










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRFO UPF
versão impressa ISSN 1413-4012
RFO UPF vol.16 no.3 Passo Fundo Set./Dez. 2011
Repair of composite restorations – Teaching information from dental schools of the State of Rio Grande do Sul (RS), Brazil
Reparo de restaurações de resina composta – informações sobre o ensino em escolas de odontologia do estado do Rio Grande do Sul (RS), Brasil
Catiane Betina Tovo*; Eduardo Dickie de Castilhos**; Sinval Adalberto Rodrigues-Junior***
* Graduate student, School of Dentistry, Federal University of Pelotas, RS, Brazil.
** MS, Adjunct Professor, Department of Public Health, School of Dentistry, Federal University of Pelotas, RS, Brazil.
*** PhD, Titular Professor, School of Dentistry, Universidade Comunitária da Região de Chapecó, SC, Brazil.
Abstract
Objective: The present study analyzed the teaching of repair of direct composite restorations (RCR) and its determining factors in Dental Schools of the State of Rio Grande do Sul (RS), Brazil. Methods: Eight Schools were selected based on registration on the website of the Ministry of Education (MEC). A first contact was made by phone, and the e-mail of the head of the Restorative Department was obtained. A questionnaire was elaborated containing 19 questions, and was e-mailed to the dental schools. Data was analyzed by descriptive statistics. Results: Six from the eight schools selected returned the questionnaire. All participating schools fulfill and teach RCR and consider the technique successful as treatment. The schools did not present any reason for not accomplishing it. The main indications for repair were shade correction, fracture of the material and fracture of the tooth. In most schools the nature of the teaching is theoretical, in clinical disciplines. Conclusions: A consistent conduct towards teaching RCR was observed from 100% of the participating schools. Most of them consider it a definitive treatment, revealing a trend towards the preservation of tooth structure.
Key-words: Dental restoration repair. Composite resins. Teaching. Dental schools.
Resumo
Objetivo: O presente estudo analisou o ensino do reparo de restaurações de resina composta (RRRC) direta e seus fatores determinantes nas escolas de odontologia do estado do Rio Grande do Sul (RS), Brasil. Materiais e método: Oito escolas foram selecionadas com base nos registros do sítio do Ministério da Educação. Um primeiro contato foi feito por telefone, e o e-mail do chefe do Departamento de Odontologia Restauradora foi obtido. Um questionário foi elaborado contendo 19 questões e enviado às escolas. Os dados foram analisados por estatística descritiva. Resultados: Seis das oito escolas deram retorno aos questionários. Todas as escolas participantes executam e ensinam RRRC e consideram a técnica efetiva como tratamento. As escolas não apresentaram razões para não executar RRRC. As principais indicações foram correção de cor, fratura do material e fratura do dente. Na maioria das escolas a natureza do ensino é teórica, em disciplinas clínicas. Conclusões: Uma conduta consistente a favor do ensino do RRRC foi observada em 100% das escolas participantes. A maioria considera o reparo de restaurações um tratamento definitivo, revelando uma tendência à preservação da estrutura dentária.
Palavras-chave: Reparação de restauração dentária. Resinas compostas. Ensino. Escolas de odontologia.
Introduction
Recent advances in the technology of adhesive systems and composite resins have improved the longevity of composite restorations. Even so, a considerable amount of failures still happen, and the substitution of the restoration fatally leads to weakening of the tooth by loss of sound tooth structure1,2. The main causes of failure of composite restorations are marginal opening associated to secondary caries, fracture of the restoration, marginal degradation, discoloration and wear of the restoration3.
Most of the dentist's time is dedicated to the substitution of restorations4. The criteria normally used in clinical evaluations of direct composite restorations are subjective and unspecific, leading to variability in the diagnostic of quality of the restorations5. Besides, the fact of being a dentist does not guarantee that the examiner is an acceptable observer for inspection of caries. Therefore, the establishment of criteria to evaluate the quality of restorations and the real need for substitution is imperative to avoid overtreatment6. More than that, the examiners should be trained and the results of this training should be measured somehow5.
Usually, restorative failures, independent of the cause, lead to the substitution of the restoration, in creasing the size of the cavity7. This is particularly true when tooth-colored restorations are fully replaced8. Repairing the defective restoration has been considered a less invasive alternative, restricted to the defect site. This approach ultimately preserves sound tooth structure and reflects the emerging minimally invasive dentistry philosophy2,9.
Even though few clinical studies exist evaluating the feasibility and the longevity of repair in composite restorations (RCR)2, these few studies have generated evidence of clinical success using this approach (up to 2 years longevity) and suggest the RCR as a reliable and promising alternative to the substitution of defective restorations10. According to these authors, RCR might be made in the presence of localized defects, such as superficial marginal staining, shade correction, marginal defects, fracture of the restoration, fracture of the tooth, and even in the presence of secondary caries lesions. Comparatively to the substitution of the entire restoration, this approach helps to reduce pulpal damage, preserves the mechanical strength of the tooth and reduces the clinical time2.
Despite the evidenced advantages of RCR, the commitment to this procedure has been lower than the expected, even in the academy. Previous studies reported that 83% of the European Dental Schools taught RCR2, while 71% of the North-American dental schools taught this procedure1. The schools that did not teach RCR reported lack of clinical experience, lack of scientific evidence and lack of case reports as reasons for not teaching it1,2.
Until the present moment, little is known about teaching of RCR in Brazilian dental schools. In light of the fact that clinical decisions, habits and behaviors of dentists start being defined in the academic environment, the analysis of this issue in Brazilian dental schools is of extreme importance. Therefore, this study aimed to analyze the teaching of RCR in dental schools of the State of Rio Grande do Sul (RS), Brazil.
Materials and method
The project was approved by the institutional Committee of Ethics in Research under the protocol no. 092/2009. The universities were identified based on registration at the Ministry of Education (MEC) website (www.mec.gov.br), verified in September 2007. The universities located at the State of Rio Grande do Sul were included in the study. Those that presented more than one campus had the central campus submitted to the evaluation. Contact information such as address, e-mail and telephone numbers were also collected from the MEC website. Eight universities were selected for the study: University of Passo Fundo (UPF), University of Santa Cruz do Sul (UNISC), Federal University of Pelotas (UFPel), Federal University of Rio Grande do Sul (UFGRS), Lutheran University of Brasil (ULBRA - Canoas), Federal University of Santa Maria (UFSM), Pontifical Catholic University of Porto Alegre (PUCRS) and Centro Universitário Franciscano (Unifra).
The heads of the Restorative Dentistry discipline were contacted, first by phone call and second by e-mail, in order to be informed about the study and its objective. A questionnaire was elaborated containing eight closed, nine semi-open and two open questions, based on previous studies1,2. The respondents were asked about their experience in executing and teaching RCR, reasons for teaching or not teaching RCR, information about the nature of the teaching process, patient's acceptance and technical issues. The questionnaire was previously submitted to professors and post-graduate students (n = 10) of the study institution to verify clearness and coherence of the questions. In August 2009 the questionnaires were e-mailed along with a consent term to the heads of the Operative Dentistry disciplines of the participating dental schools. A 7-day deadline was established, after which a reminding e-mail was sent.
Results
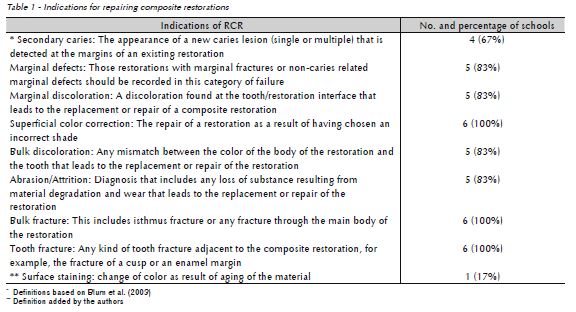
Six (75%) out of eight dental schools returned the questionnaire. Two schools belonged to Federal Universities and the other four to Private Universities. All respondents stated that they repair failed composite restorations and consider the RCR successful as treatment alternative. Also, all schools reported to teach RCR in undergraduate level and had no reasons for not teaching it. The indications of RCR taught in the respondent Dental Schools are specified in Table 1.
Below are other findings from the schools investigated:
– The rate restoration size/area to be repaired was the most cited limitation, followed by tooth sensitivity as a result of dental intervention or deep caries, esthetics and recurrent caries. Other situations included difficulty of access, difficulty of humidity control, unfavorable cost/ benefit relationship, acceptability of the patient, fracture, marginal staining, extensive secondary caries and mechanical loading at the repair area.
– The nature of the teaching of RCR was mostly theoretical in clinical disciplines (83%).
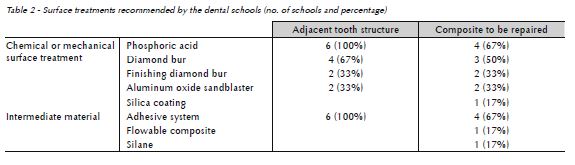
– All schools stated that they recommend preparing the surface of the tooth adjacent to the restoration by associating mechanical surface treatment with intermediate materials. When it comes to the surface of the restoration to be repaired, though, only 67% of the schools stated that they recommend any treatment. Table 2 shows the alternatives of surface treatment by the Dental Schools investigated.
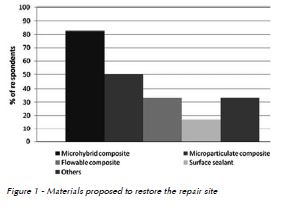
– Most of the dental schools recommend a microhybrid composite to restore the repair site (Fig. 1).
– Most of the schools consider the RCR as a definitive alternative, which lasts more than twelve months (Table 3).

– The criteria elected by the schools to consider the RCR clinically satisfactory were categorized as follows: function, anatomy, marginal sealing, esthetics, biofilm retention and absence of secondary caries.
– Four schools (67%) present a recall system for control of the procedures executed. The other two schools (33%) do not have this system.
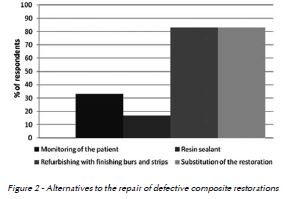
– Alternatives to the RCR when this treatment is considered unfeasible are shown in Fig. 2.
Discussion
The first purpose of our study was to analyze the practice of teaching of RCR in Dental Schools of the State of Rio Grande do Sul and the determining factors, based on information from the schools involved (whether they were public, private or community schools, whether they had post-graduation programs in the area) and the board of professors. Ones expectations were that institutional aspects such as the presence of post-graduation course and professor's time of graduation, place of graduation, post-graduation formation and clinical practice experience would interfere in the decision-making process related to the RCR. However, the lack of compliance made unviable the analysis of these factors, and confirmed a trend of low participation level in behavioral studies, probably by misjudgment of their importance by the research subjects.
Dental science worldwide has moved towards the basic research, with high technological involvement and yet, few impact to the dental practice. The relevance of this study relies on the fact that it analyses practices related to the dental profession, approximating the dental research of the daily clinical problems11. Moreover, it requires low-tech and impacts both clinicians and researchers, helping the development of in vitro studies that might solve clinical dilemmas.
Our findings showed that all the dental schools of RS perform and teach RCR at undergraduate level and, based on their experience, they consider the technique successful. In 83% of the schools the nature of the teaching is theoretical and occurs in clinical disciplines. This contrasts with the North- American schools where the teaching of RCR happens in a practical level, in clinical and pre-clinical disciplines1. The incorporation of the RCR by the schools investigated reveals the commitment with the preservation of the tooth structure that otherwise would be lost and the familiarity with the concept of minimally invasive dentistry.
On the other hand, 29% of the North-American dental schools do not teach RCR due to lack of clinical evidence1, and do not intend to teach it within the next three years, in spite of the benefits reached and extensively reported with the technique2. Most of the decision-making process in dentistry has historically occurred based on personal clinical experience. However, when it comes to the academy, this attitude is of great concern and reveals the need for additional researches that convert the experience into scientific evidence1.
Difficulty in distinguishing secondary caries from marginal staining commonly leads to replacement of the restoration, generating overtreatment. Therefore, the criteria used for diagnostic of the quality of dental restorations, including the presence of secondary caries, should make part of the daily practice of dentists. Secondary caries was pointed out as an indication for repairing the restoration by 67% of the schools (Table 1). Other indications included superficial color correction, bulk fracture and tooth fracture.
According to the schools investigated, some situations are considered limitations for the execution of RCR, such as extensive repair area proportionally to the entire restoration, the presence of tooth sensitivity due to previous restorative intervention or deep caries, the presence of recurrent caries or difficulty of moisture control or access.
Tooth sensitivity has been mentioned as a shortcoming associated to composite restorations. Postoperative sensitivity in composite restorations results from the incorrect application and solvent evaporation of the adhesive system12. Using the state-of-the-art adhesive technique with a threestep total-etch adhesive system has been shown to produce similar pulpal results of amalgam restorations12.
When it comes to the extension of the restoration involvement, the RCR could be performed when less than half of the restoration area is involved; the opposite situation does not imply any advantage by repairing the restoration. Moisture control is considered a pre-requisite for RCR the same way it is to make a new restoration. Considering that rationale and the fact that the entire restoration is replaced when the RCR is not possible, one should not consider the difficulty of moisture control as a limitation for RCR. On the other hand, difficulty of access should be taken into consideration when it involves loss of additional tooth structure to perform the repair, situation that might occur in proximal boxes of class II restorations.
All schools recommend treating the tooth structure adjacent to the restoration to be repaired using phosphoric acid and adhesive (Table 2). Four schools (67%) also recommend using diamond burs. In spite of the fact that little information on the surface treatment of the tooth structure is available, it seems reasonable to think that treating it the same way it is treated for a conventional restoration is the best alternative.
The surface treatment of the restoration to be repaired has two goals: (1) to clean the surface, increasing the surface energy, and (2) to promote surface irregularities, increasing the retention capacity13. The phosphoric acid, recommended by 67% of the schools, cleans the surface of the restoration14. Though, the acid does not promote any surface irregularity, and should be associated to a mechanical treatment, such as grinding with diamond burs or sandblasting with either aluminum or silica oxide particles14-16. The pattern of surface roughness and retention capacity of the old composite is strongly affected by the cutting instruments used. In fact, variable smearing, roughness and matrix cracking are created by different grit diamond burs or by different size sandblast particles1,16. In spite of being an effective surface treatment for composites, the sandblasting was suggested by a few schools, probably because it demands additional chair-side equipment (microetcher). Also, little is known about the effect of the particles over the tooth surface, namely the occlusion of dentin tubulli before adhesive infiltration.
High composite-composite repair bond strength is achieved using the association of surface treatment and application of a low-viscosity intermediate material1,16-18. The intermediate materials wet the treated surface of the composite, penetrating irregularities that probably would not be penetrated by the new composite layer. The participating schools reported using adhesive, flowable composite and silane as intermediate materials, being the former the most cited. In addition to the micromechanical penetration into the composite surface, the adhesive also might react with remaining free radicals of the old composite, while the silane promotes adhesion to the exposed filler particles of the old composite16. Specific primers for composite-repair bonding are also commercially available, and have provided promising bond strength results19. Previous studies indicate a tendency of similarity of bond strength, regardless the intermediate material used, provided that a chemo-mechanical surface treatment is performed beforehand16.
No consensus has been reached about the best protocol for RCR so far. Even so, in vitro studies have shown that using surface treatments and lowviscosity intermediate materials provides repair bond strength of up to 80% of the cohesive strength of the composite18. Moreover, some clinical investigations present the RCR as an acceptable and promising alternative to the substitution of the entire restoration10. Our results reveal that 83% of the dental schools from the State of Rio Grande do Sul (Brazil) consider the RCR as a definitive approach, with more than 12 months of expected longevity2.
Future researches should focus on the investigation of the practice of RCR by graduated dentists and extend the research object of this study to other dental schools in Brazil.
Conclusions
Teaching of RCR is part of the curriculum of the Operative Dentistry discipline of all Dental Schools of RS, mostly in a clinical level. Most of the schools consider the RCR as a definitive approach, and reveal a trend of compromise with the preservation of the tooth structures.
References
1. Gordan VV, Mjör IA, Blum IR, Wilson N. Teaching students the repair of resin-based composite restorations: A survey of North American dental schools. J Am Dent Assoc 2003; 134(3):317-23. [ Links ]
2. Blum IL, Schriever A, Heidemann D, Mjör IA, Wilson NHF. The repair of direct composite restorations: an international survey of the teaching of operative techniques and materials. Eur J Dent Educ 2003; 7(1):41-8.
3. Manhart J, Chen HY, Hamm G, Hickel R. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent 2004; 29(5):481-508.
4. Mjör IA. Placement and replacement of restorations. Oper Dent 1981; 6(2):49-54.
5. Cvar JF, Ryge G. Reprint of criteria for the clinical evaluation of dental restorative materials. Clin Oral Investig 2005; 9(4):215-32.
6. Elderton RJ. Treating restorative dentistry to health. Brit Dent J 1996; 181(10):362.
7. Sardenberg F, Bonifácio CC, Braga MM, Imparato JCP, Mendes FM. Evaluation of the dental structure loss produced during maintenance and replacement of occlusal amalgam restorations. Braz Oral Res 2008; 22(3):242-6.
8. Gordan VV, Mondragon E, Shen C. Replacement of resinbased composite: evaluation of cavity design, cavity depth, and shade matching. Quintessence Int 2002; 33(4):273-8.
9. Mjör IA. Clinical diagnosis of recurrent caries. J Am Dent Assoc 2005; 136(10):1426-33.
10. Gordan VV, Riley III JL, Blaser PK, Mjör IA. A 2-year clinical evaluation of alternative treatments to replacement of defective amalgam restorations. Oper Dent 2006; 31(4):418- 25.
11. Mjör IA. Practice-based dental research. J Oral Rehabil 2007; 34(12):913-20.
12. Opdam NJM, Bronkhorst EM, Roeters JM, Loomans BAC. A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent Mater 2007; 23(1):2- 8.
13. Hannig C, Sebastian L, Hahn P, Attin T. Shear bond strength of repaired adhesive filling materials using different repair procedures. J Adhes Dent 2006; 8(1):35-40.
14. Papacchini F, Dall'Oca S, Chieffi N, Goracci C, Sadek FT, Suh BI, et al. Composite-to-composite microtensile bond strength in the repair of a microfilled hybrid resin: effect of surface treatment and oxygen inhibition. J Adhes Dent 2007; 9(1):25-31.
15. Özcan M, Barbosa SH, Melo RM, Galhano GAP, Botino MA. Effect of surface conditioning methods on the microtensile bond strength of resin composite to composite after aging conditions. Dent Mater 2007; 23(10):1276-82.
16. Rodrigues-Junior SA, Ferracane JL, Della Bona A. Influence of surface treatments on the bond strength of repaired resin composite restorative materials. Dent Mater 2009; 25(4):442-51.
17. Brosh T, Bichacho N, Blutstein R. Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. J Prosthet Dent 1997; 77(2):122-6.
18. Shahdad SA, Kennedy JG. Bond strength of repaired anterior composite resins: an in vitro study. J Dent 1998; 26(8):685-94.
19. Tezvergil A, Lassila LVJ, Vallittu PK. Composite-composite repair bond strength: effect of different adhesion primers. J Dent 2003; 31(8):521-5.
 Endereço para correspondência:
Endereço para correspondência:
Sinval Adalberto Rodrigues Junior
Working and mailing address:
Universidade Comunitária da Região
de Chapecó (UNOCHAPECÓ)
Av. Senador Atílio Fontana
591-E – Bairro Efapi
Área de Ciências da Saúde Caixa Postal 1141
89809-000 Chapecó - SC
e-mail: rodriguesjunior.sa@unochapeco.edu.br
Recebido: 12.07.2010
Aceito: 31.05.2011
