminate the environment, causing different damages to the biota, and may be metals, semimetals or even non-metals as selenium. The main chemical elements labeled in this concept are: aluminum, antimony, arsenic, cadmium, lead, copper, cobalt, chromium, iron, manganese, mercury, molybdenum, nickel, selenium, and zinc16.
In Brazil many regions live together with the excess of iron in its groundwater, particularly the one captured in ancient land9. The ions iron and manganese, frequently found in groundwater, are the most abundant materials in the crust. The presence of iron in drinking water causes serious esthetic problems7.
The use of products containing high amounts of iron or iodine may be associated to a significant blackpigmentation on teeth. The exposure to sulfide, silver nitrate or manganese may cause stains that vary from grey to yellow, brown or black. Copper or nickel may produce a green stain; cadmium may be associated to a yellow to golden-brown pigmentation10. Ergo, the association between the presences of heavy metals in water with tooth color change is a relatively new matter, and therefore, there are not many articles in literature about this specific association. Development of studies on this association is of fundamental importance and great value, since it harms the esthetics of these individual immensely.
OBJECTIVES
The main objective of this research was to investigate if the water consumed by the residents from Caapiranga, Amazonas was contaminated by heavy metals and if these could be associated to such changes. The specific objectives were to analyze the physical and chemical characteristics of the water used by this population, to check what elements in the water could lead to tooth color change and to verify if there are specific points in the urban area, which the problem occurs or if it is generalized.
MATERIAL AND METHODS
The city of Caapiranga has 9,617 km2 of land area, being divided into the headquarters, where the public agencies and institutions are located, such as the executive, legislative and judicial; and the many communities that are both politically and administratively subordinated to the city. In a straight line, the distance between Caapiranga and the State Capital, Manaus, is 147 km. As to the waterway distance, it is approximately 438 km. The access to the county is mainly done through water transportation15.
The water supply service is provided by Amazonas Sanitation Company (COSAMA). Regarding the urban zone, the population that is served by the public supply network is equivalent to 63.73%, while the ones served by wells come to a total of 28.01%, and the remaining people use water directly from the river. It is noteworthy that there is no water treatment plant (ETA) in Caapiranga, Amazonas.
This is a cross-sectional descriptive study to verify if there is association between the water consumed by residents from Caapiranga city, Amazonas, and changes in color tooth, which covered the population living in the urban area of Caapiranga, Amazonas, which amounts to 3,561 habitants, according to data provided by Municipal Health Department of Caapiranga, this population is divided into 13 micro areas (Family Health Program – PSF), it was statistically analyzed in order to determine how many individuals would be investigated. The calculated sample size was 350 individuals; this calculation was based on the formula, which the prevalence of the phenomenon would be the maximum possible (50%) in a city not to exceed 100,000 people, as is the case in this study. These individuals were distributed into 13 micro areas (1st stage); therefore, from each micro area about 10% was randomly selected, for homogeneous distribution of the investigated population. This percentage was reached having as 2nd stage the draw for families in each micro area until it reached the desired value, since all components of the families were examined (Tabela 1).
Non resident individuals from the urban area of Caapiranga, Amazonas, and/or who did not consume water from the region, and people who presented tooth color change coming from intrinsic factors such as: amelogenesis imperfecta, dentinogenesis imperfecta, dental fluorosis, erythropoietic porphyria, hyperbilirubinemia, decomposition of red blood cells, supplements containing iron, iodine, potassium, calcium, etc.
Water samples were obtained from residence of the individuals involved in the research. Even if more than one person came up with the referred changes and both used the same water source, it was performed only one collection for both.
Among the activities carried out by the PSF staff, there are the home visits, which aim at checking the overall health of residents, guidance on hygiene, disease detection, and verification of oral conditions among others.
The Oral Health staff during the home visits identified the individuals selected for the survey, they were informed on what the study was about and the possibility to participate, if they agreed, they were enrolled in the study, written informed consent was obtained for every patient. Then, we proceeded to clinical examination aiming at finding whether or not there were changes in tooth color and water samples were collected for later analysis. The research was approved by the CEP/ESA-UEA nº 068/08.
The clinical examination was carried out with the help of a disposable wood spatula under natural light, having the dentist duly protected with the use of mask, cap and gloves.
The individuals in which the presence of tooth color change was detected were enlightened about the problem and forwarded to the Health Basic Unit Selestino André de Souza, for the carrying out of dental consultations and conduction of the referred case.
The water samples were collected in resistant plastic bottles, which were chemically inert, providing a tight seal.
There were three collections in each well, with minimum volume of water (500 mL) to perform the analysis and then assess all metals of the study. There were 30 collections, since 10 wells were analyzed.
The study area covered 13 micro areas, from all these micro areas samples were collected from 10 different wells, since some wells supply more than one micro area. The micro areas which were supplied by the same water source were: micro areas 1 and 2 (same well), micro areas 3 and 4 (COSAMA), and the others were the regular way.
The analyzed metals were: aluminum, antimony, arsenic, cadmium, lead, copper, cobalt, chromium, iron, magnesium, mercury, nickel, selenium, and zinc.
The collection, safety and measuring equipments were selected regarding the required samples. The internal parts of bottles and lids were not to be touched by hands. The sample bottles were only opened during the necessary time for their filling, and were kept away from sunlight.
Once collected, the sample was transported to the laboratory so that its integrity was guaranteed and its preservation time respected.
The reference documents were Standard Methods, Collection of Samples, and Sample Storage and Preservation3.
In order to analyze the data, descriptive statistics were used; for association checking the measure of Odds Ratio (OR) was performed.
RESULTS
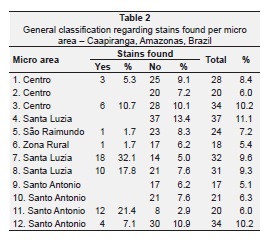
The research involved 332 individuals (there was loss of 18 individuals) divided into 13 micro areas, from these 56 had extrinsic stains, and the highest percentage found was in micro area 7, equaling 32.1% (Table 2).
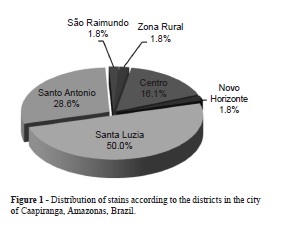
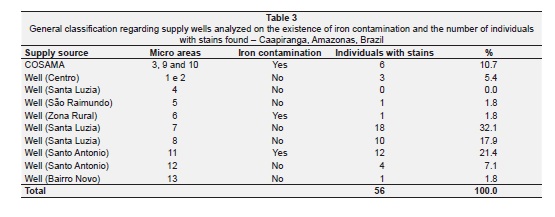
Analyzing the distribution of stains according to district, we verify that 50% are concentrated in the Santa Luzia district, 28.6% in the Santo Antônio district, and 16.1% in the Centro district (Figure 1). In laboratory analysis of the water, only iron was found in excess in three distinctive supply points, whichare the following: COSAMA (micro areas 3, 9 and 10), Santo Antônio well (micro area 5) and the Zona Rural well (micro area 6) (Table 3). The levels of iron contamination vary from 0.4 to 4.3 mg/L.
In micro area 3 (supplied by COSAMA), we found six people who showed stains, representing 10.7% out of the total found, and the highest level of iron contamination (4.3 mg/L). Another source where iron contamination was detected, was micro area 6, where only one person showed stains representing 1.8% out of total, and a level of contamination of 0.8 mg/L. The supply well from micro area 5, also presented iron contamination, in this micro area we found 12 people who showed yellow stains on their teeth, this total represents 21.4% out of the identified total (Table 3).
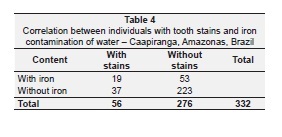
The chi-square test demonstrated there is association between the staining and the presence of iron in the supply water from Caapiranga, Amazonas (p = 0.015), presenting OR = 2.16 (1.10 < OR < 4.23), existing therefore 2.2 more chance of showing staining in the individuals who consumed water with iron. The data demonstrated association between the existence of heavy metal and the presence of dental staining (Table 4).
DISCUSSION
This study was conducted as it was noted that several individuals sought care in the health units of Caapiranga, Amazonas, aiming getting explanations regarding the frequent appearance of dental staining, requesting the removal of their teeth and at the same time complaining that this staining undermined severely their esthetics.
It was noted that there is an association between the dental staining and the presence of iron in the water, what points to the need for better control and monitoring of the water that supplies the city of Caapiranga, Amazonas.
Many factors may cause dental staining mainly when associated with each other. In a study conducted by Nordbø, Kolstø and Eriksen11, they noted that lactoferrin (bactericidal protein found in saliva) and the iron present in human saliva, produce an increase in the staining of tooth enamel, another factor pointed by Addy et al.1, that may be associated with dental staining is the high consumption of tea, coffee and wine, which according to Olson and Stookey12, these beverages contain a considerable amount of tannic acid, what may produce staining. A common eating habit in the North Region is the consumption of açaí, which according to Menezes, Torres and Sabaa Srur8, has the mineral iron in its composition (4.5 mg in 100 g of pulp). These facts, associated with the iron contamination in the water from Caapiranga may be increasing the dental staining in the residents from this city, however these pointed variables were not assessed in this study, what brings us to recommend that new researches be carried out for the understanding of dental staining.
It is vital to know the etiology of health problems in general, for a correct planning of the means of prevention and treatment. Researchers such as Loureiro, Adde and Peres.6 informed that heavy metals like lead, mercury and bismuth, when ingested or inhaled, can potentially cause a linear pigmentation along the edge of the gums. This pigmentation is directly linked to inflammatory processes, which increase vascular permeability, allowing the deposition of these metals in the cervical gingival margins through precipitation with sulfites released by local bacteria. In the present study, the inflammatory processes were not assessed and the only metal that appeared above level was iron, which contamination in the water showed to be associated to staining, having residents of the affected areas, 2.2 more chances of presenting dental staining. It is clear that the presence of heavy metals in public water supply can interfere with the oral health of individuals, and there should be greater effort by the authorities to control the means of treatment of water supplied to the population.
Regarding the laboratory examination of the water, we must take into account the precepts of Freitas, Brilhante and Almeida5, which states that “in the distribution systems of drinking water, its quality can suffer a series of changes, making the water quality at the tap of the user to be different from the one leaving the treatment plant and such changes can be caused by chemical and biological variations or integrity loss of the system”.
According to Rocha, Pereira and Pádua15 low concentrations of metals in water are often detected, but this fact is illusory because, as a result of anaerobic conditions, there is formation of insoluble salts and elimination by sedimentation. To Freitas, Brilhante and Almeida5, metals in the water distribution system may origin from the variability of water quality that the distribution system may show or be related to this fact. Two origins can be given: the first concerns the very system that provides the metal, mainly through microbiological or chemical corrosion, the second source concerns the origin of water entering the treatment plant, where mainly aluminum and iron form compounds used in the clotting process which goal is the removal of suspended particles in the water that flows into the treatment plant5.
These changes in quality in the water from the source (well or COSAMA) and tap water that reaches the user may be one of the explanations for the contamination found in the waters of COSAMA, the well in Santo Antônio in micro area 5, and the well in Zona Rural in micro area 6. Since during the course of the water from the source to the consumer, there may have been a variation in its quality with the aggregation of contaminants, which due to the poor conditions of sanitation and poor water quality, the water-borne diarrheal diseases, such as typhoid fever, cholera, salmonellosis, shigellosis and other gastroenteritis, poliomyelitis, hepatitis A, worms, amoebiasis and giardiasis in the developing countries have been responsible for several outbreaks and high rates of infant mortality related to human water consumption5.
The wells have a key role in providing water to low-income families, including the families in the state of Amazonas. For this reason, it is recommended its protection with the elimination of possible contaminant causes, as well as filtration and disinfection to reduce the possibility of pathogen transmission. Given the above it is essential to make people aware of the importance of maintaining the wells. Since its construction, the wells must follow the technical and operational standards to prevent contamination that could compromise the quality of groundwater posing a risk to human health17.
CONCLUSION
We conclude, through the research carried out, that the quality of the water supply in the county of Caapiranga, Amazonas, in three supply points was detected in disagreement with the tolerable level for the presence of iron in water (0.33 mg Fe/L). As for the other metal the levels were within the limits of tolerance.
The association between the contamination of the water supply by heavy metals and the presence of change in dental color, there were 2.2 times more likely to have this association.
Further research is needed to examine what factors could be responsible for the appearance of changes in dental color in the residents of the county of Caapiranga, Amazonas, and which damages it could cause to this population beyond the aesthetic problems initially reported by the residents of this city, as well as the sending of this data to the authorities about the amounts of iron above the standard. It is suggested that teeth stains are further studied, because they can be an important indicator of the presence of iron and/or other metals in the water.
ACKNOWLEDGMENT
This research was supported by Fundação de Amparo à Pesquisa do Estado do Amazonas (FAPEAM).
REFERENCES
1. Addy M, Moran J, Davies RM, Beak A, Levis A. The effect of single morning and evening rinses of cholorhexidine on the development of tooth staining and plaque accumulation. A blind cross-over trial. J Clin Periodontol 1982:9(2);134-40. [ Links ]
2. Carvalho MN, Santana DC, Abreu, CA, Silva VL, Motta M. Remoção do ferro da água potável da Grande Recife por adsorção em materiais naturais: Fase II – Avaliação comparativa da baronesa com o bagaço de cana-de-açúcar. 23° Congresso Brasileiro de Engenharia Sanitária e Ambiental, 2003.
3. Chemyka Consultoria Química LTDA. Chemyka, 2008. [ Links ]
4. Di Bernardo L. Métodos e técnicas de tratamento de água. ABES, Rio de janeiro 1993;1:481. [ Links ]
5. Freitas MB, Brilhante OM, Almeida LM. Importância da análise de água para a saúde pública em duas regiões do Estado do Rio de Janeiro: enfoque para coliformes fecais, nitrato e alumínio. Cad Saúde Pública;17(3):651-60 [ Links ]
6. Loureiro CC, Adde CA, Perez FE, Penha SS. Efeitos adversos de medicamentos tópicos e sistêmicos na mucosa bucal. Rev Bras Otorrinolaringol 2004;70(1):106-11 [ Links ]
7. Madeira VS, José HJ, Moreira RFPM. Utilização de carvão adsorvente para remoção de íons ferro em águas naturais, 2002. (citado 2007 Dez 10). Disponível em: http://www.enq.ufsc.br/labs/ldpt/artigo%20meio%20filtrante.pdf [ Links ]
8. Menezes EM, Torres AT, Sabaa Srur AU. Valor nutricional da polpa de açaí (Euterpe oleracea Mart) liofilizada. Acta Amazonica 2008;38(2):312-5. [ Links ]
9. Nascimento-Filho DG, Pereira AG. Remoção de ferro em águas de abastecimento, maximização da eficiência dos processos oxidativos, seguidos de filtração direta – condicionantes e resultados práticos. 23° Congresso Brasileiro de Engenharia Sanitária e Ambiental, 2003.
10. Neville BW, Damm DD, Allem CM, Bouquot JE, et al. Patologia Oral e Maxilofacial. Rio de Janeiro: Guanabara Koogan, 1998. [ Links ]
11. Nordbø H, Kolstø AB, Eriksen HM. Salivary lactoferrin in a selectes group of subjects with exceptional extrinsic dental staining. J Oral Pathl 1987;16(8):392-4. [ Links ]
12. Olson B, Stookey GK. An in vitro model for studying stain formation on intact enamel. J Dent Res 1981;60: Special issue A, abst 629. [ Links ]
13. Pereira WS, Freire RS. Ferro zero: Uma nova abordagem para o tratamento de águas contaminadas por compostos orgânicos poluentes. Quim Nova 2004;28(1):130-6. [ Links ]
14. Rebouças A. Águas Doces no Brasil – capital ecológico, uso e conservação. 2 ed. São Paulo: Escrituras, 2002.
15. Rocha AA, Pereira DN, Pádua HB. Produto de pesca e contaminantes químicos na água da represa Billings, São Paulo (Brasil). Rev Saude Publica 1985;19(5):401-10 [ Links ]
16. Secretaria de Assistência a Saúde. Secretaria Municipal de Saúde de Caapiranga – SEMSA, Caapiranga 2008. [ Links ]
17. Tsutiya MT. Metais pesados: O principal fator limitante para o uso agrícola de biossólidos das estações de tratamento de esgoto. 20° Congresso Brasileiro de engenharia Sanitária e Ambiental, 1999. [ Links ]
 Corresponding address:
Corresponding address:
Kathleen Rebêlo de Sousr
Rua Maceió, 618, apto 902 – Edifício Saint Remy – Adrianópolis
CEP 69053-730 – Manaus/AM, Brazil
Phone: (55) 92 3584-1962
e-mail: kathleenrebelo@gmail.com
Received in: 4/3/11
Accepted in: 31/3/11
