










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.18 no.35 Canoas Jul./Dez. 2012
SCIENTIFIC ARTICLE
Conservative treatment of shovel-shaped upper incisors and dens invaginatus: a case study
Tratamento conservador de incisivos superiores em forma de pá e dens invaginatus: um estudo de caso
Maisa Oliveira Caliani Corral Morales1; Luiz Evaristo Ricci Volpato2; Fabio Luis Miranda Pedro2; Cyntia Rodrigues de Araújo Estrela3; Álvaro Henrique Borges2
1Specialist in Pediatric Dentistry and a candidate at the Master’s Program of Integrated Dentistry, University of Cuiabá, Cuiabá, MT, Brazil.
2Professors at the Program of Integrated Dentistry, University of Cuiabá, Cuiabá, MT, Brazil.
3PhD in Cellular and Molecular Biology from the Federal University of Goiás, GO, Brazil.
ABSTRACT
The purpose of this paper was to describe the conservative treatment adopted in one nonsyndromic patient presenting with shovel-shaped upper incisors and dens invaginatus. A 13-yearold female patient sought treatment reporting pain in response to cold stimuli in the upper anterior teeth. Four upper incisors with shovel-shaped anatomical alterations in the palatal side of the crown were detected during intra-oral clinical examination; in addition, imaging exams revealed a type I dens invaginatus in tooth 22. There was no communication between the carious lesion and the pulp chamber, and a restorative treatment plan was developed. After 2 years of follow-up, the patient showed absence of pain, fistulas, swelling, or periodontal pockets. When faced with anomalous teeth, conservative procedures should be considered as a potential solution for restorative and endodontic treatment.
Keywords: Conservative Treatment, Dens invaginatus, Shovel-shaped Teeth, Tooth Abnormalities.
RESUMO
O objetivo desse trabalho foi descrever o tratamento conservador adotado em um paciente não sindrômico apresentando incisivos em forma de pá (shovel-shaped) e dens invaginatus. Paciente de 13 anos de idade, do sexo feminino, procurou tratamento com queixa de dor em resposta a estímulos frios nos dentes superiores anteriores. Quatro incisivos superiores com alterações anatômicas em forma de pá na face palatal da coroa foram detectados durante o exame clínico intraoral; além disso, exames de imagens revelaram a presença de dens invaginatus tipo I no dente 22. Não havia comunicação entre a cárie e a câmara pulpar, e um plano de tratamento restaurador foi desenvolvido. Após 2 anos de seguimento, a paciente demonstrava ausência de dor, fístulas, edema ou bolsas periodontais. Ao se deparar com anomalias dentárias, procedimentos conservadores devem ser considerados como uma potencial solução de tratamento restaurador e endodôntico.
Palavras-chave: Tratamento Conservador. Dens invaginatus. Dentes em Forma de Pá. Anormalidades Dentárias.
INTRODUCTION
Dental anomalies are defects caused by genetic disorders or environmental factors during tooth structure formation1-3. Teeth begin to develop around the sixth week of intrauterine life, and the process continues through many stages1. Even though developmental anomalies may occur at any stage, they will often manifest only later in life, when teeth are completely formed2,3. Anomalies in shape (morphological anomalies) may involve only one tooth, a group of teeth, or even the complete dentition4. The simultaneous presence of multiple anomalies may be related to specific syndromes, especially in patients with chromosomal alterations combined with multi-systemic alterations2,5.
Dens invaginatus is a developmental anomaly resulting from invaginations in the external surface of the tooth crown prior to mineralization of the hard tissues6. The etiology of the condition is still controversial and may be related to local delays in enamel formation, folding of the enamel organ, or external influences on the tooth bud7. The teeth most commonly affected are the upper lateral incisors, followed by the upper central incisors6. Mandibular teeth are rarely affected8, and few cases have been reported involving the deciduous dentition8. Cases of bilateral occurrence have been reported, and the exact homology remains to be investigated in cases where just one tooth is affected6. Depending on the depth of enamel invaginations inside the tooth, anomalies may be classifi ed as type I (the invagination ends as a blind sac and is limited to the coronal portion), type II (the invagination extends to the cementoenamel junction [CEJ] but remains within the main canal), or type III (the invagination extends throughout the entire interior of the root canal and reaches the apical area of the tooth, giving rise to two or more foramina)9.
Shovel-shaped incisors are anatomically characterized by a robust marginal ridge surrounding a deep lingual fossa5. Although the etiology of shovel-shaped incisors has been shown to involve a genetic component10, these teeth are considered to be anatomical variants rather than morphological defects5. They differ considerably among distinct ethnic groups and are commonly found in Asians, Africans and Native Americans, but rarely among Europeans10. The condition may affect 9% of the incisors (4% of the central and 5% of the lateral ones)11.
Even though dens invaginatus and shovel-shaped incisors are rare anomalies, they may pose challenges to dental practitioners in terms of the restorative and endodontic treatment of the teeth affected1. When deciding upon the most appropriate treatment, it is important to consider the degree of pulp involvement vs. biophysical characteristics of the tooth, symptoms reported, and pulp vitality test results12.
The present study describes the conservative treatment adopted in a non-syndromic female patient presenting with shovel-shaped upper incisors and dens invaginatus in tooth 22.
CASE DESCRIPTION
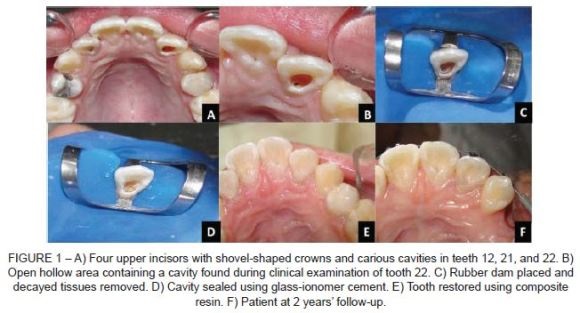
A 13-year-old white female patient sought treatment at the Pediatric Dental Clinic of the Cuiabá School of Dentistry (Cuiabá, MT, Brazil), reporting pain in response to cold stimuli affecting the upper anterior teeth. Four upper incisors with shovel-shaped anatomical alterations in the palatal side of the crown were detected during intra-oral clinical examination, we well as carious lesions in teeth 12, 21, and 22 (Figure 1A). Pulp tests were performed in all anterior teeth using Endo-Frost (Roeko-Wilcos do Brasil, Rio de Janeiro, RJ, Brazil) and suggested the presence of vital pulp tissue. As a result, treatment plan consisted of eliminating the offending agent. Tooth 12 was restored using EvoluX composite resin (Dentsply™, Maillefer), whereas teeth 11 and 21 underwent four weekly sessions using Duraphat fluoride varnish (Colgate™, A. Nattermann & Cie. GmbH, Germany) (Figure 1F).
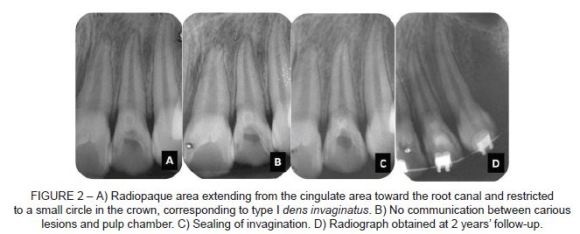
An open hollow area containing a cavity was found in tooth 22 during clinical examination (Figure 1B). After radiographic examination, the area was found to be as radiopaque as enamel. It extended from the cingulate area toward the root canal and was restricted to a small circle in the crown, corresponding to type I tooth invagination (Figure 2A). No communication was found between the carious lesion and the pulp chamber while inspecting the invaginated area (Figure 2B). Therefore, a restorative treatment plan was developed. Anesthesia consisted of infraorbital nerve block with palatal complementation. A rubber dam was placed, and decayed tissues were removed (Figure 1C). After gaining access to the invaginated area, the cavity was sealed with Vitremer glass ionomer cement (3M ESPE, St. Paul, MN, USA) (Figure 1D). A periapical radiograph was obtained to confirm sealing of the invagination (Figure 2C). Subsequently, the tooth was restored using EvoluX composite resin (Dentsply™, Maillefer). The rubber dam was then removed and occlusion was verified (Figure 1E). The patient was followed for 2 years. After this period, clinical (Figure 1F) and radiographic (Figure 2D) findings evidenced treatment success. the preservation of the pulp vitality was verified through the vitality test. An absence of pain, fistulas, swelling and periodontal pockets were also verified.
DISCUSSION
Anomalies occur as a consequence of genetic and environmental factors that interfere with the morphological differentiation of dental structures2. The simultaneous presence of multiple anomalies may be related to specific syndromes, particularly in patients with chromosomal and multi-systemic alterations2,5. However, there are also reports in the literature of patients without generalized abnormalities or a positive family history who are diagnosed with dental anomalies9, as was the case with the patient here described.
Our patient presented with four shovel-shaped upper incisors and a type I dens invaginatus affecting an upper lateral incisor. To avoid the risk of root-pulp contamination, preventative and restorative treatment should be performed before the tooth is affected by dental caries7. Treatment decisions should be based on an in-depth pre-operative evaluation of the gravity and complexity of the invagination12,13.
Dens invaginatus is a developmental anomaly that most commonly affects the upper lateral incisors6, and type I invagination is its most common manifestation14. When the invagination does not connect with the root canal system, pulp vitality may be preserved15. Under these circumstances, patient age, physical integrity, associated conditions, and the morphological characteristics of the anomaly will determine the best treatment approach12. Conservative restoration procedures, surgical therapies, or tooth extraction may be used15. In the present case study, pulp vitality tests were necessary to verify that the pulp was healthy12,13. The presence of a carious lesion with no pulp involvement led to the decision of immediately sealing the invagination and restoring the tooth, so as to prevent the need for further pulp treatment.
Shovel-shaped incisors are regarded as an anatomical variation rather than as a morphological defect5. Upper incisors are the teeth most commonly affected16. Notwithstanding, due to difficulties with proper cleaning, these teeth may end up allowing the entry of microorganisms and irritants, increasing the susceptibility of the dental structure to tooth decay15. Chronic irritation results in pulp necrosis and apical abscess, which should be prevented by sealing the cavity with sealant or restorative material and maintaining good oral hygiene16. In our case, the use of composite resin was indicated to perform the restoration. Moreover, rigorous, regular reviews are recommended to maintain a physical barrier and prevent pulp contamination7. Long-term clinical and radiographic monitoring will determine the efficacy of the therapeutic approach adopted.
CONCLUSION
Based on the case presented, it is possible to conclude that conservative procedures should be considered as a potential solution for the restorative and endodontic treatment of anomalous teeth.
REFERENCES
1. Metgud S, Metgud R, Rani K. Management of a patient with a taurodont, single-rooted molars associated with multiple dental anomalies: a spiral computerized tomography evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e81-6. [ Links ]
2. Suprabha BS, Sumanth KN, Boaz K, George T. An unusual case of non-syndromic occurrence of multiple dental anomalies. Indian J Dent Res. 2009;20:385-7. [ Links ]
3. Marques-da-Silva B, Baratto-Filho F, Abuabara A, Moura P, Losso EM, Moro A. Multiple taurodontism: the challenge of endodontic treatment. J Oral Sci. 2010;52:653-8. [ Links ]
4. Robbins IM, Keene HJ. Multiple morphologic dental anomalies: report of a case. Oral Surg Oral Med Oral Pathol. 1964;17:683-90. [ Links ]
5. Lorena SC, Oliveira DT, Odellt EW. Multiple dental anomalies in the maxillary incisor region. J Oral Sci. 2003;45:47-50. [ Links ]
6. Carvalho-Sousa B, Almeida-Gomes F, Gominho LF, Albuquerque DS. Endodontic treatment of a periradicular lesion on an invaginated type III mandibular lateral incisor. Indian J Dent Res. 2009;20:243-5. [ Links ]
7. Sathorn C, Parashos P. Contemporary treatment of class II dens invaginatus. Int Endod J. 2007; 40:308-16. [ Links ]
8. Mupparapu M, Singer SR. A review of dens invaginatus (dens in dente) in permanent and primary teeth: report of a case in a microdontic maxillary lateral incisor. Quintessence Int. 2006;37:125-9. [ Links ]
9. Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957;10:1204-18. [ Links ]
10. Kimura R, Yamaguchi T, Takeda M, Kondo O, Toma T, Haneji K, Hanihara T, Matsukusa H, Kawamura S, Maki K, Osawa M, Ishida H, Oota H. A common variation in EDAR is a genetic determinant of shovel-shaped incisors. Am J Hum Genet. 2009;85:528-35. [ Links ]
11. Saini TS, Kharat DU, Mokeem S. Prevalence of shovel-shaped incisors in Saudi Arabian dental patients. Oral Surg Oral Med Oral Pathol. 1990;70:540-4. [ Links ]
12. Estrela C. Endodontic science. São Paulo: Artes Médicas; 2009. 1223p. [ Links ]
13. Kristoffersen Ø, Nag OH, Fristad I. Dens invaginatus and treatment options based on a classification system: report of a type II invagination. Int Endod J. 2008;41:702-9. [ Links ]
14. Hülsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30:79-90. [ Links ]
15. Kirzioğlu Z, Ceyhan D. The prevalence of anterior teeth with dens invaginatus in the western Mediterranean region of Turkey. Int Endod J. 2009;42:727-34. [ Links ]
16. Galindo-Moreno PA, Parra-Vázquez MJ, Sánchez-Fernández E, Avila-Ortiz GA. Maxillary cyst associated with an invaginated tooth: a case report and literature review. Quintessence Int. 2003;34:509-14. [ Links ]
 Corresponding Author:
Corresponding Author:
Álvaro Henrique Borges
Program of Integrated Dentistry
University of Cuiabá
Cuiabá, MT, Brazil
Tel.: +55-65-3363 1000
E-mail:ahborges@brturbo.com.br
