










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.17 no.33 Canoas Jul./Dez. 2011
SCIENTIFIC ARTICLE
Intra-sinusal third molar: Case report
Terceiro molar intrassinusal: relato de caso
Frederico Sampaio Neves1; Laura Ricardina Ramírez-Sotelo1; Matheus Lima de Oliveira1; Gina Roque-Torres2; Thais de Camargo Souza3; Deborah Queiroz de Freitas4
1PhD Student in Dental Radiology, Faculty of Dentistry – UNICAMP.
2MSC Student in Dental Radiology, Faculty of Dentistry – UNICAMP.
3Student in Faculty of Dentistry – UNICAMP.
4PhD in Dental Radiology, Faculty of Dentistry – UNICAMP.
ABSTRACT
Ectopic tooth eruption into an area other than the oral cavity is rare. Nasal septum, mandibular condyle, coronoid process and infratemporal fossa space have been reported as frequent locations for ectopic tooth eruption. Ectopic teeth located within the maxillary sinus may be asymptomatic, found only in routine examinations. Headache, sinusitis and nasal obstruction are some of the associated symptoms. The differential diagnosis includes foreign bodies (rhinolith), infections (syphilis and tuberculosis), benign lesions (hemangioma, osteoma, calcified polyp) and malign lesions (osteosarcoma). Upper third molars located within the maxillary sinus may be associated with the development of mucocele or dentigerous cyst. The aim of this paper was to describe the case of a 24-year old female patient with an ectopic right upper third molar in the maxillary sinus. A hyperdense area was observed with sinus obliteration, consistent with mucous material.
Keywords: Third molar, maxillary sinus, pathology.
RESUMO
Erupção ectópica dos dentes em outras regiões além da cavidade oral é rara. O desenvolvimento ectópico desses dentes tem sido relatado no septo nasal, côndilo mandibular, processo coronoide e no espaço da fossa infratemporal. Dentes ectópicos localizados no seio maxilar podem ser assintomáticos, descobertos em exames radiográficos de rotina. Dentre os sintomas associados estão cefaleia, sinusite e obstrução nasal. Corpos estranhos (rinólitos), processos infecciosos (sífilis ou tuberculose), lesões benignas (hemangioma, osteoma, pólipos calcificados) e malignas (osteossarcoma) podem ser considerados no diagnóstico diferencial de dentes ectópicos. Os terceiros molares superiores, quando localizados no seio maxilar, podem estar associados ao desenvolvimento de mucocele, assim como de cistos dentígeros. Dessa forma, o objetivo deste artigo foi relatar o caso de uma paciente do gênero feminino, com 24 anos de idade, em que se observou terceiro molar superior direito com localização intrassinusal associado a uma área de hiperdensidade média, causando parcial obliteração do seio maxilar, compatível com material mucoide.
Palavras-chave: Terceiro molar, seio maxilar, patologia.
INTRODUCTION
Ectopic eruption of a tooth into an area other than the oral cavity is rare. The development of ectopic teeth has been reported in the nasal septum1, mandibular condyle2, coronoid process3, and infratemporal fossa4. Ectopic tooth eruption may be associated with one of the following factors: development disorders, pathologies, and iatrogenic procedures5. The aim of this paper was to describe the radiographic and tomographic aspects of a rare intra-sinusal third molar.
CASE REPORT
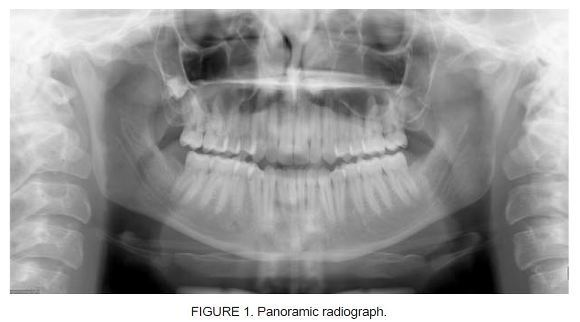
A 24-year old female patient was seen at the radiology clinic at the Piracicaba Dental School for preoperative radiographic evaluation of third molars. The patient reported no pain or any abnormality. No abnormality was observed during intraoral and extraoral examinations. Panoramic radiograph revealed superimposition of the right upper third molar and the maxillary sinus (Figure 1). The tooth presented a complete crown and incomplete root formation.
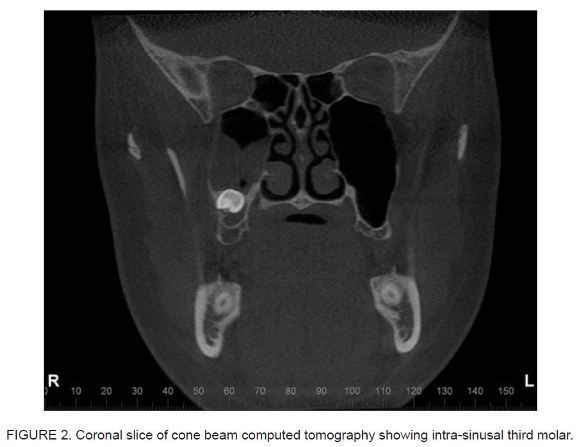
Cone beam computed tomography scans (i-CAT, Imaging Sciences International, Inc, Hatfield, PA, USA) were taken for a better evaluation. The unit was set at 120 kVp, 8 mA, a voxel size of 0.25 mm, and a field of view of 8 cm. On the coronal (Figure 2) and sagittal (Figure 3) sections, the right upper third molar was observed within the maxillary sinus in a distoangular position. A hyperdense area was observed, with partial sinus obliteration, consistent with mucous material. Radiographic follow-up was recommended due to the absence of symptoms.

DISCUSSION
Ectopic teeth located within the maxillary sinus may be asymptomatic. In such cases, they are only found in routine examinations. Headache, sinusitis and nasal obstruction are some of the associated symptoms6. Teeth located in the mandible are usually asymptomatic7, and may be associated with dentigerous cysts6,8. When symptomatic, periauricular pain and swelling in the parotid area are described9,10. This symptomatology is mostly related to infected cysts.
Computed tomography is the most appropriate method to visualize impacted teeth. It shows the relationship between teeth and adjacent structures with high-quality sectional images. Cone beam computed tomography has become a widespread imaging method in dentistry, since it provides clear images of highly contrasted structures using less radiation than traditional fan beam computed tomography systems11. In the present study, tomographic images were of great importance for the diagnosis of the intra-sinusal third molar.
The differential diagnosis of ectopic teeth in the maxillary sinus includes foreign bodies (rhinolith), infections (syphilis and tuberculosis), benign lesions (hemangioma, osteoma, calcified polyp), and malign lesions (osteosarcoma)12. In the evaluation of computed tomography images, similarity of tooth density and morphology is significant for the final diagnosis.
The location of an upper third molar within the maxillary sinus may be associated with the development of mucocele13 or dentigerous cyst6,8. In this study, the patient presented a hyperdense area associated with the tooth, compatible with mucous tissue.
Surgical removal should be considered when intra-sinusal third molars are symptomatic or associated with cysts. The traditional approach is the Caldwell-Luc procedure, in which an opening is made into the maxillary sinus3,5. Alternatively, transnasal endoscopy, another approach with lower morbidity, can also be used9,14.
The need for surgical intervention or removal of a non-erupted third molar should be analyzed for each individual patient. Removal is indicated when the tooth is associated with cysts or tumors, untreatable caries, periodontal disease, recurrent pericoronitis, abscess and osteomyelitis, or in cases of prophylactic extraction15. In this study, radiographic follow-up was recommended due to the absence of symptoms or pathological processes.
FINAL CONSIDERATIONS
Panoramic radiographs do not provide reliable information about the exact location of ectopic teeth in the maxillary sinus. Cone beam computed tomography should be the preferred method to help in establishing the diagnosis and planning treatment and follow-up.
REFERENCES
1. El-Sayed Y. Sinonasal teeth. J Otolaryngol. 1995;24(3):180-3. [ Links ]
2. Yusuf H, Quayle AA. Intracondylar tooth. Int J Oral Maxillofac Surg. 1989;18(6):323. [ Links ]
3. Keros J, Susić M. Heterotopia of the mandibular third molar: a case report. Quintessence Int. 1997;28(11):753-754. [ Links ]
4. De Moraes Ramos FM, de Barros Quirino Martins MG, de Almeida SM, Novaes PD, Haiter-Neto F. Multiple radiographic projections in diagnosis of uncommon unerupted tooth. Dentomaxillofac Radiol. 2006;35(1):65-6. [ Links ]
5. Bodner L, Tovi F, Bar-Ziv J. Teeth in the maxillary sinus--imaging and management. J Laryngol Otol. 1997;111(9):820-4. [ Links ]
6. Büyükkurt MC, Tozoglu S, Aras MH, Yolcu Ü. Ectopic eruption of a maxillary third molar tooth in the maxillary sinus: A case report. J Contemp Dent Pract. 2005;6(3):104-10. [ Links ]
7. Güler N, Çildir S, Iseri U, Sandalli N, Dilek O. Hypohidrotic ectodermal dysplasia with bilateral impacted teeth at the coronoid process: A case rehabilitated with mini dental implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(5):E34-E38. [ Links ]
8. Srinivasa Prasad T, Sujatha G, Niazi TM, Rajesh P. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: a rare entity. Indian J Dent Res. 2007;18(3):141-3. [ Links ]
9. Suarez-Cunqueiro MM, Schoen R, Schramm A, Gellrich NC, Schmelzeisen R. Endoscopic approach to removal of an ectopic mandibular third molar. Br J Oral Maxillofac Surg. 2003;41(5):340-2. [ Links ]
10. Salmerón JI, del Amo A, Plasencia J, Pujol R, Vila CN. Ectopic third molar in condylar region. Int J Oral Maxillofac Surg. 2008;37(4):398-400. [ Links ]
11. Suomalainen A, Ventä I, Mattila M, Turtola L, Vehmas T, Peltola JS. Reliability of CBCT and other radiographic methods in preoperative evaluation of lower third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(2):276-84. [ Links ]
12. Lamb JF, Husein OF, Spiess AC. Ectopic molar in the maxillary sinus precipitating a mucocele: a case report and literature review. Ear Nose Throat J. 2009;88(8):E6-E11. [ Links ]
13. Di Pasquale P, Shermetaro C. Endoscopic removal of a dentigerous cyst producing unilateral maxillary sinus opacification on computed tomography. Ear Nose Throat J. 2006;85(11):747-8. [ Links ]
14. Adeyemo WL. Do pathologies associated with impacted lower third molars justify prophylatic removal? A critical review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(4):448-52. [ Links ]
15. Beriat GK, Beriat NÇ, Yalçinkaya E. Ectopic molar tooth in the maxillary sinus: a case report. Clin Dent Res. 2011;35(2):35-40. [ Links ]
 Corresponding Author:
Corresponding Author:
Frederico Sampaio Neves
Departamento de Diagnóstico Bucal
Faculdade de Odontologia de Piracicaba
Universidade Estadual de Campinas
Av. Limeira, 901, Areião, Caixa Postal 52
CEP 13414-903 – Goiânia – Goiás – Brasil
Tel./fax: +55 (19) 2106-5327
E-mail:fredsampaio@yahoo.com.br
