










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRFO UPF
versão impressa ISSN 1413-4012
RFO UPF vol.17 no.3 Passo Fundo Set./Dez. 2012
Factors related to self-perceived need for dental treatment in adolescents, adults, and elders in a city in Northeastern Brazil
Fatores relacionados à autopercepção da necessidade de tratamento odontológico em adolescentes, adultos e idosos em um município do nordeste do Brasil
Arinilson Moreira Chaves Lima I; Karla Giovana Bavaresco Ulinski I; Regina Célia Poli-Frederico II; Ana Raquel Benetti III; Flaviana Bombarda de Andrade IV; Marina de Lourdes Calvo Fracasso V; Sandra Mara Maciel V
I MSc, Pos-Graduate student, Department of Preventive and Operative Dentistry, North Paraná University, Londrina, PR, Brazil
II Professor, Dental School, North Paraná University, Londrina, PR, Brazil
III Professor, Dental School, University of Copenhagen, Copenhagen, Denmark
IV Professor, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
V Professor, Dental School, State University of Maringá, Maringá, PR, Brazil
ABSTRACT
Objective: to identify factors related to self-perceived need for dental treatment in adolescents, adults, and elders in a small city in Northeastern Brazil. Methods: Data from a cross-sectional study with a sample of 139 individuals were assessed. Data collection included oral examinations and interviews concerning demographic and predisposing characteristics, and availability of financial resources. In a hierarchical model, Poisson regression analysis was used. Results: Out of the total sample, 85.5%, 84.5%, and 38.5% of the adolescents, adults, and elders, respectively, reported the need for dental treatment. The self-perception of this need was lower among elders who had not received information on how to avoid oral problems, and among the edentulous. On the other hand, it was higher amongst those who self-rated their oral health as fair/poor/very poor. Conclusions: These results highlight the importance of self-rated oral health and the access to preventive information on oral problems in modulating the individual concept of dental treatment need. Moreover, they point to the need for greater attention to the elderly group, mostly edentulous that showed lower perceived need.
Keywords: Oral health. Self-perception. Adolescent. Adult. Elderly.
RESUMO
Objetivo: identificar fatores relacionados à autopercepção da necessidade de tratamento odontológico em adolescentes, adultos e idosos de um pequeno município do nordeste do Brasil. Métodos: Dados de um estudo transversal com uma amostra de 139 indivíduos foram analisados. A coleta de dados incluiu exames bucais e entrevistas sobre características sociodemográficas, de predisposição e disponibilidade de recursos financeiros. A análise de regressão de Poisson, em um modelo hierárquico, foi utilizada. Resultados: Do total da amostra, 85,5%, 84,5% e 38,5% dos adolescentes, adultos e idosos, respectivamente, relataram necessitar de tratamento odontológico. A autopercepção desta necessidade mostrou-se menor entre os idosos, entre os que não haviam recebido informações sobre como evitar problemas bucais, e entre os edentados. Por outro lado, foi maior entre os que autoperceberam sua saúde bucal como regular/ruim/péssima. Conclusões: Estes resultados destacam a importância da autopercepção das condições de saúde bucal e do acesso à informação preventiva sobre problemas bucais para modular o conceito individual de necessidade de tratamento odontológico. Além disso, eles apontam para a necessidade de maior atenção aos idosos, a maioria dos quais desdentados, grupo que apresentou menor necessidade autopercebida.
Palavras-chave: Saúde bucal. Autopercepção. Adolescente. Adulto. Idoso.
Introduction
Measurements of self-rated oral health may be used in population studies or act as a complement to routinely used clinical measurements. Results obtained through self-rated health studies may assist in the selection of treatment, in monitoring patients, in identifying health determinants and risk factors, in the selection of specific services for the population, in the establishment of health services and priorities, and in allocating financial and other resources1,2. Despite its importance, often there are subjective aspects of oral health disregarded in epidemiological studies in contrast with contemporaneous health definitions that include both clinical and subjective aspects3.
An important step to understand the search standard for health services is to know how each individual perceives their own oral health. The results of the Brazilian National Research per Household Sample4 (1998) showed that 96% of the people who did not seek health services declared that they did not do so for they "did not need them" (lack of self-perceived need).
In the last two nationwide epidemiological surveys carried out in Brazil with the purpose of obtaining a diagnosis of the population's oral health, the Projects SB Brasil 20035 (2002-2003 Oral Health Conditions of the Brazilian Population) and SB Brasil 20106 (2010 National Oral Health Survey), in addition to the traditional indexes to assess oral conditions, some subjective information was collected, including self-perceived need for treatment, and self-rated oral health. In the SB Brasil 20106, although an improvement in various oral health normative indicators was verified, high percentiles of caries experience and tooth loss were recorded. The rates of self-referred treatment needs were: 65.1%, 75.2%, and 46.6%, respectively, for adolescents, adults, and elders. Previous studies have shown divergence between people's self-perception and their objective conditions of oral health7-9.
A number of researchers have sought to understand what factors are related to greater or lower self-perceived need for dental treatment in some specific ages. In a national data study on Brazilian adolescents, Bastos et al.10 (2009) observed that self-perceived need for dental treatment was higher in poorer regions. Heft et al.11 (2003) reported a strong association between self-perceived need for treatment by American adults and apparent clinical conditions, such as broken restorations, residual roots, dental mobility, and toothache. Moreira et al.12 (2009) observed that Brazilian non-edentulous elderly felt a greater need for dental treatment than edentulous elderly did, and that the variables associated to the subjective need for dental treatment were different for both groups.
Although some studies have investigated objective and subjective factors related to self-perceived need for dental treatment11,13,14, few have done so based on a previous theoretical model12,15,16, and these ones have investigated the self-perception of adults and elders, analyzing secondary data of national studies. Using the model proposed by Gift et al.15 (1998), Martins et al.16 (2008) found that information, oral health conditions, and subjective questions were associated with the self-perceived need for dental treatment among elderly indivi duals.
According to the Gift et al.15 (1998) model, perceived need for dental treatment is predicted by multiple factors including demographic characteristics, availability of financial resources, predisposing/ enabling factors, and oral health conditions. The demographic characteristics are immutable. The availability of resources can be changed through public policies, directly or indirectly due to increased supply and demand for free public services. The predisposing/enabling factors include resources that provide means for individuals to take action as well as underlying beliefs such as orientations to care, and global health perceptions. These variables influence actual levels of diseases and conditions and self-defined need for treatment.
Very few studies proposed by authorities of Brazilian cities have considered the self-perceived need for dental treatment of their populations in the planning of local policies. The present study aimed to analyze the factors associated to self-perceived need for dental treatment in adolescents, adults, and elders in a small city in Northeastern Brazil.
Methods
This cross-sectional study using secondary data was conducted in the city of Limoeiro do Norte, situated in the Northeast, the poorest region of Brazil, with an estimated population at the time of the study of 54,582 inhabitants17, inserted into different social stratums and with no access to a public supply of water fluoridation.
The epidemiological survey database used was that on the oral health conditions of the population of Limoeiro do Norte, performed by the Health Department of the State of Ceará in partnership with the Municipal Health Department, which used the same methodology as the SB Brasil 20035, which in turn, complied with the recommendations of the WHO - World Health Organization18 (1997). Authorization for the use of data was previously obtained from the Municipal Health Department, and the Permanent Research Ethics Committee of the University of Northern Parana (Pt/0268/2010) approved the study protocol. All participants or their guardians, in case of individuals under the age of 18, provided written informed consents.
Although the total sample of the original survey contained 495 individuals, in the present study only those who answered to the self-reported questions were involved. Thus, the study sample consisted of 139 subjects assigned to 3 age groups-from 15 to 19 years old (n=55), from 35 to 44 years old (n=58), and from 65 to 74 years old (n=26), and it was representative for the size of the city according to the methodology used19,20.
Data collection comprised dental examinations and interviews, using a questionnaire on socio-demographic characteristics, use of dental services, and self-rated oral health. The participants were examined under natural illumination in their respective households, by dentists of Oral Health Teams of the Family Health Program, using community periodontal index (CPI) probes, flat mirrors, and wooden spatulas. In the calibration phase, the percentages of inter and intra-examiner agreements for assessing dental caries were 90% and 97.5%, respectively. More information about the methodology used in the survey are available in other publications 5,20,21.
The secondary data for analysis were obtained by means of the Visual Fox Pro 5.0 software, converted to the Excel software, and subsequently exported to the Statistical Package for Social Science 15.0 software, with which the data was analyzed.
The dependent variable assessed in the present study was the subjective self-perceived need for dental treatment, obtained by means of the following question in the interview: "Do you think you need treatment today?" (yes, no). The independent variables were gathered in four groups (demographic characteristics, availability of financial resources, predisposing characteristics, and oral health conditions), as defined by the Gift et al.15 (1998) model and adapted by Martins et al.16 (2008).
The demographic variables (group 1) were: age (15-19 years old, 35-44 years old, and 65-74 years old), gender (male, female), skin color/race (white and non-white), household location (rural, urban).
The following variables comprised group 2 (availability of financial resources): monthly family income calculated in Brazilian currency - Reais (≥R$ 241.00; R$ 101.00 – R$ 240.00; ≤100.00), car ownership (yes, no), and type of dental service used (private, public).
Variables of predisposing/enabling factors (group 3) were: years of schooling (≥9 years, 5-8 years, ≤4 years), access to information on how to avoid oral problems (yes, no), visit to a dentist at some point in life (yes, no), time in years from the last visit to dentist (≤ 1 year, > 1 year, never went), reason for seeking a dental appointment (routine/preventive, treatment/curative), self-rated oral health, self-rated dental and gum appearance, self-rated chewing ability, self-perception of speech (dichotomized in very good/good, and fair/poor/very poor), self-perceived interference of oral health in relationships (does affect it, does not affect it), reported dental or gum pain in the past six months (yes, no).
The oral health clinical conditions (normative needs) in group 4 were: number of decayed, missing, and filled teeth (DMFT index) (0-9, 10-26, 27- 32), presence of teeth (dentate, edentulous), use of any type of prosthesis (yes, no), untreated dental caries (none, at least one), need for any type of prosthesis (yes, no).
First, the data analysis consisted of a description of the variables and their distribution within each group in order to characterize the population and allow subsequent analyses. Next, the univariate analysis was carried out in each one of the four groups of variables. Poisson Regression model with robust variance was used. Only the variables with a significant level of 20% or lower in the univariate analysis were included in the multivariate hierarchical analyses that followed. Variables were controlled for all others in the same level/group (horizontal), and those with p ≤ 0.05 were retained to the next level down (vertical). The assessment of the associations between the dependent variable and the independent variable was presented as unadjusted and adjusted prevalence ratios (PR), with 95% confidence intervals (95% CI).
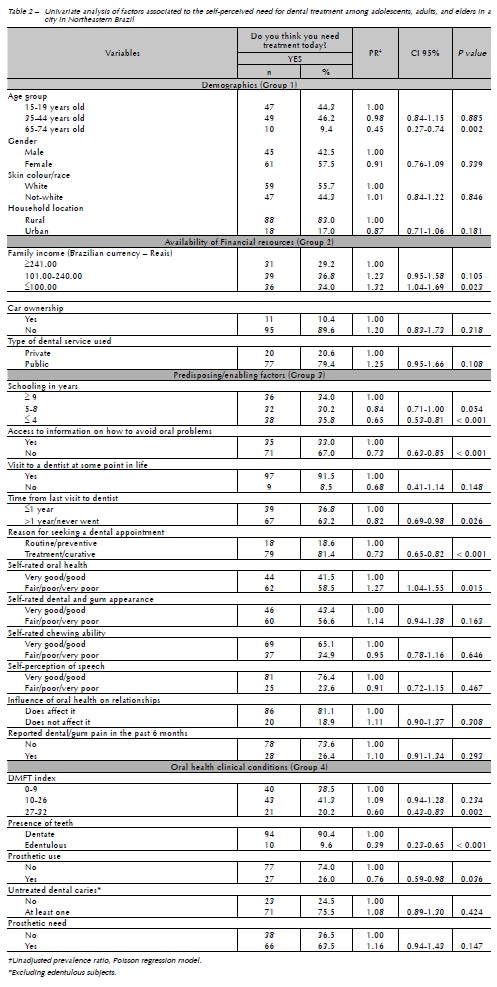
Results From the total number of participants (139) that answered the interview, 1.4% (2) did not undergo oral examinations. Considering the whole sample, 76.2% of the interviewed subjects declared they needed dental treatment. In the stratification by age groups, percentiles were of 85.5%, 84.5%, and 38.5%, respectively, for the groups of adolescents, adults, and elders. Table 1 shows the sample distribution according to the characteristics investigated, grouped as defined by Gift et al.15 (1998). Most of the subjects was women, white, living in rural areas, from low family income, had no car, used public dental services, with < 4 years of formal education, reported not receiving information on how to avoid oral problems, had the last dental appointment > 1 year and for curative reasons, reported not having experienced pain in teeth and/or gums in the six months prior to the interview, were dentate, needed treatment for caries in at least one tooth and needed prosthesis, regardless of the type, in at least one arcade. Regarding the subjective variables, there were similar proportions of individuals' self-rated oral health and appearance of teeth and gums as fair/poor/very poor or very good/good. On the other hand, the majority of them self-rated their chewing ability and speech as very good/good, and considered that oral health had no influence on their social relationships. According to the univariate analysis (Table 2), the higher self-perceived need for dental treatment was statistically related to a family income up to R$ 100.00 and the self-rated oral health as fair/ poor/very poor. On the other hand, the variables: age from 65 to 74 years old, ≤ 4 years of schooling, lack of access to information as to how to avoid oral problems, last visit to dentist more than one year ago, last appointment for curative reason, DMFT index between 27 and 32, edentulism, and use of prosthesis were statistically associated with the lower self-reported need for dental treatment. In the multivariate analysis (Table 3), intermediary models were removed due to their extension. No variable of the resource availability group was retained in the final model. Only the negative self-rated oral health remained related to the higher self-perceived need for dental treatment (PR=1.27; 95% CI: 1.06-1.34). In addition, lower ratios of perceived need remained statistically associated to the following characteristics: ages between 65 to 74 years old (PR= 0.45: 95% CI: 0.27-0.75), lack of information about how to avoid oral problems (PR= 0.80; 95% CI: 0.67-0.96), and edentulism (PR= 0.53: 95% CI: 0.29-0.98). Discussion Combining objective and subjective indicators into a comprehensive model of oral health, the present study identified that demographic, predisposing, and clinical factors were associated with self-perceived need for treatment in a sample of adolescents, adults, and elders of a rural town in northeastern Brazil. In this city, high percentages of adolescents (85.5%) and adults (84.5%) self-referred a current need for dental treatment. These rates were higher than those reported in SB Brasil 20106 for the country as a whole (65.1% and 75.2 %, respectively) and for the northeastern region (72.6% and 79.0%, respectively). These numbers may reflect the poor oral health conditions of the population in the investigated city, and are in agreement with the information shown by the two latest national surveys5,6 where the most unfavorable oral health conditions are registered in cities with smaller populations. However, the low percentile of elders who perceived dental treatment need (38.5%) was even lower than the values found for Brazil (46.6%) and the northeast (49.4%)5. It is worth noting that among the demographic factors assessed, only the age group was associated to the dependent variable and remained up to the final model. Despite the evidence that oral health worsens with aging22, in the present study the lower self-perceived need for treatment in the elderly group (65 to 74 years old) may be related to a certain conformity on their part as to poor dental conditions, or even to tooth loss, and to the false idea that tooth loss is associated with aging as a natural and inevitable process8. Moreover, we must take into account the influence of the Brazilian health care model, which historically has been centered on curative, mutilating, and excluding practices concerning adults and elders23. Regarding the variables of resource availability, in the present investigation, the lowest family income figured as a factor associated with higher self-perceived need for treatment at the univariate analysis. Socioeconomic conditions may have an influence on access and use of dental services and preventive information promoting favorable behavior and attitudes24. The adverse conditions of this population group may have contributed to the lack of access and to foster poor clinical conditions, which subsequently result in higher self-perceived need for treatment. It is worth noting that the association between level of income and perceived need did not remain statistically significant after adjusting for demographic, predisposing, and clinical variables. In the group of predisposing variables, a number of associations with the self-perceived need for dental treatment were also found in the univariate analysis that did not remain in the multivariate analysis. Lower subjective need was related to less educated individuals, those who reported they had never been to a dentist or had been for over a year ago, and those who sought for a dentist for curative reasons. Martins et al.16 (2008) also found an association between self-perceived need and the use and reason for dental visit only at the univariate analysis; however, differently from what was observed in this study, these variables were associated with higher self-perceived need for treatment. In literature, controversial results were found regarding self-perceived need for treatment and use of dental services: Chisick et al.25 (1997) observed better self-perception among individuals who used dental services; on the other hand, Atchison and Dubin26 (2003) observed better self-perception among those who did not use these services. Two predisposing variables remained significant associations in the multivariate analysis. The first was the access to information on how to avoid oral problems. Lower self-perceived need for treatment was found among those who had not received this information. This indicates the importance of health education in modulating the individual concept of dental treatment need, and may explain the variability of results in different surveys, even for similar objective oral health conditions. The same result was found in a previous study10. For Gift et al.15 (1998), self-perception is hypothetically determined by the orientation received in health centers. This hypothesis requires further studies, since those that deal with this kind of association are rather scarce to date. The second predisposing variable that had a significant association with self-perceived need for treatment in the multivariate analysis was self-perception of the oral health condition. The subjective need of dental treatment was higher among those that declared they had fair/poor/very poor oral health conditions. Similar results were obtained in national12,16 and international11,13,15 studies. No significant associations were found with the self-perception of the appearance of teeth and gums, and of chewing ability; or with reports of pain in teeth and/or gums in the months prior to the interview. This absence of association is opposed to the results of previous publications11-13. In assessing the oral health variables of the studied sample, the need for restorative and prosthetic treatment was not associated with self-perceived need for treatment. On the other hand, the presence of edentulism was related to lower self-perception of this need. The discrepancy between subjective treatment needs and normative needs found in oral examinations was shown in other studies16,27,28. The same applies to the results of the SB Brasil 20106 survey which showed that: in the age group from 15 to 19 years old, only 23.9% were caries free; in the age group from 35 to 44 years old, the DMFT index was of 16.75 (with 7.4 for the missing component), only 0.9% were caries free, and only 31.2% did not require a prosthesis; in the age group from 65 to 74 years old, a DMFT index of 27.5 was found (with 25.2 for the value of the missing component), only 0.2% were caries free, and only 7.3% did not need prosthesis. Contrasting with these data, self-perceived need was reported by 65.1% of adolescents and by 46.6% of elders5. Although the sample size was considerably reduced, the robustness of the Poisson regression in a hierarchical statistical model showed consistent results that are similar to those found in literature. It is important to recall the cross-sectional nature of this study, and as such, it affords limitations that are typical of this kind of investigation. It is suggested that other surveys, followed by careful data analysis, be carried out in order to establish a longitudinal perspective. Conclusion The results obtained indicate the importance of self-perceived oral health and access to preventive information on oral problems, in order to modulate the individual concept of dental treatment need. Furthermore, they show the need for paying more attention to elders, since this was the age group, along with the edentulous individuals (mostly elders), who showed lower self-perceived need for treatment, which may lead to a lower search for dental services among other things. This study may provide health authorities, mainly those of small cities, a consistent scientific basis for planning and developing strategies on oral health education and intervention that take into account the subjective criteria studied. References 1. Gift HC, Atchison KA. Oral health, health, and health-related quality of life. Med Care 1995; 33 Suppl 11:NS57-NS77. [ Links ] 2. Sheiham A, Tsakos G. Oral health needs assessments. In: Pine C, Harris R, editors. Community oral health. Mew Malden: Quintessence Publishing Co. Limited; 2007. p. 59-79. 3. Leão ATT, Locker D. Impacto das condições de saúde bucal na qualidade de vida. In: Antunes JLF, Peres MA. Fundamentos de odontologia: epidemiologia da saúde bucal. Rio de Janeiro: Guanabara Koogan; 2006. p. 260-7. 4. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílio 1998: análise dos resultados. [acessado 2011 mar 29]. Disponível em: http://www. ibge.gov.br/home/estatistica/populacao/trabalhoerendimento/ pnad98/saude/analise.shtm. 5. Brasil, Ministério da Saúde, Coordenação Nacional de Saúde Bucal. Projeto SB Brasil: condições de saúde bucal da população brasileira 2002-2003: resultados principais. Brasília; 2004. 6. Brasil, Ministério da Saúde, Coordenação Geral de Saúde Bucal. Projeto SB Brasil 2010: pesquisa nacional de saúde bucal: resultados principais. Brasília; 2011. 7. Silva DD, Sousa MLR, Wada RS. Autopercepção e condições de saúde bucal em uma população de idosos. Cad Saúde Pública 2005; 21(4):1251-59. 8. Martins AMEBL, Barreto SM, Pordeus IA. Auto-avaliação de saúde bucal em idosos: análise com base em modelo multidimensional. Cad Saúde Pública 2009; 25(2):421-35. 9. Bandéca MC, Nadalin MR, Calixto LR, Saad JR, da Silva SR. Correlation between oral health perception and clinical factors in a Brazilian community. Community Dent Health 2011; 28(1):64-8. 10. Bastos JL, Antunes JLF, Frias AC, Souza MLR, Peres KG, Peres MA. Color/race inequalities in oral health among Brazilian adolescents. Rev Bras Epidemiol 2009; 12(3):313-24. 11. Heft MW, Gilbert GH, Shelton BJ, Duncan RP. Relationship of dental status, sociodemographic status, and oral symptoms to perceived need for dental care. Community Dent Oral Epidemiol 2003; 31(5):351–60. 12. Moreira RS, Nico LS, Sousa MLR. Fatores associados à necessidade subjetiva de tratamento odontológico em idosos brasileiros. Cad Saúde Pública 2009; 25(12):2661-71. 13. Ekanayake L, Perera I. Perceived need for dental care among dentate older individuals in Sri Lanka 2005. Spec Care Dentist 2005; 25(4):199-205. 14. Weyant RJ, Manz M, Corby P, Rustveld L, Close J. Factors associated with parents' and adolescents' perceptions of oral health and need for dental treatment. Community Dent Oral Epidemiol 2007; 35(5):321–30. 15. Gift HC, Atchison KA, Drury TF. Perceptions of the natural dentition in the context of multiple variables. J Dent Res 1998; 77(7):1529-38. 16. Martins AMEBL, Barreto SM, Pordeus IA. Fatores relacionados à autopercepção da necessidade de tratamento odontológico entre idosos. Rev Saúde Públ 2008; 42(3):487-96. 17. Instituto Brasileiro de Geografia e Estatística. Estimativa populacional para o ano 2005. [acessado 2010 jun 10]. Disponível em http://www.ibge.gov.br/home/download/estatistica. shtm. 18. World Health Organization. Oral health surveys: basic methods. 4ed. Geneva: WHO; 1997. 19. Brasil. Ministério da Saúde. Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Área Técnica de Saúde Bucal. Projeto SB2000: condições de saúde bucal da população brasileira no ano 2000: manual do coordenador. Brasília: Ministério da Saúde, 2001. 20. Brasil, Ministério da Saúde. Secretaria de Políticas da Saúde. Departamento de Atenção Básica. Área Técnica de Saúde Bucal. Projeto SB 2000: condições de saúde bucal da população brasileira no ano 2000. Brasília: Ministério da Saúde; 2000. 21. Silva NN. Amostragem probabilística. São Paulo: EDUSP; 1998. 22. Rihs LB, Silva DD, Sousa MLR. Dental caries and tooth loss in adults in a Brazilian southeastern state. J Appl Oral Sci 2009; 17(5):392-6. 23. Moreira RS, Nico LS, Tomita, NE, Ruiz T. A saúde bucal do idoso brasileiro: revisão sistemática sobre o quadro epidemiológico e acesso aos serviços de saúde bucal. Cad Saúde Pública 2005; 21(6):1665-75. 24. Pattussi MP, Peres KG, Boing AF, Peres MA, Costa JSD. Self-rated oral health and associated factors in Brazilian elders. Community Dent Oral Epidemiol 2010; 38(4):348–59. 25. Chisick MC, Poindexter FR, York AK. Factors influencing perceived need of dental care by active duty U.S. military personnel. Mil Med 1997; 162(9):586-9. 26. Atchison KA, Dubin LF. Understanding health behavior and perceptions. Dent Clin North Am 2003; 47(1):21-39. 27. Gilbert GH, Branch LG, Longmate J. Dental care use by U.S.veterans elegible for VA Care. Soc Sci Med 1993; 36(3):361-70. 28. Gilbert GH, Heft MW, Duncan RP, Ringelberg ML. Perceived need for dental care in dentate older adults. Int Dent J 1994; 44(2):145-52. 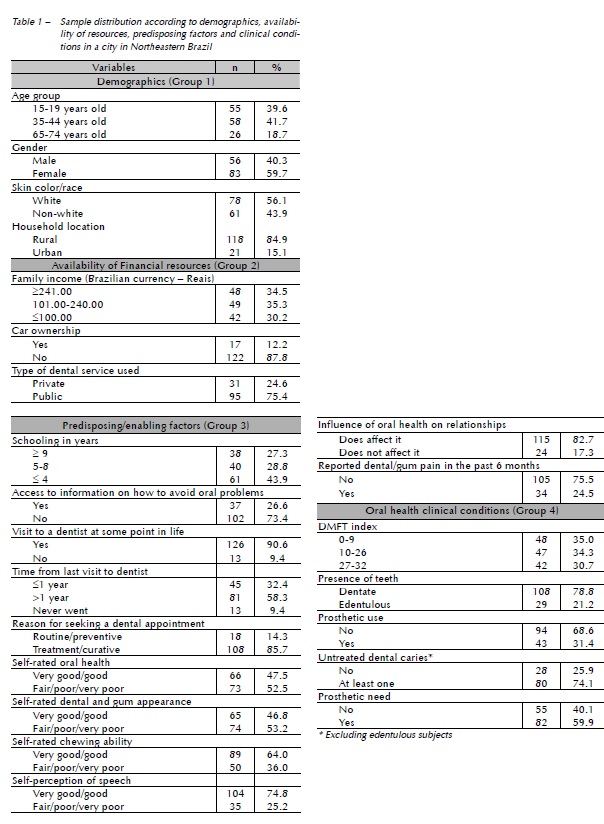

 Endereço para correspondência:
Endereço para correspondência:
Profa. Dra. Sandra Mara Maciel
Rua Brasil, 649 Centro
86010-200 Londrina – PR
e-mail: sanmaciel@sercomtel.com.br
