










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.17 no.33 Canoas Jul./Dez. 2011
SCIENTIFIC ARTICLE
Porcelain laminate veneers: A minimally invasive esthetic procedure
Laminados cerâmicos: um procedimento estético minimamente invasivo
Rafael de Almeida Decurcio1; Paula de Carvalho Cardoso2
1MSc in Oral Rehabilitation – UFU, GO, Brazil. Professor of Specialization Course
in Operative Dentistry, UniABO, Goiânia, GO, Brazil.
2PhD in Restorative Dentistry – UFSC, SC, Brazil. Professor of Specialization Course
in Operative Dentistry, UniABO, Goiânia, GO, Brazil. ProDoc grantee, Faculty of Dentistry - UFGO, GO, Brazil.
ABSTRACT
Technological advances in materials and techniques have been allowing to obtain natural esthetic results with conservative interventions. Ceramic veneers are very effective tools for both esthetic and functional rehabilitation. This study describes the use of ceramic veneers without tooth wear, reinforcing the concept that minimally invasive porcelain laminate veneers could become versatile and conservative allies in the field of esthetic dentistry.
Keywords: Ceramics, dentin-bonding agents, esthetics.
RESUMO
O avanço tecnológico de materiais e técnicas tem proporcionado resultados estéticos cada vez mais naturais com intervenções conservadoras. As facetas cerâmicas se solidificaram como uma das ferramentas mais eficazes na reabilitação estética e funcional. Este artigo tem como objetivo descrever o uso de facetas cerâmicas sem a realização de desgaste dental, sedimentando o conceito de que os laminados cerâmicos minimamente invasivos podem tornar-se um aliado extremamente versátil e conservador na área da estética odontológica.
Palavras-chave: Cerâmica, adesivos dentinários, estética.
INTRODUCTION
The incessant search for beauty has motivated important advances in the physical and optical properties of dental materials1. Such advances have enabled the development of more conservative techniques and increased the chances of obtaining more predictable esthetic results. Considering the particularities of each technique, ceramic has been used due to its biocompatibility, longevity and resemblance with the natural appearance of teeth2.
The ceramic systems currently available have important esthetic qualities and great resistance, once they are reinforced with leucite and lithium disilicate3. These properties allow the performance of minimally invasive procedures with porcelain laminate veneers. In the tooth veneering technique, thin porcelain laminates (0.1 to 0.7 mm thick) are applied to the dental structure with minimal or no dental reduction/wear4,5. Porcelain veneers replace the visible portion of enamel, and they are strongly bonded to the dental surface6.
Tooth veneering was first recommended by Christensen 7 and Quinn et al.8. However, some subsequent studies have revealed limitations such as overcontour9 and fractures10,11. As a result of the thin thickness of veneers, the color of the underlying dental substrate can also affect the final result. Jorgenson and Goodkind12 and Volpato et al.13 have reported that the correct selection of a ceramic system involves the assessment of the color of the dental substrate, of the thickness of ceramic materials available, as well as of the degree of translucency and/or opacity of the veneers. In order to neutralize the influence of the dental substrate, the practitioner can use bleaching techniques prior to treatment or use a variety of colors of composite cements14 to optimize biomimetics.
The objective of this paper was to describe the case of a patient treated with porcelain laminate veneers, with an emphasis on the possibility of using veneers without significant dental wear/reduction.
CASE REPORT
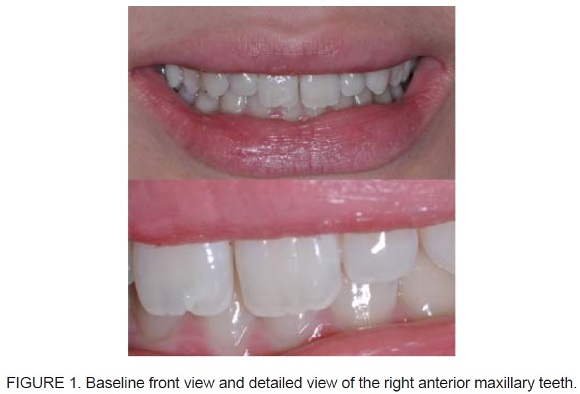
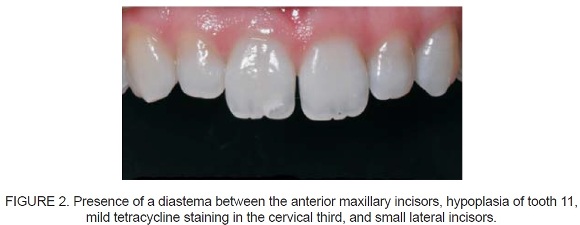
A 20 year-old female patient sought our dental service reporting dissatisfaction with the appearance of her smile (Figure 1). Anamnesis, clinical examination and intraoral photographs revealed a small diastema between the maxillary central incisors, small lateral incisors, and light cervical staining caused by tetracycline (Figure 2).
A treatment plan was devised to restore the appearance of the patient’s smile, with dental bleaching and preparation/installation of porcelain laminate veneers on the anterior affected teeth (teeth 13 to 23).
A combined in-office and take-home bleaching technique was adopted. Initially, in-office bleaching was carried out by applying 35% hydrogen peroxide gel (Opalescence Xtra Boost, Ultradent, USA), on the buccal surface of teeth in both the maxillary and mandibular arches. This bleaching session lasted for 45 minutes.
The bleaching gel used at the office is comprised of two syringes, one containing hydrogen peroxide and the other containing the activator. Following manufacturer’s instructions, both bleaching gels were mixed syringe-to-syringe 50 times. Following preparation, the mixture was applied to the tooth surfaces using a tip, without lightcuring.
The in-office bleaching session was complemented with a take-home bleaching system consisting of application of 15% carbamide peroxide gel (Opalescence 15% PF, Ultradent, USA) for 2 hours a day, over 16 days.
Addition silicone impressions (Elite, Zermack, Italy) were taken one week after bleaching. A double-cord technique was used for deflection of the soft tissues, using 0 and 00 cords (Ultrapak, Ultradent, South Jordan, USA). The 0 cord was removed from the gingival sulcus, and the 00 cord remained in place during impression.
Silicone impressions of the maxillary and mandibular arches, bite registration and diagnostic wax-up data were sent to the prosthetic laboratory along with the work order, which contained the following information: patient’s chief complaint, color map, shade selection, dental substrate shade, porcelain system selection and additional information about color and contours. Clinical baseline photographs of the teeth were also sent to the dental laboratory.
After 15 days, the porcelain laminate veneers fabricated using the IPS Empress Esthetic Ingots (Ivoclar Vivadent, Amherst, USA) ceramic system were applied to the teeth using a try-in paste (Variolink Veneer Try-in, Ivoclar Vivadent, Amherst, USA) that simulates the fi nal shade of restorations.
The adhesive cementation of ceramic veneers is an irreversible process. Therefore, ensuring an accurate fit of the final restoration is extremely important, once it determines the final esthetic result. Also, while working with veneers, it is important to keep in mind that the cement shade may change the final restoration color, due to the thin thickness of veneers. The try-in paste used in our patient is available in seven shades and three degrees of translucency. In order to maximize optical results, the system also offers three different intensity shades for try-in high values and try-in low values.
Porcelain laminate veneers were positioned using an appropriate applicator (Vivastick, Ivoclar Vivadent, Amherst, USA). A small amount of paste was applied on the restoration and carefully set on the tooth remnant, without pressure. Excess material was removed and the final shade was analyzed.
After completion of the try-in stage and determination of the cement color, the internal areas of the veneers were etched with 4% hydrofluoric acid for 60 seconds, rinsed thoroughly with water and air dried. The Relyx silane-based ceramic primer (3M ESPE, St. Paul, USA) was then applied to the inner surfaces of the restorations for 60 seconds. Subsequently, the surfaces were dried using oil/moisture-free air for 5 seconds, and the Scotchbond Multi Purpose Plus adhesive system (3M ESPE, St. Paul, USA) was applied to the internal areas of the veneers.
Prophylaxis was performed using pumice paste and a rubber cup, prior to veneer placement. Then, 00 compression cords (Ultrapak, Ultradent, South Jordan, USA) were inserted at the bottom of the sulcus around each tooth, and the adjacent teeth were coated with polytetrafluoroethylene.
Before luting, 37% phosphoric acid was applied to the surface of the prepared tooth and allowed to react for 30 seconds. Thorough rinsing of the surface with water for 60 seconds was followed by application of the primer and bonding agents (Scotchbond Multi Purpose System, 3M ESPE, St. Paul, USA).
Luting procedures were performed individually, as follows: hybridization, lightcuring for 20 seconds, and removal of excess material to minimize the risk of laminate fracture. Resin cements were light-cured for 60 seconds (XL 3000, 3M/ESPE, St. Paul, USA), at a light output of 700 mW/cm2.
Tooth 11 was cemented using a medium value light-curing composite cement (Medium Value, Variolink Veneer, Ivoclar, Vivadent, Amherst, USA). A high value lightcuring composite cement (+3 High Value, Variolink Veneer, Ivoclar, Vivadent, Amherst, USA) was used in tooth 21.
The final aspect of restorations is shown in (Figures 3 and 4). Porcelain laminate veneers allowed to successfully restore dental function and esthetics, resulting in a natural and esthetically pleasing smile.


DISCUSSION
Tooth veneering is a minimally invasive procedure that enables the practitioner to apply biomimetic principles in cosmetic dentistry, finding a balance between ceramic and enamel. The great majority of restorative procedures violates the balance between enamel and dentin in natural teeth. Unlike these procedures, the use of porcelain laminate veneers offers an excellent combination of hardness, resistance, and resilience 15. According with Magne and Belser 16, a tooth restored with a porcelain laminate veneer that is subjected to posterior-anterior force recovers 89 to 96% of its coronary stiffness when compared with a healthy tooth.
Diagnostic wax-up mock-up techniques are great tools during clinical evaluation and treatment planning, once they provide information on the possibility of using porcelain laminate veneers with minimal or no dental wear. That said, establishing a treatment plan using diagnostic wax-ups is utterly necessary to determine the exact final position and anatomy of the veneer. This preview is the safest way to evaluate the real need to perform dental wear.
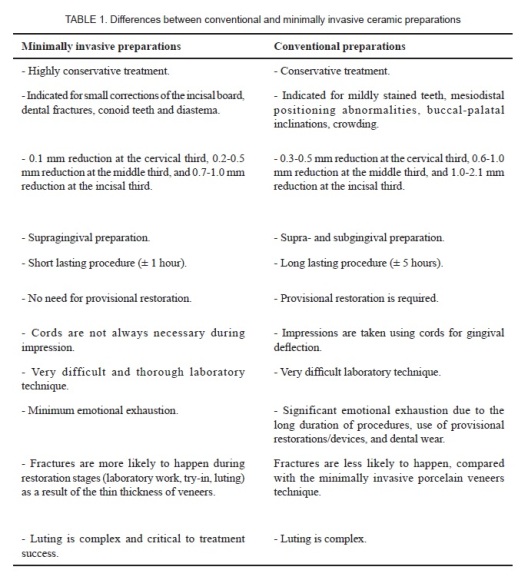
(Tables 1) shows the differences between conventional and minimally invasive ceramic preparations, based on adhesive techniques and tooth structure preservation principles.
The IPS Empress Esthetic ceramic system used in our case contains leucite crystals dispersed in a glass matrix, forming a homogeneous interlocking structure that prevents internal crack propagation17. The composition and injection molding mechanism of this system provide an increase in flexural strength and fracture resistance when compared with the conventional ceramic system. These characteristics contribute to an easier and faster execution of the clinical and laboratory steps involved in restoration. They also enable the production of very thin veneers, further reinforcing the minimally invasive aspect of the technique.
Clinical factors such as remnant/substrate color, laminate thickness and luting system are known to potentially interfere with the final esthetic result. That said, the professional may resort to clinical interventions prior to optimizing esthetic results, as well as promote the use of minimally invasive or conservative techniques.
Conversely, the following variables have been associated with optimal and predictable results: dental/remnant bleaching prior to veneer application, use of opaque ceramic systems, careful selection of the most appropriate luting system and of adequate shades/colors, try-in stage using appropriate pastes, use of hydrosoluble gel or water prior to final luting with composite cements.
FINAL CONSIDERATIONS
The minimally invasive, conservative porcelain laminate veneer technique here described is an extremely versatile clinical procedure, with excellent esthetic results when performed according to a well-designed treatment plan and a strict protocol during the clinical and laboratory stages.
REFERENCES
1. Goldstein RE. Study of need for esthetic in dentistry. J Prosthet Dent. 1969;21(6): 589-98. [ Links ]
2. Kelly JR, Nishimura I, Campbell SD. Ceramic in dentistry: history and historical roots and current perspectives. J Prosthet Dent. 1996;75(1):18-32. [ Links ]
3. Anusavice KJ. Cerâmicas odontológicas. In: Anusavice KJ. Philips materiais dentários. 11ª ed. Rio de Janeiro: Elsevier; 2005. p. 619-77. [ Links ]
4. Baratieri LN, Guimarães J. Laminados cerâmicos. In: Baratieri LN. Soluções clínicas: fundamentos e técnicas. Florianópolis: Ponto; 2008. p. 214-271. [ Links ]
5. Kina S, Brugrera A. Invisível: restaurações estéticas cerâmicas. Maringá: Dental Press; 2007. [ Links ]
6. Horn HR. Porcelain laminate veneers bonded to etched enamel. Dent Clin North Am. 1983;27(4):671-84. [ Links ]
7. Christensen GJ. Veneering of teeth. State of the art. Dent Clin North Am. 1985;29(2):373-91. [ Links ]
8. Quinn F, McConnell RJ, Byrne D. Porcelain laminates: a review. Br Dent J. 1986;161(2):61-5. [ Links ]
9. Hahn P, Gustav M, Hellwig E. An in vitro assessment of the strength on porcelain veneers dependent on tooth preparation. J Oral Rehabil. 2000;27(12):1024-9. [ Links ]
10. Brunton PA, Wilson NH. Preparations for porcelain laminate veneers in general dental practice. Br Dent J. 1998;184(11):553-6. [ Links ]
11. Shaini FJ, Shortall AC, Marquis PM. Clinical performance of porcelain laminate veneers. A retrospective evaluation over a period of 6.5 years. J Oral Rehabil. 1997;24(8):553- 9. [ Links ]
12. Jorgenson MW, Goodkind RJ. Spectrophotometric study of five porcelain shades relative to the dimensions of color, porcelain thickness, and repeated firings. J Prosthet Dent. 1979;42(1):96-105. [ Links ]
13. Volpato CA, Monteiro S Jr, de Andrada MC, Fredel MC, Petter CO. Optical influence of the type of illuminant, substrates and thickness of ceramic materials. Dent Mater. 2009;25(1):87-93.
14. Rezende MO, Cardoso PC, Rodrigues MB, Porfi rio W. Laminados cerâmicos minimamente invasivos. Clin Int J Braz Dent. 2009;5(2):182-92. [ Links ]
15. Magne P, Belser U. Estética dental natural. Restaurações adesivas de porcelana na dentição anterior: uma abordagem biomimética. São Paulo: Santos; 2003. [ Links ]
16. Magne P, Douglas WH. Additive contour of porcelain veneers: a key element in enamel preservation adhesion, and esthetics for aging dentition. J Adhes Dent. 1999;1(1):81-92. [ Links ]
17. Fradeani M, Redemagni M, Corrado M. Porcelain laminate veneers: 6-to 12-year clinical evaluation-a retrospective study. Int J Periodontics Restorative Dent. 2005;25(1):9-17. [ Links ]
 Corresponding Author:
Corresponding Author:
Rafael Almeida Decurcio
Associação Brasileira de Odontologia, Seção de Goiás
Departamento de Dentística
Av. Itália, 1184, Jardim Europa
CEP 74325-110 - Goiânia, GO – Brazil
Tel.: +55 (62) 3236.3116 / 7814.1178
E-mail: rafaeldecurcio@gmail.com
