










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkArquivos em Odontologia
versão impressa ISSN 1516-0939
Arq. Odontol. vol.48 no.3 Belo Horizonte Jul./Set. 2012
ARTIGO ORIGINAL
Accuracy and reproducibility of dental caries risk classification in São Paulo, Brazil
Acurácia e reprodutibilidade da classificação de risco de cárie dentária em São Paulo, Brasil
Henri Menezes KobayashiI; Antonio Carlos PereiraII; Marcelo de Castro MeneghimII; Glaucia Maria Bovi AmbrosanoII
IPost-graduate Program in Dentistry, Piracicaba School of Dentistry, Universidade Estadual de Campinas (UNICAMP), Piracicaba, SP, Brazil
IIDepartment of Social Dentistry, Piracicaba School of Dentistry, Universidade Estadual de Campinas (UNICAMP), Piracicaba, SP, Brazil
ABSTRACT
Aim: To evaluate the accuracy and reproducibility of the dental caries risk classification applied in the state of São Paulo, Brazil, in an attempt to organize the demand for primary care in oral health.
Materials and Methods: Eleven dentists independently examined 120 individuals (75 from 12 to 19 years of age and 45 from 35 to 44 years of age) by visual inspection, and classified them into six codes ranging from A to F, in which code A indicated the healthiest individual (low-risk) and F indicated the sickest individual (high-risk). The agreement between the intraexaminer and the gold standard examiner was evaluated by Kappa. The percentage of agreement, sensitivity, specificity, positive predictive value, and negative predictive value regarding the gold standard examiner was also calculated.
Results: It could be observed that 60.0% of the individuals examined were considered sick, while 40.0% were considered healthy. Values for intra and inter-examiner agreement were k=0.66 and k=0.72, respectively. The percentage of agreement, sensitivity, specificity, positive predictive value, and negative predictive values were 83.8%, 82.5%, 85.8%, 90.2%, and 76.9%, respectively.
Conclusion: This study suggests that the dental caries risk classification, with its various levels of standardization, presented good accuracy and reasonable reproducibility, as well as a low cost and a relatively low demand for resources. As such, this risk classification is recommended for large-scale use.
Uniterms: Dental caries. Epidemiology. Oral health. Primary health care.
RESUMO
Objetivo: Avaliar a acurácia e reprodutibilidade da classificação de risco de cárie dentária utilizada no estado de São Paulo, Brasil, para organização da demanda de atenção primária em saúde bucal.
Materiais e Métodos: Onze dentistas examinaram, independentemente e por inspeção visual, 120 pessoas (75 delas de 12 a 19 anos e 45 adultos de 35 a 44 anos de idade), classificando-as em seis códigos de A a F. O código A classificou o indivíduo de menor risco/mais saudável e o código F aquele de maior risco/mais doente. A concordância intra e inter examinador foi avaliada pelo teste Kappa. A porcentagem de concordância, sensibilidade, especificidade, valor preditivo positivo, valor preditivo negativo foi calculada em relação ao examinador padrão.
Resultados: Dentre os indivíduos avaliados, 60% apresentaram-se doentes e 40,0% saudáveis. A concordância intra e inter examinador foram de k=0,66 e k=0,72. O percentual de concordância, a sensibilidade, a especificidade, o valor preditivo positivo e o valor preditivo negativo foram, respectivamente, 83,8%, 82,5%, 85,8%, 90,2% e 76,9%.
Conclusão: O estudo sugere que a classificação de risco de cárie dentária, com suas devidas padronizações, apresentou boa acurácia e razoável reprodutibilidade, com baixo custo, exigindo pouco recurso e recomendado para ser utilizado em larga escala.
Descritores: Cárie dentária. Epidemiologia. Saúde bucal. Atenção primária à saúde.
INTRODUCTION
Although the prevalence of dental caries has decreased in recent years, it is still the most prevalent disease in the oral cavity, causing several problems and suffering in the Brazilian population1. In Brazil, the prevalence of this disease in 12-year-old children decreased from 2.8 (DMF-T) in 2003 to 2.1 in 20102-3. The results of the oral health status survey of the Brazilian population in 2002-2003 reported another important fact: toothaches proved to be the most common reason why 30.0% of adolescents and 46.0% of adults and the elderly seek dental care3.
The term health risk classify has been widely used, especially in hospitals and emergency clinics, in an attempt to organize the demand for emergency services. This classify is a dynamic process that identifies individuals who need prompt treatment, according to the potential risk of damage to health or the degree of pain4-5.
One of the main concerns in public health is access to dental treatment at the level of basic primary care, especially as regards dental caries. Due to a high demand for this service, it is difficult to ensure the paradigms of universality and equity of access to the entire population6-7. In the city of São Paulo, Brazil, with approximately 11 million inhabitants and 1.515 dentists working in public health services, the technical department of oral health has been using specific criteria to assess the risk of caries in an attempt to prioritize and organize the population that truly reqquires dental care in primary healthcare8-9. This tool consists of classify each individual by their clinical oral health status, divided into six codes (A, B, C, D, E, and F). An individual classified as F needs immediate treatment, while individuals classified as A present no caries and have no restorations10-15. In addition, according to various documents in which this classification is described, it could be observed that there is no standardization of the proposed criteria, causing health professionals to have doubts at the time of clinical examination. Furthermore, to date, there is no report regarding any accuracy test having been performed about this nominal instrument.
To improve oral health related to healthcare, the purpose of this manuscript was to evaluate the accuracy and reproducibility of dental caries riskclassification applied in the state of São Paulo, Brazil, in an attempt to organize the demand for primary care in oral health.
MATERIALS AND METHODS
The sample size was calculated to suit the aim of this study, assuming a confidence level of 95% and a sampling precision level (confidence interval) of +/-10% for the measurements of accuracy and reproducibility, arriving at a minimum sample size of 120 volunteers. Considering that there would be a loss, 160 volunteers were initially selected (80 from 12 to 19 years of age and 80 from 35 to 44 years of age), of both genders, belonging to a Family Health Unit. These were randomly selected and invited by the community health agent to participate in a research project in which the participants would receive free dental treatment by the oral health team of this Family Health Unit.
To evaluate the instrument, 11 dentists from 11 Family Health Units, who used the dental caries risk classification daily when planning oral health actions, were selected to be examiners. The dentist responsible for the research, who had experience in epidemiological surveys, was appointed the gold standard examiner. The evaluation was performed over a two-day period, at a dental clinic in one of the Family Health Units during a period of eight hours each day. On the first day, a theoretical meeting was held with the examiners, lasting one hour. The research and a brief explanation about the dental caries risk criteria were presented. After the meeting, the dentists were provided a note book and pen, which were used to take note of the patient's names and their rating codes. Finally, the professionals went to the dental clinic to perform the clinical examinations.
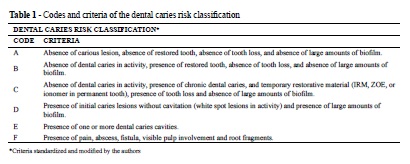
On the first evaluation day, the studies were conducted at the dental clinic, where 144 people were attended to. Patients were seated in dental chairs and were examined by dental surgeons were appropriately clothed with personal protective equipment. In clinical exams, only a wooden spatula and the dental chair reflector were used, without drying teeth with compressed air. Each examiner had 30 seconds to classify the patient's oral health status and record it in the respective examination-record, emphasizing that each patient was examined by the eleven dentists, without communication between examiners. In the literature, due to the non-compliance of the risk ratings in various documents, some minor changes in standardization and risk criteria were made, classifying them according to individual situations shown in Table 110-15.
On the second day of evaluation, 21 days after the first exam, of the 144 people examined on the first day, 122 persons appeared at the Family Health Unit, where the eleven professionals again examined each patient separately. This loss of 22 persons (15.3%) was due to the patients' decision not to continue to participate in the research.
After the clinical exam, patients were referred to the gold standard examiner for dental treatment. This dentist examined each patient individually, evaluating them during a period of 30 minutes (three minutes for the clinical exam, completion of the odontogram and risk classification, and the 27 remaining minutes to complete some form of clinical dental procedure), using a clinical mirror, a CPI millimetric probe (Community Periodontal Index), dentin curettes, drying with compressed air, and a dental chair reflector. Of the 122 patients scheduled, only 02 failed to attend the dental visit. At the end, a total of 120 people were examined. It it is important to note that all the patients scheduled by the gold standard dentist received complete dental treatment, even those who were considered healthy by the eleven examiners.
After having concluded all the tests, the data were organized in Excel 2007. To evaluate reproducibility, statistical tests were performed by analyzing the percentage of intra and interexaminer agreement (Weight Kappa)16-17. When evaluating accuracy, in which sensitivity, specificity, positive predictive value, and negative predictive value were analyzed, the codes were grouped into two groups of oral health situations: codes A, B, and C were considered Healthy, whereas codes D, E, and F were grouped together as Sick. For these groups, the values of intra and inter-examiner agreement (Weight Kappa)were also calculated. All tests were performed using the SAS statistical software (SAS Institute Inc., Cary, NC, USA, 9.2, 2008).
This study was conducted in accordance with the norms and principles recommended by the Research Ethics Committee of the Municipal Health Department in Protocol No. 96/10.
RESULTS
Table 2 shows the absolute frequencies and percentage of the sample evaluated according to age, dental caries risk classification, and oral health status.
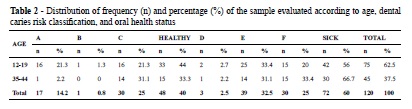
Table 3 shows the intraexaminer analysis with the percentage of agreement, Kappa statistical test and confidence interval for the dental caries risk classification, and oral health status. As regards the dental caries risk classification, the percentage of agreement ranged from 63.3% to 75.8% with a mean of 69.6, while the Kappa ranged from 0.59 to 0.77 with a mean of 0.70. Concerning the health status (Healthy and Sick), the percentage of agreement ranged from 76.9% to 90% with a mean of 83.7% and a Kappa ranging from 0.49 to 0.80 with a mean of 0.66.
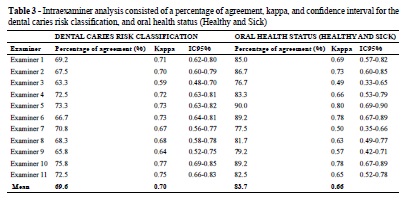
Table 4 shows the percentage of agreement, the Kappa statistical test, and the confidence interval among the 11 examiners regarding the gold standard examiner for the dental caries risk classification. It could be observed that the percentage of agreement ranged from 62.5% to 81.7% with a mean of 70.9%, while the Kappa ranged from 0.6063 to 0.8530 with a mean of 0.7203.
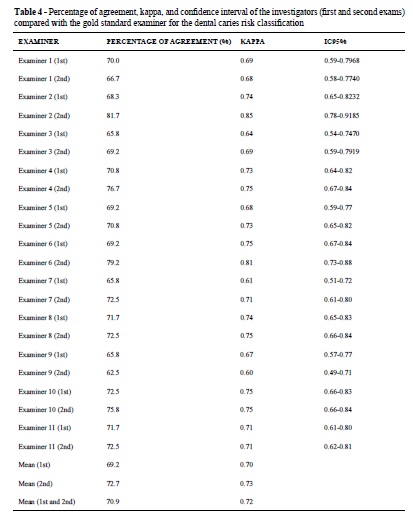
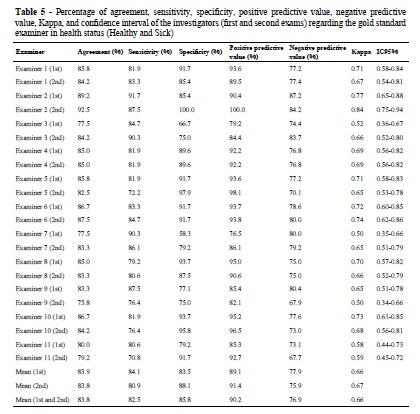
Table 5 shows the percentage of agreement, sensitivity, specificity, positive predictive value, negative predictive value, Kappa, and confidence interval of examiners regarding the gold standard examiner in the health status (Health and Sick). It could be observed that: the percentage of agreement ranged from 92.5% to 75.8% with a mean of 83.8%, sensitivity ranged from 70.8% to 91.7% with a mean of 82.5%, specificity ranged from 58.3% to 100% with a mean of 85.8%, positive predictive value ranged from 76.5% to 100% with a mean of 90.2%, negative predictive value ranged from 67.7 to 87.2%, and kappa ranged from 0.50 to 0.84 with a mean of 0.66.
DISCUSSION
The dental caries risk classification was created to prioritize and organize the demand for the tracking of individuals who require dental treatment, based on the principle of equity of access to health assistance, as well as the optimization of the therapeutic resources for oral health assistance. Although the title of this instrument is the dental caries risk classification, this nominal epidemiological tool only rates the clinical situation of the individual's oral cavity during examination. This instrument is routinely used in clinical dental exams in the public health services of both the state and city of São Paulo10-14. According to some authors, the term risk appears to be much broader, considering that, together with a given clinical situation, it also includes the social, economic, and behavioral aspects, which includes all risk factors for disease development18-20.
This instrument is indicated for use on a large scale, that is, use by a large number of professionals who require the tracking of dental caries quickly and at a low cost, expending few resources (only a wooden spatula is required for the clinical examination). It should be emphasized that this procedure is performed routinely when the oral health services of primary health care in both the state and city of São Paulo select individuals for dental treatment10-14. Only one study could be found in the literature in which the dental caries risk classification used in São Paulo was compared to another dental caries classification performed in Brasilia, which was used to prioritize the treatment of this disease in the Family Health Program. The authors concluded that the criteria proved to be statistically different when determining the priority for dental caries assistance, the nonnormative dimensions of which could complement the findings of the clinical exam21.
Concerning the codes and criteria applied in this study, in accordance with the technical departments of oral health, individuals classified as F are to be scheduled first for immediate dental treatment. Individuals classified as E are those who, after the treatment of those classified as F has begun and if auxiliary oral health staff members are available, are to be scheduled next. While patients with F codes are receiving treatment in the dental chair, those classified as E may receive some therapeutic procedures, such as the application of topical fluoride and oral health advice10-14.
Individuals classified as D are those who are considered to be at risk of getting sick. These individuals will first receive oral health instructions, followed by therapeutic procedures, such as the application of topical fluoride and fluoride varnish, sealants, and dental prophylaxis. As the oral health team also counted on the participation of dental hygienists, these patients were able to receive initial dental care from these professionals. Although the patients classified as C presented no active caries disease, they were the next to be scheduled for treatment, after the treatment of those of codes F, E, and D and provided they had temporary restorations10-14.
Patients classified as B are those who show no signs of caries, but who have already been submitted to dental restorations. These individuals will, if necessary, receive an application of fluoride and oral health advice, as they do not require treatment appointments. It should be pointed out that the recommendations of fluoridated products within the different dental caries risk criteria must take into consideration the conditions of access to fluoridated water10-11,14.
Finally, patients classified as A are those considered at low risk for caries. These individuals will only be given oral health advice as according to the principles of rationalization of fluoride use in public health, fluoride application is generally deemed unnecessary10-11,14.
Due to the nonconformity of criteria in the dental caries risk classification within the literature, it was decided certain points of the instrument's criteria needed to be standardized and improved. For example, the term gingivitis was excluded from codes A, B, C, and D, because in the first documents, this criterion was not recommended, since it was viewed as subjective and indicative of periodontal health. The oral health departments in São Paulo are already using the modified Russell index. Both the State Health Department and Municipal Health Department documents contain several criteria included in the annexes of these documents, which were incorporated into the main classification, such as the presence of provisional restoration in the C code, the large amounts of biofilm in the D code, and the visible presence of pulp involvement in the F code10-15. In addition, fistula and root fragments were also included in the F code, as they were considered to require immediate care and to be the best way to organize the demand, respectively.
This instrument also shows us the oral health conditions in a particular group of individuals. Considering individuals A, B, and C as apparently healthy, and D, E, and F as sick, the data showed that in the group from 12 to 19 years of age, 44.0% were classified as apparently healthy and 56.0% were considered sick, with 2.7% of those considered at risk of getting sick (D) and 20.0% considered to require immediate care (F). However, in the group from 35 to 44 years of age, 33.3% were classified healthy, 66.7% were considered sick, whereas 2.2% were considered at risk of getting sick (D) and 33.4% were considered to require immediate care (F). With this information, the oral health teams can organize, prioritize, carry out strategies, and plan the treatment of these individuals, optimizing the use of oral health equipment, considering the principles of equity to access, consequently improving oral health services7,11,13-14.
The instrument was dichotomized (A, B, and C into Healthy and D, E, and F into Sick) to test precision with regard to dental caries disease. This can be seen in the clinical practice of the public dental services in the state and municipality of São Paulo, where only the individuals with codes D, E, and F would sit in the dental chair, while the individuals with codes A, B, and C would only be given oral health advice and a topical application of fluoride, if necessary11,13-14.
Regarding the reproducibility of the dental caries risk classification, it could be observed that, in the intraexaminer analysis, the mean percentage of agreement was 69.6%, with a mean Kappa of 0.70 and confidence intervals ranging from 0.48 to 0.85. When the codes were grouped into healthy and sick, it could be perceived that the percentage of agreement increased to 83.7%, while the Kappa diminished to 0.66, with confidence intervals ranging from 0.33 to 0.90. It could be verified that the majority of the Kappa interexaminer values remained above 0.60, which is considered good and in substantial agreement. Furhtermore, only e caries risk classification examiner, together with three other examiners when the criteria were grouped, presented values of below 0.60, representing moderate agreement22-23. The weight of kappa statistics are influenced by the prevalence of the disease, and these values may be lower for populations in which the prevalence of caries is higher16-17.
It is important to note that, of the six proposed codes, two present items of subjective criteria, such the "large amounts of biofilm" in code D and the "presence of pain" in code F, which can vary from professional to professional and may well be difficult to measure, with no reliable measurement tool24. Concerning data analyses, it could be observed that the code with the best accuracy and reproducibility was code A, as it seems to lead to an easy classification. The worst classification was code D, because the criterion "large amounts of biofilm" was considered subjective and the "presence of white spot in activity" was difficult to diagnose.
When comparing the interexaminer agreement with the gold standard examiner, it could be verified that the percentage of agreement was 70.9%, with a mean Kappa of 0.72 and confidence intervals of 0.49 to 0.91. All the Kappas of the examiners remained above 0.60 and were considered good and substantial22-23. When the codes were grouped into healthy and sick, it could be observed that the percentage of agreement increased to 83.9%, while the Kappa diminished to 0.66. When grouping the codes for dental caries disease detection (Healthy/Sick), the percentage of agreement proved to be slightly below that recommended by the World Health Organization (85.0%)17. In addition, five examiners obtained Kappa values of below 0.6, which was also considered moderate agreement22-23. These results may well be explained by the fact that, in order to detect caries, the standard examiner used a clinical mirror, probe, and air drying of the teeth, thus making it easier to diagnose more initial active caries lesions, which are difficult to diagnose. By contrast, the other examiners made evaluations using only a wooden spatula and a dental reflector for only 30 seconds25-26. The Technical Departments of Oral Health of the state and municipality of São Paulo recommend only a quick inspection and the use of a wooden spatula for the clinical examination of the population who receives free dental treatment. The use of a clinical mirror, exploratory probe, and air drying could improve these values. The technical departments of oral health are also responsible for carrying out permanent courses among the dentists within the public network for the training and calibration of this instrument.
By means of the positive predictive value (mean of 90.2%), this tool could be considered satisfactory for the tracking of caries diseases, as it is able to identify the truly sick individuals, despite the fact that it is primarily an instrument used for tracking, in which only visual inspection with a wooden spatula is used, as compared to other instruments used to verify this disease25-30. It is also important to remember that this study was conducted within a population with a high prevalence of disease (60.0% of the individuals), which could influence the final results.
The negative predictive value had a relatively lower index than did the other values (76.9%). It could be considered that the high prevalence of caries disease is the main factor in obtaining high positive predictive values and low negative predictive values, which represents a bias in health service research. Furthermore, it could be observed that the examiners had difficulty in diagnosing chronic caries in code C. It should be noted that this diagnosis was made only by visual inspection, with no biofilm removal, which can transform the individual from C to E or vice versa. It is also important to remember that in contemporary literature it is difficult to achieve a gold standard method to diagnose this disease26-30.
Results from the negative predictive value demonstrated that, in clinical practice, for every 20 patients evaluated, approximately five are incorrectly classified as healthy. This result should be further analyzed in the technical areas of oral health to reflect on what option would be best for dental healthcare within public services: (1) to evaluate a larger number of patients at a lower cost, using only wooden spatulas, but not treating some of the sick who were classified as healthy or (2) examine a much lower number of individuals, improving the quality of the clinical exam, using a clinical mirror, exploratory probe, dentin curette with air drying, but at a higher cost, given that these instruments are frequently unavailable in a sufficient quantity for this purpose.
Although the accuracy values were considered satisfactory and those of reproducibility substantial to moderate, it could be observed that the inclusion of drying with compressed air, a clinical mirror, an exploratory probe, a dental chair reflector, and a longer time spent in clinical examination, in addition to standardizing the measurement of subjective criteria, such as the "large amounts of biofilm" in code D, the "presence of pain" in code F, and the diagnosis of chronic carious lesions in code C code could improve the accuracy and reproducibility of these results, considering that a lower amount of available auxiliary resources can lead to a greater underestimation of caries diagnoses26,30.
CONCLUSION
This study suggests that the dental caries risk classification used in basic oral healthcare in the state of São Paulo, with its due standardizations, presents good accuracy and moderate reproducibility, with a low cost and a relatively low demand for few resources. As such, it should be recommended for large-scale use.
REFERÊNCIAS
1. Narvai PC, Frazão P, Roncalli AG, Antunes JL. Cárie dentária no Brasil: declínio, polarização, iniqüidade e exclusão social Rev Panam Salud Publica. 2006; 19:385-93. [ Links ]
2. Roncalli AG. Projeto SB Brasil 2010: pesquisa nacional de saúde bucal revela importante redução da cárie dentária no país. Cad Saúde Pública. 2011; 27:4-5. [ Links ]
3. Ministério da Saúde. Projeto SB Brasil 2003: condições da saúde bucal da população brasileira 2002-2003: resultados principais. Brasília: Ministério da Saúde; 2004. [ Links ]
4. Taboulet P, Moreira V, Haas L, Porcher R, Bragança A, Fontaine JP, et al. Triage with the French emergency nurses classification in hospital scale: reliability and validity. Eur J Emerg Med. 2009; 16:61-7. [ Links ]
5. Ministério da Saúde. Acolhimento e classificação de risco nos serviços de urgência. Brasília: Ministério da Saúde; 2009. [ Links ]
6. Nickel DA, Lima FG, Silva BB. Modelos assistenciais de saúde bucal no Brasil. Cad Saúde Pública. 2008; 24:241-6. [ Links ]
7. Ministério da Saúde. Saúde bucal. Brasília: Ministério da Saúde; 2006. [ Links ] (Caderno de Atenção Básica; nº 17).
8. Morita MC, Haddad AE, Araújo ME. Perfil atual e tendências do cirurgião-dentista brasileiro. Maringá: Dental Press Editora; 2010. [ Links ]
9. Secretaria Municipal de Saúde de São Paulo. Boletim Ceinfo em dados 2010, 9ª ed. São Paulo: Secretaria Municipal de Saúde de São Paulo; 2010. [ Links ]
10. São Paulo, Secretaria de Saúde do Estado. Recomendações sobre uso de produtos fluorados no âmbito do SUS/SP em função do risco de cárie dentária. São Paulo: Secretaria de Saúde do Estado de São Paulo; 2000. [ Links ]
11. São Paulo, Secretaria de Saúde do Estado. A Organização das ações de saúde bucal na atenção básica: versão cidade de São Paulo. São Paulo: Secretaria de Saúde do Estado de São Paulo; 2001. [ Links ]
12. São Paulo, Secretaria Municipal de Saúde. 1° Caderno de apoio ao acolhimento: orientações, rotinas e fluxo sob a ótica do risco/vulnerabilidade. São Paulo: Secretaria Municipal de Saúde de São Paulo; 2004. [ Links ]
13. Bourget IM. Programa Saúde da Família. saúde bucal. São Paulo: Martineri; 2006. [ Links ] (O cotidiano do PSF).
14. São Paulo, Secretaria Municipal de Saúde. Diretrizes para a atenção em saúde bucal : "crescendo e vivendo com saúde". São Paulo: Secretaria Municipal de Saúde de São Paulo; 2009. [ Links ]
15. Sartori LC. Rastreamento do câncer bucal: aplicações no Programa Saúde da Família. [dissertação]. São Paulo (SP): Universidade de São Paulo; 2004. [ Links ]
16. Peres MA, Traebert J, Marcenes W. Calibração de examinadores para estudos epidemiológicos de cárie dentária. Cad Saúde Pública. 2001; 17:153-9. [ Links ]
17. Assaf AV, Zanin L, Meneghim MC, Pereira AC, Ambrosano GM. Comparação entre medidas de reprodutibilidade para calibração em levantamentos epidemiológicos da cárie dentária. Cad Saúde Pública. 2006; 22:1901-7. [ Links ]
18. Ayres JR. Epidemiologia, promoção da saúde e o paradoxo do risco. Rev Bras Epidemiol. 2001; 5:28-42. [ Links ]
19. Burt BA. Concepts of risk in dental public health. Community Dent Oral Epidemiol. 2005; 33:240- 7. [ Links ]
20. Jamieson LM, Thomson KFR, Sayers SM. Dental caries risk indicators among Australian aboriginal young adults. Community Dent Oral Epidemiol. 2010; 38:213–21.
21. Terreri AL, Soler ZA. Estudo comparativo de dois critérios utilizados no Programa Saúde da Família na priorização do tratamento da cárie entre crianças de 5 a 12 anos. Cad Saúde Pública. 2008; 24:1581-7. [ Links ]
22. Oakley C, Brunette DM. The use of diagnostic data in clinical dental practice. Dent Clin North Am. 2002; 46:87-115. [ Links ]
23. Góes PS, Fernandes LM, Lucena LB. Validação de instrumentos de coleta de dados. In: Antunes JL, Peres MA. Fundamentos de odontologia: epidemiologia da saúde bucal. Rio de Janeiro: Guanabara Koogan; 2006. p.390-7. [ Links ]
24. Ware JE, Brook RH, Davies AR, Lohr KN. Choosing measures of health status for individuals in general populations. Am J Public Health. 1981; 71:620-5. [ Links ]
25. Assaf AV, Meneghim MC, Zanin L, Mialhe FL, Pereira AC, Ambrosano GM. Classification of different methods for diagnosing dental caries in epidemiological surveys. Community Dent Oral Epidemiol. 2004; 32:418-25. [ Links ]
26. Kassawara AB, Assaf AV, Meneghim MC, Pereira AC, Topping G, Levin K, et al. Comparison of epidemiological evaluations under different caries diagnostic thresholds. Oral Health Prev Dent. 2007; 5:137-44. [ Links ]
27. Bader JD, Shugars DA, Bonito AJ. Systematic reviews of selected dental caries diagnostic and management methods. J Dent Educ. 2001; 65:960-8. [ Links ]
28. Bader JD, Shugars DA, Bonito AJ. A systematic review of the performance of methods for indentifying carious lesions. J Public Health Dent. 2002; 62:201-13. [ Links ]
29. Zaroni WCS, Ciccone JC, Gabriel AES, Ramos SA, Dibb RGP. Validity and reproducibility of different combinations of methods for occlusal caries detection: a vitro comparison. Caries Res. 2006; 40:194-201. [ Links ]
30. Assaf AV, Meneghim MC, Zanin L, Cortelazzi KL, Pereira AC, Ambrosano GM. Effect of different diagnostic thresholds on dental caries calibration. J Public Health Dent. 2006; 66:17-22. [ Links ]
 Autor correspondente:
Autor correspondente:
Henri Menezes Kobayashi
Faculdade de Odontologia de Piracicaba/FOP-UNICAMP
Av. Limeira 901, Areião
CEP: 13414-903 – Piracicaba – SP – Brasil
e-mail:henrimenezeskobayashi@yahoo.com
Recebido em 13/02/2012 – Aceito em 26/05/2012
