










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRFO UPF
versão impressa ISSN 1413-4012
RFO UPF vol.21 no.2 Passo Fundo Mai./Ago. 2016
Effectiveness of hand and Mtwo™ instruments in preparing oval-shaped root canals: in vitro study
Efetividade de instrumentos manuais e Mtwo® no preparo de canais radiculares ovais: estudo in vitro
Fernanda Diederichs Coutinho I; Renata Dornelles Morgental II; Simone Bonato Luisi I; Fabiana Vieira Vier-Pelisser III; Patrícia Maria Poli Kopper I
I Departamento de Odontologia Conservadora / Endodontia, Faculdade de Odontologia, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brasil
II Departamento de Estomatologia / Endodontia, Faculdade de Odontologia, Universidade Federal de Santa Maria, Santa Maria, RS, Brasil
III Departamento Clínico / Endodontia, Faculdade de Odontologia, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brasil
Abstract
Objective: This study evaluated through stereomicroscopy the effectiveness of hand and rotary instrumentation techniques, either isolated or combined, in the preparation of oval-shaped root canals. Materials and method: Thirty single-rooted human mandibular incisors were selected. After endodontic access and coronal preflaring, teeth were mounted in a modified Bramante muffle and then sectioned transversely at 3 and 6 mm from the root apex. Images of each section were made under a stereomicroscope at 30× magnification. Teeth were reassembled in the muffle and divided into three groups (n=10) according to the root canal preparation technique: GI - rotary preparation with Mtwo™ basic sequence (10/.04; 15/.05; 20/.06; 25/.06), followed by Mtwo™ complementary instruments (30/.05; 35/.04; 40/.04); GII - rotary preparation with Mtwo™ basic sequence, complemented by hand instruments (#30, #35 and #40); GIII - hand instrumentation using the conventional technique (#10 to #40). All instruments were used in brushing motion. The muffles were separated again so that new images of each section could be obtained. The following parameters were evaluated in pre- and postoperative images: root canal area; perimeter; mesiodistal (MD) and buccolingual (BL) diameters; and mesial (M) and distal (D) wall thickness. Next, the values measured in post- and preoperative images were subtracted for comparison of experimental groups. Data were analyzed using the Kruskal-Wallis test (α=0.05). Results: No significant difference between groups was observed for all parameters. Conclusion: There was no difference among hand, rotary, or combined instrumentation; all techniques were able to increase root canal area, perimeter, and diameter in MD and BL directions. Moreover, the amount of dentin wear on proximal root canal walls was similar for all tested groups.
Keywords: Endodontics. Microscopy. Root canal preparation. Root canal therapy. Stereomicroscopy.
Resumo
Objetivo: este estudo avaliou, por estereomicroscopia, a eficácia da instrumentação manual e rotatória, isoladas ou combinadas, no preparo de canais radiculares de formato oval. Materiais e método: foram selecionados trinta incisivos inferiores humanos com canais únicos. Após acesso endodôntico e pré-alargamento cervical, os dentes foram montados em uma mufla de Bramante modificada e seccionados transversalmente a 3 mm e 6 mm do ápice radicular. Imagens de cada seção foram feitas sob estereomicroscópio com ampliação de ×30. Os dentes foram remontados na mufla e divididos em três grupos (n=10) de acordo com a técnica de preparo do canal radicular: GI - preparo rotatório com a sequência básica do sistema Mtwo® (10/.04; 15/.05, 20/.06; 25/.06), seguido por instrumentos Mtwo® complementares (30/.05; 35/.04; 40/.04); GII - preparo rotatório com a sequência básica do sistema Mtwo®, complementado por instrumentos manuais (#30, #35 e #40); GIII - instrumentação manual, utilizando a técnica clássica (#10 a #40). Todos os instrumentos foram utilizados com movimentos de pincelamento. As muflas foram novamente separadas de modo que novas imagens de cada secção pudessem ser obtidas. Os seguintes parâmetros foram avaliados nas imagens pré e pós-operatórias: área do canal radicular, perímetro, diâmetros mésio-distal (MD) e vestíbulo-lingual (VL), espessura das paredes mesial (M) e distal (D). Em seguida, os valores mensurados nas imagens pós e pré-operatórias foram subtraídos para comparação dos grupos experimentais. Os dados foram analisados pelo teste de Kruskal-Wallis (α=0,05). Resultados: para todos os parâmetros, não foi observada diferença significativa entre os grupos. Conclusão: não houve diferença entre a instrumentação manual, rotatória ou a combinação de ambas; todas as técnicas foram capazes de aumentar a área, o perímetro e o diâmetro do canal radicular, nas direções MD e VL. Além disso, o desgaste de dentina nas paredes proximais foi semelhante para todos os grupos avaliados.
Palavras-chave: Endodontia. Microscopia. Preparo do canal radicular. Tratamento de canal radicular. Estereomicroscopia.
Introduction
Chemomechanical preparation is an important step of root canal therapy. Along with irrigation, the instrumentation removes dentin, pulp remnants, and microbes, allowing proper obturation and contributing to treatment success1. Despite the outstanding technological advance reached in endodontics, mainly in the last two decades, a complete mechanical preparation of the root canal system is rarely achieved2. A major reason is the geometric asymmetry between root canals and endodontic instruments3.
Nickel-titanium rotary instruments were introduced in the 80's and since then several systems have been launched in the market. Regardless of size, taper, or design, these instruments tend to produce round preparations when used with a pecking motion3-5, which in most cases does not match the original root canal shape. Therefore, incomplete cleaning and shaping are usually observed when the canal has an oval or mesiodistal flattened format4. One perception is that recesses of oval canals not included in a round preparation could be instrumented by a circumferential filling movement with small instruments6-8. However, this fact is yet to be confirmed, especially in the middle and apical portion of root canals where instruments may not be easily controlled.
Oval-shaped root canals can be found in all dental groups, but mandibular incisors are especially known by their oval or long oval canals6,9. A canal is considered long oval when its maximum diameter is at least two times larger than the minimum diameter6,10. The oval shape is more common in the middle region of the roots and less frequent in the apical segment6.
Many instruments and techniques have been tested in the preparation of oval-shaped root canals3,4,7,8,11-14. However, incomplete preparations have been observed in most of the aforementioned studies. The MTwo™ system (VDW), which includes narrow instruments with taper up to 7%, was poorly investigated for the preparation of oval-shaped canals, either isolated or in association with other instruments4,5. This system presents S-shaped cross-sectional design and non-cutting safety tip. In addition, the positive rake angle with two cutting edges is claimed to cut dentin effectively with less energy. MTwo™ instruments have an increasing pitch length from the tip to the shaft, which reduces debris accumulation and attain effective cutting action with less risk of fracture15.
Different methods have been used to evaluate the effectiveness of instrumentation techniques. The muffle system proposed by Bramante et al.16 allows comparing the morphological condition of root canals prior and subsequent to chemomechanical preparation, with the initial condition as a control for the instituted therapy. This proposal involves the inclusion of specimens in acrylic resin in which grooves are made to serve as a guide for reassembly. The resin block with the specimen is surrounded by a plaster muffle. The plaster reproduces the grooves of the block and aids further mounting. Over the years, researchers have made changes to this methodology, creating modified muffles5,17.
Based on the above considerations, this study aimed to evaluate the preparation of root canals of mandibular incisors with the MTwo™ system, complemented by instruments of the same system or by hand files, in comparison with hand instrumentation technique alone. A previous study5 suggests that a preparation refinement with either ultrasonic files or hand H-files after using MTwo™ instruments, results in significantly less uninstrumented perimeter in oval-shaped root canals. The hypothesis tested was that the additional use of hand instruments after the initial preparation with rotary instruments would be more effective in preparing oval-shaped canals than thorough preparation with rotaries or hand files.
Materials and method
This study was approved by the Research Ethics Committee at the Federal University of Rio Grande do Sul, Porto Alegre, Brazil (Protocol n. 19704). Thirty human mandibular incisors with mesiodistal-flattened roots were selected. Only teeth with intact or almost intact crown (small decay), complete root formation, and a single root canal without calcifications or previous endodontic treatment were used.
Endodontic access was performed with a diamond round bur (#1012; KG Sorensen, São Paulo, SP, Brazil) at high speed. Root canals were irrigated with 1% sodium hypochlorite (NaOCl) solution, using 30G needle (NaviTip, Ultradent, South Jordan, UT, USA) coupled to 5 mL plastic syringe (Ultradent, South Jordan, UT, USA). The irrigant was simultaneously aspirated with the aid of a suction cannula #20 (Becton Dickinson Ltda, Juiz de Fora, MG, Brazil). Then, canals were explored with size #10 K-files (Dentsply Maillefer, Ballaigues, Switzerland) and tissue remnants were removed.
Next, coronal preflaring was performed with a 20/.06 LA Axxess bur (SybronEndo, Anaheim, CA, USA) coupled to a low-speed handpiece. This bur was introduced with continuous motion in the apical direction until it met resistance. At this moment, it was slowly pulled in the coronal direction with traction movements. Time was recorded during bur use for no longer than 5 seconds. New irrigation was carried out with NaOCl and concomitant aspiration of loosened debris.
To measure the tooth length, a size #10 K-file with silicone cursor was introduced into the root canal until its tip was juxtaposed to the apical foramen. This procedure was performed with the aid of a magnifying glass with 4× magnitude (Bio- Art, São Carlos, SP, Brazil). The silicone cursor was then stabilized in the incisal edge of the tooth. The instrument was removed and the distance between the tip and the cursor was measured with a millimeter ruler (Angelus, Londrina, PR, Brazil). This measure was considered the total tooth length. Working length (WL) was determined by subtracting 1 mm from this value.
Inclusion of specimens in muffles
Specimens were mounted in a modified version of the muffle proposed by Bramante et al.16. Each specimen was embedded in clear acrylic resin (Classic Dental Products Ltd., Toronto, ON), in which two longitudinal grooves and two transverse grooves with depth of 2 mm were made, using carborundum disk (Schelble Ltda, Petropolis, RJ, Brazil). Two sets (resin block + specimen) were positioned within each muffle, which was then filled with stone plaster (Asfer, São Caetano do Sul, SP, Brazil). The grooves of the resin blocks were reproduced on the plaster surface, guiding posterior reassembly of blocks into the muffles.
The muffles were numbered from 1 to 15 and specimens from 1 to 30, arranged two by two in each muffle. The resin blocks were removed from their muffles and sectioned transversely in two root levels previously marked with ink pen: 3 and 6 mm from the apex. A double-sided diamond disc (911 H; Komet Brasseler, Düsserdorf, Germany) with 0.2 mm of thickness was used for this purpose, coupled to a straight handpiece at low speed.
Analysis by stereomicroscopy and root canal preparation
Root sections were analyzed under a stereomicroscope (Zeiss, Jena, Germany) with the coronal face turned up. The images were obtained at 30× magnification with a digital camera, transferred to a computer, and saved in JPEG format.
The resin blocks containing the specimens were reassembled into their muffles and divided into three experimental groups (n = 10) according to the root canal instrumentation technique:
• GI - rotary preparation with NiTi Mtwo™ system (VDW Endodontic Synergy, Munich, Germany), basic sequence, including 10/.04, 15/.05, 20/.06, and 25/.06 instruments, followed by Mtwo™ complementary instruments (30/.05, 35/.04, and 40/.04);
• GII - rotary preparation with NiTi Mtwo™ system, basic sequence, complemented by hand instrumentation, using 30/.02, 35/.02, and 40/.02 stainless steel K-files (VDW);
• GIII - hand Instrumentation by conventional technique using 10/.02 to 40/.02 stainless steel K-files (VDW).
Rotary instruments were driven by an electric motor (Endo ProTorque; VK Driller Ltda, São Paulo, SP, Brazil) at 300 rpm and 2 N.cm. For all groups, brushing movements were applied toward the buccal and lingual walls until the instrument had reached the WL. Time of use for each instrument was standardized in 15 seconds. Irrigation was performed with 2 mL of 1% NaOCl solution after each file exchange. Next, root canals were irrigated with 5 mL of 17% EDTA (Biodinâmica, Ibiporã, PR, Brazil) for 3 minutes18,19. A final irrigation was performed with 5 mL of saline solution.
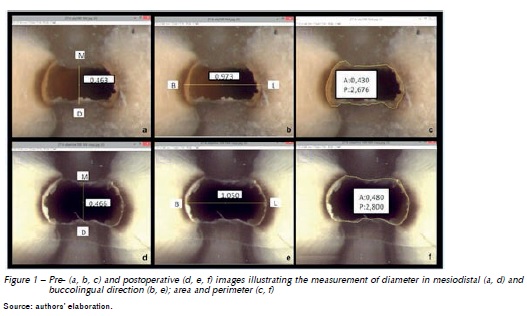
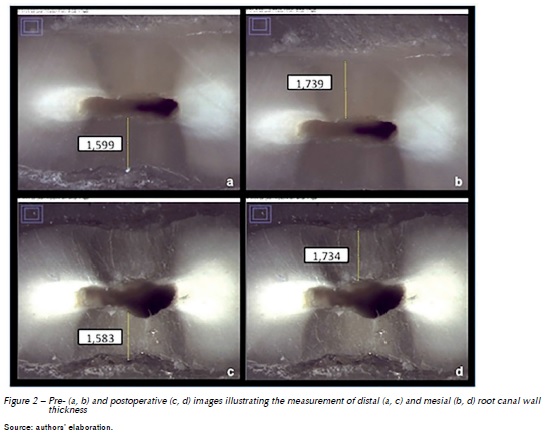
After chemomechanical preparation, the resin blocks containing the specimens were removed from their muffles and new images of each section were taken under the stereomicroscope. Such images were also saved in JPEG format and transferred to the ImageJ software (Version 1.43; National Institutes of Health, Bethesda, Maryland, USA). Software calibration was performed using a standard image of known measure. A blinded and calibrated operator (ICC=0.94) analyzed pre- and postoperative images. The following parameters were assessed: a) root canal area and perimeter; b) root canal diameter in mesiodistal (MD) and buccolingual (BL) direction; c) mesial (M) and distal (D) root canal wall thickness. Figures 1 and 2 illustrate the measurements. The difference between pre- and postoperative values were calculated for group comparisons.
The results for each parameter at 3 and 6 mm levels were compared using the Kruskal-Wallis test. The significance level was set at 5%.
Results
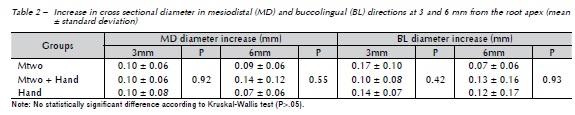
Data analysis showed no significant difference between groups, considering all parameters individually. The results are presented in Tables 1, 2, and 3.


Discussion
There is a high prevalence of oval-shaped root in human teeth, especially in the middle and coronal third of distal roots of mandibular molars and mandibular incisors9,20. This irregular canal format may also be observed in the apical third of several teeth. The percentage of long oval canals in mandibular incisors was 10%, 55%, and 40% at 1, 2, and 3 mm from the apex, according to Wu et al.6. In this context, it is worth noting that rotary instruments produce round preparations, leaving a great portion of the oval root canal without proper cleaning and shaping2,4,13.
Therefore, some authors have suggested the association of different instrumentation techniques as an attempt to reach the buccal and lingual extensions of oval root canals5. The hypothesis that the combination of hand instrumentation after the initial preparation with rotary instruments would be more effective in shaping oval canals than thorough preparation with rotary instruments was not confirmed, considering there was no difference between experimental groups in any tested parameter. However, it is noteworthy that this study did not directly evaluate the untouched areas of oval-shaped canals. Nonetheless, uninstrumented walls were visible in some images. In future investigations, the superimposition of pre- and postoperative images should be considered, as well as the use of high resolution methods such as micro-computed tomography.
In this context, the findings of the present research cannot be fully compared with previous studies that confirmed that preparation of oval canals with rotary instrumentation alone leaves uninstrumented regions3-5,8,13. Direct comparisons cannot be made because of differences in methodological design. For instance, coronal preflaring was performed before apical preparation in this study. This maneuver may have facilitated the access of rotary instruments in the root canal causing easier contact with the walls.
The coronal preflaring procedure during endodontic treatment is important to remove cervical dentin interferences. It allows easier insertion of manual or rotary instruments into the apical portion of root canals and avoids changes in WL during root canal preparation21. Moreover, previous studies have shown that this procedure improves the accuracy of electronic apex locators22.
Another differential of this study, which may have improved the results, was the use of Mtwo™ in brushing motion. Some authors have suggested that NiTi rotary instruments should be used like a 'brush' to optimize preparation effectiveness, particularly in oval canals23, contrary to the original recommendation of using NiTi rotary instruments passively inside the root canals avoiding lateral movements. A past study has shown that pressing motion may reduce the fatigue life of larger size instruments, but the Mtwo™ system may be used safely in brushing action in simulated clinical conditions up to 10 times in oval canals24.
The section of specimens at 3 and 6 mm from the root apex allowed the evaluation of shaping quality at the apical and middle thirds of root canals. Considering that the oval shape prevails in the middle third6, the 6-mm level seems to be the most critical one, and it may be assumed that the regions would not be touched by instruments. This was not confirmed, since root canal diameter increased in both MD and BL directions in all experimental groups. As in the apical third (3 mm), the root canal format usually approaches the circular shape6, therefore the results were not surprising.
Mesial and distal wall thickness was assessed before and after root canal preparation to observe the amount of lost structure when employing each technique. Excessive preparation that leaves very narrow walls (<0.5 mm) is not desirable since it can result in weakened tooth structure prone to fracture25. By the difference observed between preand postoperative images in the three experimental groups, it was possible to observe that the wear was small and, subsequently, excessive and dangerous wear did not occur in any group. None of the techniques tested herein resulted in wall thickness smaller than 0.5 mm (data not shown). A previous study3 observed that Mtwo™ instruments left thin dentin walls (<0.5 mm) in 20% of the cases, however this was mainly observed in mandibular molars, and Mtwo™ was safer than other NiTi systems (ProTaper; Dentsply-Maillefer, Ballaigues, Switzerland).
Another important aspect related to the amount of wear on root canal walls is the penetration of bacteria within dentinal tubules in cases of pulp necrosis and apical periodontitis. It has been shown that the pattern of bacterial infection is variable, with maximum penetration ranging from 60 μm (0.06 mm) in the apical dentin to 200 μm (0.2 mm) in the middle and cervical regions26. According to the values expressed in Table 3, it seems reasonable to say that Mtwo™ instruments remove a substantial amount of infected dentin, but dentists still need to consider the role of irrigating solutions and intracanal medicaments as adjunct methods to mechanical instrumentation.
The NiTi Mtwo™ system (VDW) has shown good results in the preparation of curved root canals15,27. However, its effectiveness in the preparation of oval-shaped canals was poorly investigated5. These authors showed that the preparation of oval-shaped canals with the Mtwo™ system up to 35/.04 instruments should be refined with Hedströem or ultrasonic files to achieve improved results. In the present study, we used the Mtwo™ system up to 40/.04 instruments with a brushing motion. Similarly, to our results, Grecca et al.28 (2007) have not found significant difference among rotary, hand, and ultrasonic techniques in preparing proximally flattened canals. By the results of this research, the Mtwo™ system was effective and safe, although further investigations with high resolution and accuracy methods are necessary. It is noteworthy that the prior coronal preflaring procedure and the use of rotary instruments in brushing action may have favored such results and should be recommended in the preparation of oval canals with Mtwo™ instruments.
Thus, based on the present methodology and results, it is possible to conclude that there was no difference between the techniques used to prepare root canals in both middle and apical segments. All techniques were able to increase the root canal diameter in MD and BL directions, as well as its area and perimeter. Additionally, the amount of dentin wear on proximal root canal walls was similar for all tested techniques.
References
1. Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod 1992; 18(12):625-7. [ Links ]
2. Uzun O, Topuz O, Aydyn C, Alacam T, Aslan B. Enlarging characteristics of four nickel-titanium rotary instrument systems under standardized conditions of operator-related variables. J Endod 2007; 33(9):1117-20.
3. Elayouti A, Chu AL, Kimionis I, Klein C, Weiger R, Lost C. Efficacy of rotary instruments with greater taper in preparing oval root canals. Int Endod J 2008; 41(12):1088- 92.
4. Rodig T, Hulsmann M, Muhge M, Schafers F. Quality of preparation of oval distal root canals in mandibular molars using nickel-titanium instruments. Int Endod J 2002; 35(11):919-28.
5. Pontes CM, Sassone LM, Murad CF, Fidel RA, Vilhena FS. Refinement influence in the cleaning efficacy of rotary nickel-titanium Mtwo instruments in oval-shaped canals by means of optical microscopy. Indian J Dent Res 2014; 25(3):279-83.
6. Wu MK, R'Oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 89(6):739-43.
7. Weiger R, ElAyouti A, Lost C. Efficiency of hand and rotary instruments in shaping oval root canals. J Endod 2002; 28(8):580-3.
8. Wu MK, van der Sluis LW, Wesselink PR. The capability of two hand instrumentation techniques to remove the inner layer of dentine in oval canals. Int Endod J 2003; 36(3):218-24.
9. Mauger MJ, Schindler WG, Walker WA. An evaluation of canal morphology at different levels of root resection in mandibular incisors. J Endod 1998; 24(9):607-9.
10. Jou YT, Karabucak B, Levin J, Liu D. Endodontic working width: current concepts and techniques. Dent Clin North Am 2004; 48(1):323-35.
11. Wu MK, Wesselink PR. A primary observation on the preparation and obturation of oval canals. Int Endod J 2001; 34(2):137-41.
12. Barbizam JV, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J Endod 2002; 28(5):365-6.
13. Ruttermann S, Virtej A, Janda R, Raab WH. Preparation of the coronal and middle third of oval root canals with a rotary or an oscillating system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 104(6):852-6.
14. Paque F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickeltitanium rotary instruments: a micro-computed tomography study. J Endod 2010; 36(4):703-7.
15. Schafer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J 2006; 39(3):203-12.
16. Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod 1987; 13(5):243-5.
17. Kuttler S, Garala M, Perez R, Dorn SO. The endodontic cube: a system designed for evaluation of root canal anatomy and canal preparation. J Endod 2001; 27(8):533-6.
18. Mello I, Kammerer BA, Yoshimoto D, Macedo MC, Antoniazzi JH. Influence of final rinse technique on ability of ethylenediaminetetraacetic acid of removing smear layer. J Endod 2010; 36(3):512-4.
19. Balto H, Salama F, Al-Mofareh S, Al-Yahya F. Evaluation of different irrigating solutions on smear layer removal of primary root dentin. J Contemp Dent Pract 2015; 16(3):187-91.
20. Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, Villas-Boas MH, Amoroso-Silva PA, Brandao CG, et al. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod 2013; 39(12):1529-33.
21. Iqbal A, Akbar I, MK AL-O. An in vivo study to determine the effects of early preflaring on the working length in curved mesial canals of mandibular molars. J Contemp Dent Pract 2013; 14(2):163-7.
22. de Camargo EJ, Zapata RO, Medeiros PL, Bramante CM, Bernardineli N, Garcia RB, et al. Influence of preflaring on the accuracy of length determination with four electronic apex locators. J Endod 2009; 35(9):1300-2.
23. Clauder T, Baumann MA. ProTaper NT system. Dent Clin North Am 2004; 48(1):87-111.
24. Plotino G, Grande NM, Sorci E, Malagnino VA, Somma F. Influence of a brushing working motion on the fatigue life of NiTi rotary instruments. Int Endod J 2007; 40(1):45-51.
25. Hartmann RC, Baldasso FE, Sturmer CP, Acauan MD, Scarparo RK, Morgental RD, et al. Clinically relevant dimensions of 3-rooted maxillary premolars obtained via high-resolution computed tomography. J Endod 2013; 39(12):1639-45.
26. Love RM. Regional variation in root dentinal tubule infection by Streptococcus gordonii. J Endod 1996; 22(6):290-3.
27. Sant'Anna Junior A, Cavenago BC, Ordinola-Zapata R, De-Deus G, Bramante CM, Duarte MA. The effect of larger apical preparations in the danger zone of lower molars prepared using the Mtwo and Reciproc systems. J Endod 2014; 40(11):1855-9.
28. Grecca FS, Garcia RB, Bramante CM, Moraes IG, Bernardineli N. A quantitative analysis of rotary, ultrasonic and manual techniques to treat proximally flattened root canals. J Appl Oral Sci 2007; 15(2):89-93.
 Endereço para correspondência:
Endereço para correspondência:
Renata Dornelles Morgental
Universidade Federal de Santa Maria
Rua Marechal Floriano Peixoto, 1.184
97015-372 Santa Maria, RS – Brasil
e-mail: remorgental@hotmail.com
Recebido: 28/08/2015
Aceito: 12/08/2016
