










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRFO UPF
versão impressa ISSN 1413-4012
RFO UPF vol.17 no.1 Passo Fundo Jan./Abr. 2012
Radiographic evaluation of antral pseudocyst, Stafne bone cavity and elongated stylohyoid complex
Avaliação radiográfica do pseudocisto antral, cavidade óssea de Stafne e alongamento do processo estilóide
Natália Gomes e Silva LeonardoI; Luiza Helena Silva de AlmeidaI; Fernanda Geraldo PappenII; Ana Paula Neutzling GomesII
IDDS, Faculty of Dentistry, Federal University of Pelotas, Pelotas, Rio Grande do Sul, Brazil.
IIAssociate professor, Department of Semiology and Clinics, Faculty of Dentistry, Federal University of Pelotas, Pelotas, Rio Grande do Sul, Brazil.
ABSTRACT
Objective: The aim of this present study was to determine the prevalence of developing lesions such as: antral pseudocyst, Stafne bone cavity and elongated stylohyoid complex in patients from the Dentistry Faculty of the Federal University of Pelotas – RS – Brazil. Methodology: A total of 667 panoramic radiographies were observed. Dome-shaped, faintly radiopaque lesions arising from the floor of the maxillary sinus were diagnosed as antral pseudocyst; yet, a stylohyoid complex was considered elongated when it presented over 30 mm length; and radiolucent cavity, unilaterally located in the posterior region of the mandible, between the mandibular angle and the third molar area, below the inferior dental canal and slightly above the mandibular basis was considered a Stafne bone cavity. Results: Fourteen cases of Antral pseudocyst were diagnosed. Most of them (93%) were unilateral, with no apparent etiology (86%). The elongated stylohyoid complex was diagnosed in 158 patients (23.68%). The Stafne bone cavity was diagnose in one patient (0.14%) only. Conclusion: It can be concluded that antral pseudocyst and Stafne bone cavity are uncommon lesions in the studied population, while the elongated stylohyoid complex was a common finding, confirming data already reported in the literature.
Keywords: Radiography. Panoramic. Diagnosis. Maxillofacial Development.
RESUMO
Objetivo: o objetivo deste estudo consiste em determinar a prevalência de lesões de desenvolvimento, como pseudocisto antral, cisto ósseo de Stafne e alongamento do processo estiloide em pacientes da Faculdade de Odontologia da Universidade Federal de Pelotas - RS - Brasil. Metodologia: foram avaliadas 667 radiografias panorâmicas dos arquivos da Faculdade de Odontologia da UFPel. Como critérios de diagnóstico, lesões radiopacas em formato de cúpula no assoalho do seio maxilar foram diagnosticadas como pseudocisto antral, bem como foi considerado alongado o processo estiloide com extensão maior que 30 mm e lesões radiolúcidas uniloculares, bem delimitadas, localizadas na região posterior da mandíbula, abaixo do canal dentário inferior foram identificadas como defeito de Stafne. Resultados: foram identificados 14 casos de pseudocisto antral, sendo a maior parte (93%) unilateral e sem causa aparente (86%). O processo estiloide alongado foi diagnosticado em 158 pacientes (23,68%). Apenas em uma radiografia (0,14%) foi observado defeito ósseo de Stafne. Conclusão: pode-se concluir que o pseudocisto antral e o defeito ósseo de Stafne foram alterações incomuns na população estudada, enquanto o alongamento do processo estiloide foi um achado frequente, confirmando dados já relatados na literatura.
Palavras-chave: Desenvolvimento maxilofacial. Diagnóstico. Radiografia panorâmica.
Introduction
All dental clinician should be aware to establish a presumptive diagnosis when observe the existence of some variation of normality in oral and facial area, especially when this abnormality presents characteristic radiographic aspects. Development abnormalities such as antral pseudocyst, Stafne bone cavity and elongated stylohyoid complex are asymptomatic entities usually found in panoramic radiographs. These entities present specific radiographic characteristics, and the patient usually does not show any symptoms or clinical signs related with such alterations1.
The antral pseudocyst is described as a sessile soft tissue elevation on the floor of the maxillary sinus and is caused by the accumulation of inflammatory exudates surrounded by loose connective tissue, and partially lined by superior sinus epithelium, so the reason of being nominated as a pseudocyst2,3. On a panoramic radiograph, an antral pseudocyst presents a dome-shaped, faintly radiopaque lesion arising at the floor of the maxillary sinus. It is a relatively common finding with a prevalence varying between 1.4% and 9.6%4,5.
Elongation of the stylohyoid ligament complex and calcification of the stylohyoid ligament are often reported in the literature. This abnormallymay be associated with Eagle's syndrome, or also to stylohyoid complex syndrome6,7 and its pathogenesis is still not clarified8. Stylohyoid ligament is considered normal when presents until 30 mm long, and its tip is located between the external an internal carotid arteries, just lateral to the tonsillar fossa. It may develop inflammatory changes in the pharyngeal tissues or impinge on the adjacent arteries or sensory nerve endings, promoting symptoms9,10.
Stafne bone cavity was described for the first time in the literature, as a radiolucent cavity, unilaterally located in the posterior region of the mandible, between the mandibular angle and the third molar area, below the inferior dental canal and slightly above the basis mandibulae11. Forward, this entity had been described by numerous names, as static bone cyst, lingual mandibular bone defect, idiopathic bone cavity and lingual mandibular bone depression12-14. This abnormality can also be observed in an anterior lingual location, between the incisor and the premolar areas, above the insertion of the mylohyoid muscle, however, this location is at least seven times less frequent than the posterior lingual one13-16. The etiopathology of the Stafne bone cavity was still not clarified, but the large majority of authors12-15 agree that this entity is originated from the pressure exercised by glandular tissue on the lingual cortical of the mandible. Part of submandibular gland tissue is frequently found in the posterior variant15.
The aim of the present study was to determine the prevalence of development lesions such as antral pseudocyst, Stafne bone cavity and elongated stylohyoid complex in panoramic radiographs of patients who pursued dental treatment in the Faculty of Dentistry of Federal University of Pelotas - RS - Brazil.
Materials and method
The present study was approved by the Research Board and to the Ethics Committee in Research at the Federal University of Pelotas (Pelotas, RS, Brazil).
Panoramic radiographs of patients referred to a dental clinic of a Federal University from Brazil for routine clinical investigation as part of their dental care were used in this study.
Panoramic radiographs that did not show a good radiographic quality were rejected and 667 panoramic radiographs were included in the study. The evaluation of the panoramic radiographies was realized by two examiners after calibration.
The following data were collected: age and gender, clinical and radiological findings, as well as possible related causes to the lesion.
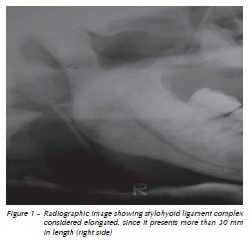
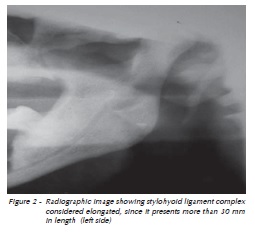
The measurement of the length of the stylohyoid ligament complex was initiated proximally at the point where the stylohyoid ligament complex extended from the temporal bone17, using a 2 times magnifying glass and transparent millimetre radiology ruler on both sides. The lengths of stylohyoid ligament complex were recorded, and whether the condition was bilateral or unilateral was noted. The stylohyoid ligament complex was considered elongated when the length was equal or greater than 30mm (Fig. 1 and 2).
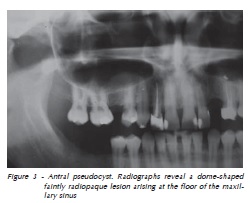
The antral pseudocyst was diagnosed when radiographs revealed a dome-shaped faintly radiopaque lesion arising from the floor of the maxillary sinus (Fig. 3).
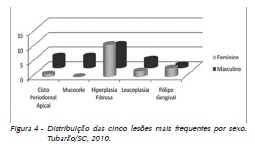
Stafne bone cavity was diagnosed when a unilocular well-defined radiolucent cavity, unilaterally located in the posterior region of the mandible, between the mandibular angle and the third molar, below the inferior dental canal and slightly above the basis mandibulae was found (Fig. 4).
The data was processed using the Statistical Package for Social Sciences verson 9.0 (SPSS; Chicago, USA).
Results
The age of the subjects ranged from 4 to 89 years (mean age, 46.1). In the population studied 60.8% were female and 39.2% were male.
Antral pseudocyst was observed in 14 (2.09%) of the examined panoramic radiographs. The distribution of this entity was exactly the same for both genders. In most part of the patients who presented antral pseudocysts (92.85%) it was observed in an unique side of the face. In 85.71% of the cases, a probable cause could not be noticed.
Styloyoid ligament complex was considered elongated in 158 panoramic radiographs (23.68%), and it was more frequent among females (56.33%). In most part of them, the entity occurred in both sides of the face (57.59%). The mean length of elongated styloyoid ligament complex was 38.11 mm, ranging from 31 to 59 mm. Stafne bone cavity was diagnosed only in one (0.14%) of the 667 panoramic radiographs. The patient who presented this abnormality was a 37 years old male.
Discussion
With the aim of diagnosis and setting up of dental treatment, frequently panoramic radiographs are recommended. This kind of exam allows the diagnosis of bone and dental resorption, cysts, tumours and post-trauma fractures. Panoramic radiographs are also usually required before unerupted, impacted or supernumerary teeth extractions and can still be used to long term follow up of patients after different dental procedures.
The occurrence of some radiographic evidence of abnormality in oral and facial area should be identified by dental clinicians. Antral pseudocyst, Stafne bone cavity and elongated stylohyoid complex are some of these asymptomatic abnormalities which are usually observed in panoramic radiographs1.
A sessile soft tissue elevation on the floor of the maxillary sinus when identified can be diagnosed as antral pseudocyst. The formation of pseudocyst begins by the accumulation of inflammatory exudates delimited by connective tissue, and partially by superior sinus epithelium2,3.
Radiographically, an antral pseudocyst is observed as a dome-shaped, slightly radiopaque lesion at the floor of the maxillary sinus. It is occurrence has a prevalence varying between 1.4% and 9.6%4,5. The results found in the present study is in accordance with these findings, since antral pseudocyst was diagnosed in 2.09% of analysed panoramic radiographs.
The pathogenesis of the antral pseudocyst has not been totally explained. In some cases it is possible to relate it with an adjacent odontogenic infection, or with recurrent upper respiratory infections18. In our study, 85.71% of the cases analysed did not present a probable cause.
Usually, the antral pseudocyst does not require treatment, unless a significant expansion is radiographically evident, or when there are some symptoms associated18. When an adjacent odontogenic infection or a recurrent respiratory infection can be identified, the possible cause should be removed. An antral pseudocyst on the maxillary sinus has previously been a contraindication for sinus augmentation. However, recent studies had described that it is may not be necessary to remove a sinus cyst before sinus augmentation if the patient does not present any symptoms and the cyst is not large19,20, or had described modified surgical techniques which allow the minimally invasive removal of the antral pseudocyst without compromising the nasoantral entrance as well as the anatomy of the sinus for future sinus augmentations21.
Elongation of the stylohyoid ligament complex or calcification of the stylohyoid ligament may be associated with Eagle's syndrome, and its pathogenesis is still not clarified8. A normal stylohyoid
ligament usually presents the length until 30mm, with its tip located between the external an internal carotid arteries, lateral to the tonsillar fossa. Its presence can cause inflammatory alterations in adjacent tissues, promoting symptoms9,10.
Eagle's syndrome occurs when an elongated stylohyoid ligament complex or calcified sylohyoid ligament causes recurrent throat pain, with or without referred pain to the ear and mastoid region on the affected side. The patient can also describe foreign body feeling, dysphagia, or facial pain7. Other symptoms that help in the diagnosis are pain with rotation of the head, recurrent headache, vertigo, facial pain, otalgia and cephalgia6,22. It is also common to note association between these symptoms and temporomandibular disorders23.
Elongated stylohyoid ligament complex was observed in 158 panoramic radiographs, giving an incidence of this abnormality of 23.68%. These results are very similar with those described by Rizatti-Barbosa et al.24, related to be around 20% in adult population. The abnormality was more frequently bilateral (57.59%), what is in accordance with previous reports24.
Different studies show a greater prevalence of an elongated stylohyoid ligament complex in elderly females23,24. These data described in the literature are in accordance with our findings where the occurrence of elongated sylohyoid ligament complex was more frequent among females (56.33%).
When it is assymptomatic, elongated stylohyoid ligament complex will not require treatment. In case of pain, corticoids can be prescribed with good results, and these cases related to strong and persistent pain can be referred to surgery to removal of elongated or calcified stylohyoid ligament complex25.
Stafne bone cavity can be described as a radiolucent cavity, unilaterally located in the posterior region of the mandible, between the mandibular angle and the third molar area, below the inferior dental canal and slightly above the basis mandibulae11. Panoramic radiographs is commonly recommended to minerralized Stafne bone cavity diagnostic in patients presenting pain or dysfunction17,24, since it is able to determine the outline of the cavity and its three dimensional shape26. In the present study, 667 panoramic radiographs were analysed, representing 1334 potential STCs.
The posterior lingual Stafne bone cavity can be observed radiographically in a frequency between 0.10% and 0.48%. Otherwise, when the study was performed in cadavers, the incidence was as high as 6.06%13. It is more frequent in male, and in patients in the 5th or 6th decade of life, although cases have been described in other ages11,16,26. Our findings show a prevalence of stafne bone cavity of 0.14%, since Stafne bone cavity was diagnosed only in one of the 667 panoramic radiographs.
The etiopathology of the Stafne bone cavity was still not clarified, but the large majority of authors12,13,15 agree that this entity is originated from the pressure exercised by glandular tissue on the lingual cortical of the mandible.
Conclusion
The present results confirm other studies, which show that antral pseudocyst and Stafne bone cavity are uncommon abnormalities in population. Elongated stylohyoid complex, however, was observed most frequently in the studied population.
Acknowledgments
Natália Gomes e Silva Leonardo and Luiza Helena de Almeida had their work supported by PET/SISU - Scholarship.
References
1. Quesada-Gómez C, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Stafne bone cavity: a retrospective study of 11 cases. Med Oral Patol Oral Cir Bucal 2006; 11(3):E277-80. [ Links ]
2. Mardinger O, Manor I, Mijiritsky E, Hirshberg A. Maxillary sinus augmentation in the presence of antral pseudocyst: a clinical approach. Oral Surg Oral Med Oral Pathol Endod 2007; 103(2):180-4. [ Links ]
3. Vigneswaran N, Patel PY. Oral and maxillofacial pathology case of the month. Antral pseudocyst.Tex Dent J 2007; 124(11):1140-1, 1146-7. [ Links ]
4. Hadar T, Shvero J, Nageris BI, Yaniv E. Mucus retention cyst of the maxillary sinus: the endoscopic approach. Br J Oral Maxillofac Surg 2000; 38(3):227-9. [ Links ]
5. MacDonald-Jankowski DS. Mucosal antral cysts observed within a London inner-city population. Clin Radiol 1994; 49(3):195-8. [ Links ]
6. Colby CC, Del Gaudio JM. Stylohyoid complex syndrome: a new diagnostic classification. Arch Otolaryngol Head Neck Surg 2011; 137(3):248-52. [ Links ]
7. Politi M, Toro C, Tenani G. A Rare Cause for Cervical Pain: Eagle's Syndrome. Int J Dent 2009; 2009:781297. [ Links ]
8. Manganaro AM, Nylandr J. Eagle's syndrome: a clinical report and review of the literature. Gen Dent 1998; 46(3):282-4. [ Links ]
9. Bafageeh SA. Eagle's syndrome: Classic and carotid artery types. J Otolaryngol 2000; 29(2):88-94. [ Links ]
10. Fini G, Gasparini G, Filippini F, Becelli R, Marcotullio D. The long styloid process syndrome or Eagle's syndrome. J Craniomaxillofac Surg 2000; 28(2):123-7. [ Links ]
11. Stafne E. Bone cavities situated near the angle of the mandible. J Am Dent Assoc 1942; 29:1969-72. [ Links ]
12. Ariji E, Fujiwara N, Tabata O, Nakayama E, Kanda S, Shiratsuchi Y, Oka M. Stafne's bone cavity: Classification based on outline and content determined by computer tomography. Oral Surg Oral Med Oral Pathol 1993; 76(3):375-80. [ Links ]
13. Philipsen H, Takata T, Reichart P, Sato S, Suei Y. Lingual and buccal mandibular bone depressiones: A review based on 583 cases from a world-wide literature survey, including 69 new cases from Japan. Dentomaxillofac Radiol 2002; 31(5):281-90. [ Links ]
14. Turkoglu K, Orhan K. Stafne bone cavity in the anterior mandible. J Craniofac Surg 2010; 21(6):1769-75. [ Links ]
15. Courten A, Kuffer R, Samson J, Lombardi T. Anterior lingual man dibular salivary gland defect (Stafne defect) presenting as a residual cyst. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 94(4):460-4. [ Links ]
16. Katz J, Chaushu G, Rotstein I. Stafne's bone cavity in the anterior mandible: A possible diagnostic challenge. J Endod 2001; 27(4):304-7. [ Links ]
17. Ilgüy M, Ilgüy D, Güler N, Bayirli G. Incidence of the type and calcification patterns in patients with elongated styloid process. J Int Med Res 2005; 33(1):96-102. [ Links ]
18. Gardner DG. Pseudocysts and retention cysts of the maxillary sinus. Oral Surg 1984; 58(5):561-7. [ Links ]
19. Tang ZH, Wu MJ, Xu WH. Implants placed simultaneously with maxillary sinus floor augmentations in the presence of antral pseudocysts: a case report. Int J Oral Maxillofac Surg 2011; 40(9):998-1001. [ Links ]
20. Kara IM, Küçük D, Polat S. Experience of maxillary sinus floor augmentation in the presence of antral pseudocysts. J Oral Maxillofac Surg 2010; 68(7):1646-50. [ Links ]
21. Lin Y, Hu X, Metzmacher AR, Luo H, Heberer S, Nelson K. Maxillary sinus augmentation following removal of a maxillary sinus pseudocyst after a shortened healing period. J Oral Maxillofac Surg 2010; 68(11):2856-60. [ Links ]
22. Diamond LH, Cottrell DA, Hunter MJ, Papageorge M. Eagle's syndrome: a report of 4 patients treated using a modified extraoral approach. J Oral Maxillofac Surg 2001; 59(12):1420-6. [ Links ]
23. Rizatti-Barbosa CM, Lopes EB, Albergaria-Barbosa JR, Gomes BPF. Eagle syndrome associated with temporomandibular disorder: a clinical report. J Prosthet Dent 1999; 81(6):649-51. [ Links ]
24. Rizatti-Barbosa CM, Ribeiro MC, Silva-Concilio LR, Di Hipolito O, Ambrosano GM. Is an elongated stylohyoid process prevalent in the elderly? A radiographic study in a Brazilian population. Gerodontol 2005; 22(2):112-5. [ Links ]
25. Satyapal KS, Kalideen JM. Bilateral styloid chain ossification: case report. Surg Radiol Anat 2000; 22(3-4):211-2. [ Links ]
26. Segev Y, Puterman M, Bodner L. Stafne bone cavity--magnetic resonance imaging. Med Oral Patol Oral Cir Bucal 2006; 11(4):E345-7. [ Links ]
 Correspondence author:
Correspondence author:
Fernanda Geraldo Pappen
Faculdade de Odontologia de Pelotas – UFPel
Departamento de Semiologia e Clínica
Rua Gonçalves Chaves, 457
96015-560 Pelotas - RS
e-mail: ferpappen@gmail.com
Recebido: 16/03/2012
Aceito: 23/04/2012
