










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.17 no.33 Canoas Jul./Dez. 2011
SCIENTIFIC ARTICLE
Apical root resorption of maxillary first molars related to headgear use as detected by cone beam computed tomography
Reabsorção radicular apical dos primeiros molares superiores decorrente do uso de aparelho extraoral, diagnosticada na tomografia computadorizada cone beam
Jairo Curado de Freitas1; Olavo César Porto Lyra1; Ana Helena Gonçalves de Alencar1; Carlos Estrela1
1Dentistry School, Universidade Federal de Goiás (UFG), Goiânia, GO, Brazil.
ABSTRACT
Extraoral traction (EOT) by occipital headgear is a widely used anchorage and orthopedic approach for the control of maxillary growth. The aims of this study were: 1) to test the hypothesis that headgear use may increase the risk of apical root resorption, using cone beam computed tomography (CBCT) to detect root resorptions of maxillary first molars, and 2) to assess which roots are more prone to resorption and to which extent. A total of 112 maxillary first molars from 56 patients at 52 to 288 months after orthodontic treatment were evaluated to detect apical root resorption on CBCT images. Patients were divided into two groups: Group 1, patients who used EOT for up to six months; Group 2, patients who did not use EOT. The Levander and Malmgren scoring system was used to classify the root apices of maxillary first molars. Significance was set at 5%. Kappa statistics was used to assess agreement; scores were evaluated twice, according to the study methods. There were no differences in the frequency and severity of apical root resorption of maxillary first permanent molars in the two groups as detected by CBCT. The use of EOT did not show association with frequency and severity of ARR considering a long time of follow up.
Keywords: Extraoral traction; root resorption; cone beam computed tomography; orthodontic treatment.
RESUMO
A Tração extraoral (EOT) com puxada cervical é um tipo de ancoragem com abordagem ortopédica amplamente utilizada para o controlo do crescimento maxilar. Os objetivos deste estudo foram: 1) testar a hipótese de que o uso de tração extraoral pode aumentar o risco de reabsorção radicular apical, usando tomografia computadorizada cone beam (TCFC), para detectar reabsorções radiculares dos primeiros molares, e 2) avaliar quais as raízes mais propensas à reabsorção e em que extensão. Um total de 112 primeiros molares superiores, de 56 pacientes, com 52 a 288 meses pós-tratamento ortodôntico, foram avaliados para detectar a reabsorção radicular apical em imagens TCFC. Os pacientes foram divididos em dois grupos: Grupo 1, pacientes com uso de EOT por período superior a seis meses; Grupo 2, pacientes que não usaram EOT. O sistema Levander e Malmgren foi usado para classificar os ápices dos primeiros molares superiores. As análises foram realizadas duas vezes, sendo utilizado o índice Kappa, ao nível de significância de 5%. Os resultados mostraram que não houve diferença na freqüência e gravidade da reabsorção radicular apical dos primeiros molares permanentes superiores entre os dois grupos, detectadas por CBCT. O uso de EOT não mostrou associação com a freqüência e a gravidade das reabsorções radiculares apicais, considerando o período avaliado.
Palavras-chave: Tração extraoral; reabsorção radicular; tomografia computadorizada cone beam; tratamento ortodôntico.
INTRODUCTION
Extraoral traction (EOT) by occipital headgear is a widely used anchorage and orthopedic approach for the control of maxillary growth. Daily and/or night-time use of EOT for anchorage may cause jiggling, rotational, and extrusional forces1. A previous study employing finite element analysis has shown that the stress pattern in the periodontal ligament for a distalizing force without counterbalancing moments shows a high concentration at the cervical level of the distobuccal root due to tipping and rotation of the tooth2.
Little attention has been paid to the possibility of apical root resorption (ARR) of posterior teeth. This can be explained by the strong evidence suggesting resorption in the anterior region and also by the technical difficulty associated with detecting resorption in molars. Notwithstanding, the latter teeth also appear to be vulnerable to mechanotherapy. The variable amount of root resorption observed in molars via cone beam computed tomography (CBCT) resulting from the use of extraoral appliances, e.g. those employed during mechanotherapy in Class II malocclusions, has been little discussed in the literature3.
ARR has been frequently detected and followed with conventional radiography4-6. Promising developments in the diagnosis of lesions affecting the tooth surface and the periapical area, e.g. CBCT, have allowed to more closely follow and predict the evolution of these abnormalities7-12.
There is a shortage of studies on root resorption of first molars in general and on the use of CBCT to detect resorption in particular. Therefore, the aims of the present study were: 1) to test the hypothesis that headgear use may increase the risk of ARR of maxillary first molar teeth, using CBCT as the diagnostic method; and 2) to assess which roots are more prone to resorption and to which extent (level). The null hypothesis was that there would be no differences in the frequency and severity of ARRs detected by CBCT in patients who used EOT when compared with patients who did not use EOT.
METHODOLOGY
Sample
This study evaluated 112 maxillary first molars showing ARR on CBCT 52 to 288 months after orthodontic treatment. Fifty-six patients (26 males and 30 females) were selected through a database search at a private orthodontic clinic in Goiânia, GO, Brazil. Patients were divided into two groups: Group 1, n=28, patients who used EOT for up to six months; Group 2, n=28, patients who did not use EOT.
Inclusion criteria were: availability of CBCT images, orthodontic records, radiographs, pictures, and plaster models; orthodontic treatment completion at least 52 months before. None of the patients had a history of retreatment. All patients had been treated by the same orthodontist using standard edgewise appliances (0.022x0.028). The study was approved by the local Research Ethics Committee (UFG, protocol no. 169/2008).
Imaging method
CBCT images were acquired with a first generation i-CAT cone-beam 3D imaging system (Imaging Sciences International, Hatfi eld, PA, USA). Volumes were reconstructed using a 0.2 x 0.2 x 0.2 mm voxel size. The tube voltage was 120 kVp, and the current, 3.8 mA. Exposure time was 40 seconds. Images were examined using the scanners proprietary software (Xoran 3.1.62; Xoran Technologies, Ann Arbor, MI, USA) on a PC workstation running Microsoft Windows XP professional SP-2 (Microsoft Corp., Redmond, WA, USA), Intel® CoreTM 2 Duo-6300 1.86 GHz (Intel Corporation, Santa Clara, CA, USA), NVIDIA GeForce 6200 with turbocache videocard (NVIDIA Corporation, Santa Clara, CA, USA), and an EIZO - Flexscan S2000 monitor at a resolution of 1600 x 1200 pixels (EIZO NANAO Corporation Hakusan, Ishikawa, Japan). The tools available on the software allowed to evaluate each tooth in three dimensions.
Evaluation methods
CBCT images were evaluated by an orthodontist and a radiology specialist with 5 years of training until a consensus was reached. The examiners were blind to the use of EOT. For the assessment of intra-examiner reliability, 20% of the sample was evaluated twice at a 15-day interval. Analysis of the apical region of the right and left first molars was performed dynamically, in different planes (axial and cross-sectional). Slice thickness varied between 1 and 1.5mm.
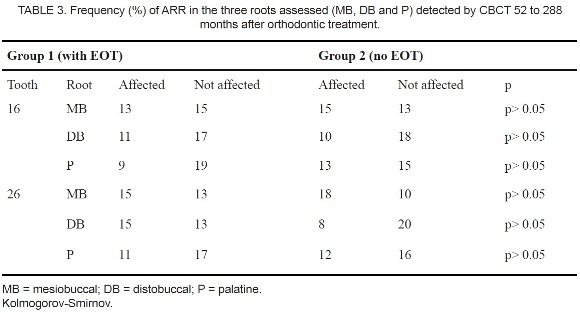
In Group 1, EOT was applied to first molars using several force levels, at an average of 300g on each side. Root apices were named mesiobuccal (MB), distobuccal (DB), and palatine (P). The number of teeth and root apices presenting and not presenting ARR was recorded.
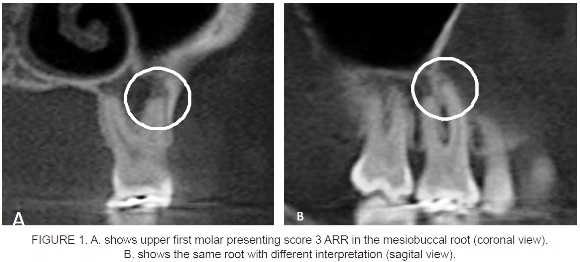
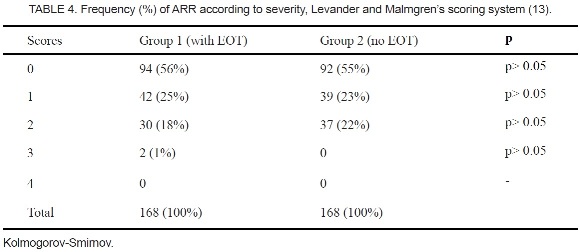
The Levander and Malmgren13 scoring system was used to classify the root apices of maxillary first molars. ARR was graded as follows: 0, no root resorption; 1, irregular root contour; 2, ARR< 2mm; 3, ARR from 2mm to one third of the original root length; and 4, ARR exceeding one third of the original root length.
The Kolmogorov-Smirnov and chi-square tests were used to evaluate the data. Significance was set at 5%. Kappa statistics was used to assess agreement; scores were, according to the study methods.
RESULTS
Significant agreement was obtained between the observations made in two phases (Kappa test = 0.631).
ARR results are presented in (Tables 1 to 4). At the beginning of the orthodontic treatment, mean age was 12 years (SD: 1.6) in Group 1 (with EOT) and 12 years (SD: 1.7) in Group 2 (no EOT). Each group included 13 males and 15 females. Mean time elapsed between orthodontic treatment completion and CBCT image acquisition was 179 months (SD: 70 months) in Group 1 and 123 months (SD: 47 months) in Group 2.
(Figure 1) shows a maxillary first molar presenting score 3 ARR in the mesiobuccal root in coronal view and the same root with different interpretation in sagittal view.
DISCUSSION
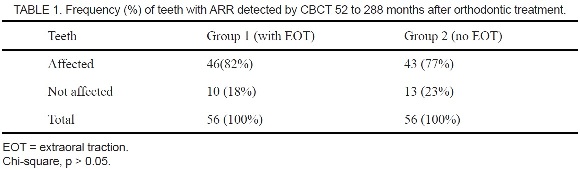
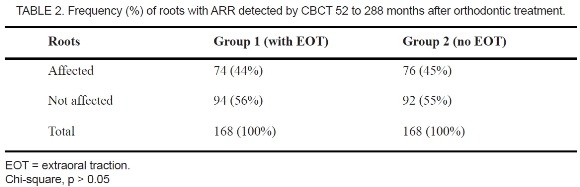
New scientific parameters have been introduced in orthodontics with the advent of CBCT technology. The possibility to identify ARR in all roots of molars was an expressive diagnostic improvement. One hundred and sixty eight roots received forces using EOT. The results of the present study suggested that the use of EOT is not associated with the number of teeth or roots affected by resorption (Tables 1 to 2).
Comparing pre and post-treatment orthopantomograms of 97 patients, MacNab et al.14 reported that the incidence of ARR was positively associated with tooth position, type of appliance used, tooth extraction, and use of headgear. Alwaliu et al.1 radiographically evaluated night-time use of EOT in 21 patients selected for orthodontic treatment. Those patients used a full fixed appliance as anchorage system for at least 6 months. The experimental group in the study by Alwaliu et al. comprised 11 patients and was treated with reinforcement anchorage in the maxilla with EOT (cervical pull) at night. The other 10 patients (control group) were treated with anchorage by either a Goshgarian palatal bar or Class II elastics. Standardized periapical radiographs of the maxillary first molars were taken at the start of treatment, and after 3 and 6 months. Data recording also included patient compliance, force evaluation and the measurement of tooth movement. Significant reduction in root length was observed for some roots already after 3 months. However, mean root resorption after 6 months did not exceed 0.6 millimeter in any maxillary first molar root of those authors sample1. The degree of root resorption was similar in the experimental and control groups assessed by Alwaliu et al. The authors concluded that patients treated with night-time anchorage by EOT will show similar degrees of root resorption of maxillary molars as those treated with a Goshgarian bar or Class II elastics1.
In the present study, the level of ARR observed with the use of EOT was assessed using the Levander and Malmgren13 scoring system. The results revealed absence of significant differences in all severity scores. Although first molars tend to present a high frequency of ARR, the severity of the condition is similar in posterior and anterior teeth11.
Jeon et al.2, using a finite element model, found a high concentration of stress at the cervical level of distobuccal roots after application of distalizing forces without counterbalancing movements. Conversely, when counterrotation and countertipping moments were applied, an even distribution of low compression on the distal side of the periodontal ligament was obtained. Furthermore, high stress concentration was observed on the root surface at the furcation level, in contrast with anterior teeth, reported to display high concentration at the apex. This result may suggest that the morphology of maxillary first molars makes them less susceptible to ARR during tooth movement. Siqueira et al.3 have assessed the effect of occipital headgear use on the intensity of ARR of maxillary first permanent molars. Periapical radiographs of 19 young females aged 8 to 10 years, with dental Class II division 1 malocclusion, were evaluated before and after orthodontic treatment. Those authors concluded that headgear use did not negatively influence root formation and did not provoke apical resorption of the molars submitted to traction. Their findings therefore suggest that the use of headgear does not pose risks to root structure and formation when correctly indicated and applied.
Experimental models using periapical or panoramic radiographs to measure ARR associated with orthodontic movement have reported different results when compared with ARR measurement in CBCT images11, 12.
Dudic et al.12 have compared ARR in 275 teeth of 22 orthodontic patients assessed with panoramic radiography vs. CBCT using the scoring system developed by Levander and Malmgren13. They found significant differences between the two methods for all levels of severity of ARR. Panoramic radiography underestimated ARR after orthodontic treatment. CBCT should be used to help monitor patients at risk for developing severe root resorption during orthodontic movement. Our results were similar to those reported by Dudic et al.12, but we evaluated ARR after a long-term follow-up of orthodontic treatment using CBCT.
Freitas et al.11 reported differences between CBCT and periapical radiography when comparing the frequencies of ARR. Differences were significant for both maxillary/ mandibular premolars and mandibular molars. In these teeth, a greater presence of ARR was detected by periapical radiography. These results suggest that periapical radiography, due to its limitations, tends to overestimate the severity of ARR in posterior tooth groups. This may be explained by the tooth group analysis adopted by the authors. When comparing different tooth groups, factors such as apical morphological variations, surrounding bone density (thick or thin cortical bone), X-ray angulations, radiographic contrast, and overlapping anatomic structures may affect radiographic interpretations. In our study, the estimations of frequencies of EOT-related ARR, particularly in the roots of molars as detected by CBCT, were not influenced by the limitations observed when using periapical radiography.
It is expected that the development of new tools with a potential to assist in diagnosis, such as CBCT, will bring new challenges for dental professionals before we can reach a complete understanding of the properties and limitations of such new technologies. The possibility to assess all surfaces of teeth and adjacent structures with a reliable imaging method has been addressed in several studies7,8,9-12,15.
CONCLUSION
There were no differences in the frequency and severity of ARR of maxillary first permanent molars treated or not with EOT, as detected by CBCT.
REFERENCES
1. Alwaliu S, Marklund M, Persson M. Apical root resorption of upper first molars as related to anchorage system. Swed Dent J. 2000;24:145-53. [ Links ]
2. Jeon PD, Turley PK, Moon HB, Jeon K. Analysis of stress in the periodontium of the maxillary first molar with a three-dimensional finite element model. Am J Orthod Dentof Orthop.1999;115:267-74. [ Links ]
3. Siqueira VCV, Gameiro GH, Magnani MBBA, Sousa MA, Carvalho AZNB. Estudo comparativo da reabsorção radicular apical após o uso de aparelho extrabucal no tratamento da má oclusão do tipo Classe II, 1ª divisão dentária. Rev Dent Press Ortodon Ortop Facial. 2009;14:54-62.
4. Bender IB. Factors influencing the radiographic appearance of bone lesions. J Endod. 1982;8:161-70. [ Links ]
5. Laux M, Abbott PV, Pajarola G, Nair PNR. Apical infl ammatory root resorption: a correlative radiographic and histological assessment. Int Endod J. 2000;33:483-93. [ Links ]
6. Huumonen S, Ørstavik D. Radiological aspects of apical periodontitis. Endod Topics. 2002;1:3-25. [ Links ]
7. Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999;28:245-8. [ Links ]
8. Mozzo P, Procacci C, Taccoci A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol. 1998;8:1558-64. [ Links ]
9. Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008;34:273-9. [ Links ]
10. Estrela C, Bueno MR, Alencar AH, Mattar R, Valladares Neto J, Azevedo BC, De Araújo Estrela CR. Method to evaluate inflammatory root resorption by using cone beam computed tomography. J Endod. 2009;35:1491-7. [ Links ]
11. Freitas JC, Estrela C, Alencar AHG. Long-term evaluation of apical root resorption after orthodontic treatment using periapical radiography and cone beam computed tomography. Dent Press J Orthod. 2011. In press. [ Links ]
12. Dudic A, Giannopoulou C, Leuzinger M, Kiliaridis S. Detection of apical root resorption after orthodontic treatment by using panoramic radiography and conebeam computed tomography of super-high resolution. Am J Orthod Dentofac Orthop. 2009;135:434-7. [ Links ]
13. Levander E, Malmgren O. Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988;10:30-8. [ Links ]
14. McNab S, Symons AL, Battistutta D, Taverne A. External apical root resorption following orthodontic treatment. Angle Orthod. 2000;70:227-32. [ Links ]
15. Estrela C, Bueno MR, Porto OCL, Rodrigues CD, Pécora JD. Influence of intracanal post on apical periodontitis identified by cone beam computed tomography. Braz Dent J. 2009;20:370-5. [ Links ]
 Corresponding Author:
Corresponding Author:
Prof. Jairo Curado Freitas
Department of Stomatologic Sciences.
Universidade Federal de Goiás
Praça Universitária s/n, Setor Universitário
CEP 74605-220, Goiânia, GO, Brazil
E-mail: curadojf@terra.com.br
ACKNOWLEDGMENTS
This study was partly supported by grants from the National Council for Scientific and Technological Development (CNPq grant no. 302875/2008-5 and CNPq grant no. 474642/2009 to C.E.).
