










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.19 no.37 Canoas Jul./Dez. 2013
Modified implant-supported fixed maxillary prosthesis: removable gingival veneer retained with attachments
Prótese fixa maxilar sobre implantes tipo protocolo modificada: gengiva destacável retida por encaixes
Jeferson L. Rabaiolli I; Bruno R. Rybu I; Roberta P. Russomanno II; Luis C. F. Frasca III; Elken G. Rivaldo IV
I Graduate students in the Graduate Program in Implantology, School of Dentistry, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II MSc in Implantology from the School of Dentistry, ULBRA, Canoas, RS, Brazil
III MSc in Prosthodontics and chair of the School of Dentistry, ULBRA, Canoas, RS, Brazil
IV MSc in Implantology and chair of the School of Dentistry, ULBRA, Canoas, RS, Brazil
ABSTRACT
This study reports a clinical case of prosthetic rehabilitation of a patient with a totally edentulous maxilla using a fixed prosthesis supported by six implants, but modified by the inclusion of a removable gingival veneer retained with attachments. This alternative provides a rehabilitation model as functional and comfortable as the fixed prosthesis, enhancing facial aesthetics (reestablishing lip support) and phonetics and facilitating patient access for proper periimplant hygiene and prosthesis cleaning. We concluded that implant-supported fixed maxillary restorations, modified by the inclusion of a removable gingival veneer, come as a great alternative in cases of severe maxillary alveolar ridge atrophy.
Keywords: Implants, Prosthetic Gingival Reconstruction, Implant-Supported Fixed Prosthesis.
RESUMO
Este trabalho relata um caso clínico de reabilitação protética dental em um paciente edêntulo total superior com prótese fixa tipo protocolo sobre seis implantes, porém modificada com o acréscimo de uma gengiva destacável e retida por encaixes de semiprecisão. Esta alternativa reabilitadora fornece ao paciente a funcionalidade e o conforto dos dentes fixos, bem como mantém a estética facial pelo apoio do lábio, mantém fonação adequada e possibilita correta higiene peri-implantar e da prótese, através de gengiva destacável retida por encaixes. Concluímos que as reabilitações fixas maxilares sobre implantes do tipo protocolo, modificadas pelo acréscimo de uma gengiva destacável, são uma ótima alternativa para os casos de severa atrofia vestibular do rebordo alveolar da maxila.
Palavras-chave: Implantes, Prótese de Reconstrução Gengival, Prótese Fixa Suportada por Implantes.
INTRODUCTION
Totally edentulous patients have increasingly requested implant-supported fixed restorations, because they provide greater stability and better masticatory function than conventional complete dentures and overdentures 1,2.
In most cases, these patients show different degrees of ridge deficiency, with a characteristic resorption pattern of the maxillary ridge and another of the mandibular ridge 3. In the maxilla, implant-supported fixed prosthetic rehabilitation often requires gingival augmentation, since ridge resorption is mainly horizontal and reduces upper lip support, particularly in the anterior region. In these cases, implants are often positioned palatally in relation to the ideal position of artificial teeth. For these cases, some authors suggest that the prosthesis design receive an artificial gingiva attached to the teeth 3,4. However, this condition invariably impedes patient access for proper oral hygiene in the cervical area of the prosthesis and in peri-implant areas 5.
On the other hand, prostheses developed with proper access for oral hygiene often give patients an aged facial appearance (due to loss of lip support), who also show unfavorable patterns of speech (due to unwanted air moving toward the open cervical areas of the prosthesis) and report dense accumulation of food debris 5,6.
Other authors suggest that this gingival augmentation be accomplished by means of a removable, acrylic-made gingival epithesis or artificial gingiva that can carry out the function of muscular support of the lips, closing interdental cervical spaces and allowing proper hygiene procedures in the prosthesis and implants 7,8.
This case report shows a new prosthetic augmentation option for deficient maxillary ridge, in complete rehabilitation using a fixed prosthesis supported by six implants, through the fabrication of a removable artificial gingiva retained with ballsocket attachments welded to the prosthesis metal framework, ensuring optimal stability for the device and, therefore, comfort and safety for the patient.
CASE REPORT
A 59-year-old man, with a totally edentulous maxilla, wearing a complete upper denture, inquired about the possibility of fixed prosthetic maxillary rehabilitation with osseointegrated implants. Clinical examination revealed loss of lip support in the absence of the prosthesis, as evidenced by the large thickness of the buccal flange of the patient's complete denture and on computed tomographic (CT) scan guide. CT scan supported the decision to place 6 Branemark System MKIII implants (Nobel Biocare, Göteborg, Sweden). Five months after implant placement, reopening was performed and healing abutments were placed (Figure 1). Multi-unit abutments (Nobel Biocare, Göteborg, Sweden) were then installed with a tightening torque of 32 N/cm2. Two transfer techniques were performed. In the first stage, closed-tray impression transfer copings were used to obtain a model with abutment replicas. Into this first model, open-tray transfer devices were installed and connected with orthodontic wire and low-shrinkage autopolymerizing acrylic resin (GC Pattern Resin; GC Europe N.V., Leuven, Belgium), i.e., creating a rigid acrylic bar between the transfer devices. This bar was sectioned with a thin disk. Over the sectioned bar, an individual impression tray was manufactured with openings to allow access only to the transfer devices. In the second stage, already in the mouth, the open-tray transfer devices around the sectioned acrylic bar were installed into the multi-unit abutments and then joined with autopolymerizing acrylic resin (GC Pattern Resin; GC Europe N.V., Leuven, Belgium). Using the impression open tray coated with polyether adhesive on the inside, abutment transfer was performed with medium density polyether (impregum, 3M/ESPE, St Paul, USA). To obtain a new working cast, impressions and abutment replicas were poured with a type IV dental stone (Fujirock; GC America, Alsip, USA). Artificial gingiva was used around the abutments prior to cast preparation.

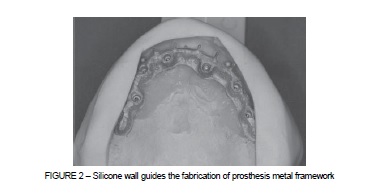
Tooth mounting was then performed. The choice of tooth size and color was based on the patient's own facial features. This tooth positioning was used as a guide for the fabrication of the prosthesis metal framework, using a silicone index (Figure 2). In this stage, the plate was adjusted to the teeth previously mounted according to the volume and shape of the framework. Also in this stage, we identified the best position to place the attachments of the removable gingival veneer.
At this moment, the thickness and extension of the removable gingival veneer was determined. This is a very important stage, because it defines, among other things, the need for lip support (esthetics), adequate speech production and access for proper periimplant hygiene. To facilitate good oral hygiene, whenever posterior gingival volume is necessary, gingival veneer attached to the artificial teeth should not extend anteriorly into the space between the two most distal implants, bilaterally.
Regarding the thickness of the removable gingival veneer, the patient's needs and the variety of attachment dimensions were considered. This choice depends on the volume needed for lip support, since the thinner the gingival veneer, the lower attachment dimensions should be. In this case, we chose resilient ball-socket attachments (CNG Axial; CNG Soluções Protéticas, São Paulo, Brazil), of 2.9 mm in height and diameter and retention with nylon clips (5 Newtons). It is worth noting that in this case the metal housing was not used, only the teflon female thread.
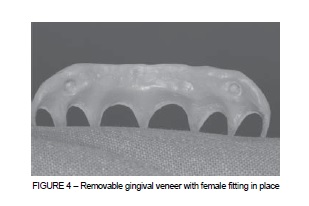
A diagnostic wax-up on the framework was then performed, since attachment male threads were welded in the ideal position. Upon verification and approval by the patient, at the prosthesis laboratory the acrylic resin of the fixed prosthesis was pressed, the removable gingival veneer was characterized and the retaining caps were captured in the gingiva (Figures 3 and 4).

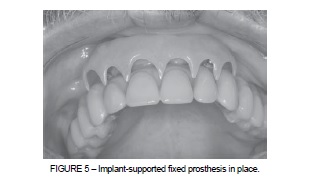
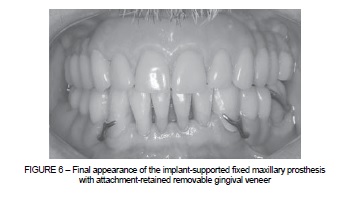
The fixed prosthesis was screwed into the abutments with a tightening torque of 20 N/cm2 applied to each screw. The patient received instructions in oral hygiene procedures in the cervical area of the prosthesis and also on how to insert and remove the detachable gingival veneer (Figure 5). Screw access holes were sealed with composite resin, and occlusal adjustment was then performed (Figure 6).
DISCUSSION
The loss of upper teeth causes different degrees of bone ridge resorption in height and anteroposterior dimension, depending on mechanical, biological and anatomical factors 3. The shape and structure of the edentulous residual ridge in patients who wear complete dentures demonstrate continuous loss of bone tissue after extraction and prosthesis placement 1. Therefore, in clinical situations in which patients with an edentulous maxilla request rehabilitation with fixed prostheses, some discrepancy often occurs between the ideal cervical position and shape of the teeth being manufactured and the remaining position of the ridge.
In the present clinical case, this discrepancy became evident after the initial observation of the buccal flange of the patient's complete denture, which was very thick. In addition, volumetric CT showed this discrepancy, through the analysis of details outlined by radiopaque material on the CT scan guide, which is a replica of the patient's complete denture.
Deficiencies of the remaining ridge in fixed complete or partial maxillary restorations may be compensated by both bone and gingival reconstructive surgical procedures 9, by prosthetic procedures using removable artificial gingiva or artificial gingiva attached to the prosthesis 4,5,8.
In partial restorations, although gingival augmentation might be accomplished with a removable gingival veneer 3, in most cases it is attached to the teeth; therefore, authors suggest that dentogingival prostheses should be fixed on natural teeth 4,10 or implants 3 and fixed-detachable prostheses should be retained with precision or semi-precision attachments on the implant superstructure 5.
In fixed complete maxillary prostheses, deficient alveolar ridge augmentation may also be achieved by different prosthesis designs. Several authors advocate implantsupported maxillary rehabilitation with dentogingival prostheses, with engagement of the pink portion into the teeth, targeting lip support and an adequate smile line 2,3.
However, these cases present some drawbacks. Many patients, although happy with the esthetic outcome of rehabilitation, have reported difficulty in carrying out hygiene procedures. This is perfectly understandable, since, if we design a dentogingival prosthesis with optimal closing of cervical spaces and optimal volume of artificial gingiva to obtain lip support, this patient will likely have great difficulty with periimplant hygiene and prosthesis cleaning, which interferes directly with prosthesis longevity and the patient's quality of life, due to possible pathological peri-implant alterations and damage to prosthetic components resulting from poor hygiene. On the other hand, prosthetic designs that promote access for proper hygiene often fail in terms of esthetics and lip support, which was provided by the flange of the conventional complete denture that the patient used to wear 5,7. In addition, these patients experience phonetic problems due to escape of unwanted air through the cervical areas of the prosthesis 5,6.
As a solution, some studies suggest the manufacturing of a gingival epithesis or artificial gingiva, gingival mask, or gingival prosthesis. A gingival epithesis may be indicated in cases of treated periodontitis, with resulting exaggerated cervical prominence, in cases of alveolar ridge augmentation 10, and also to assist in the cervical sealing of implant-supported fixed prostheses 7,8.
Other authors suggest the fabrication of dentogingival prostheses retained with precision attachments on a superstructure, which, in turn, is fixed on implants. These prostheses show excellent stability and masticatory function and can be easily removed by the patient 5.
We understand that the choice of rehabilitation method should be discussed with the patient at length, in an attempt to associate patient demands with the techniques currently available to the professional. Thus, we can provide individually focused patient treatment. In this particular case, the patient was clearly hoping to get a fixed prosthesis that would not pose any problems in terms of phonetics, esthetics and oral hygiene. Considering these arguments, we proposed, in accordance with the literature reviewed, a fixed prosthesis associated with a removable gingival veneer. For a better mechanical response from retention of the removable gingival veneer, we decided to attach the veneer to the fixed base with ball-socket attachments, with a medium retention level. Thus, the patient's demands for esthetics and comfort were fully met, with a relatively simple solution and an easy-handling device.
Attachment-retained removable gingival veneer associated with implant-supported fixed maxillary prostheses is a feasible, low-cost alternative in cases of bone resorption in the anterior maxilla, providing good facial and esthetic harmony, enhancing phonetics and facilitating oral hygiene.
REFERENCES
1. Peñarrocha M, Carrillo C, Boronat A, Balaguer J, Peñarrocha M. Palatal positioning of implants in severely resorbed edentulous maxillae. Int J Oral Maxillofac Implants. 2009;24(3):527-33. [ Links ]
2. Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Branemark System implants for completely edentulous maxillae: a 1-year retrospective clinical study. Clin Implant Dent Relat Res. 2005;7(Suppl 1):S88-94.
3. Holst S, Blatz MB, Bergler M, Wichmann M, Eitner S. Implant-supported prosthetic treatment in cases with hard and soft-tissue defects. Quintessence Int. 2005;36(9):671-8.
4. Coachman C, Salama M, Garber D, Calamita M, Salama H, Cabral G. Prosthetic gingival reconstruction in a fixed partial restoration. Part 1: introduction to artificial gingiva as an alternative therapy. Int J Periodontics Restorative Dent. 2009;29(5):471-7.
5. Morgano SM, Verde MA, Haddad MJ. A fixed-detachable implant-supported prosthesis retained with precision attachments. J Prosthet Dent. 1993;70(5):438-42.
6. Lundqvist S. Speech and other oral functions. Clinical and experimental studies with special reference to maxillary rehabilitation on osseointegrated implants. Swed Dent J Suppl. 1993;91:1-39.
7. Brygider RM. Precision attachment-retained gingival veneers for fixed implant prostheses. J Prosthet Dent. 1991;65(1):118-22.
8. Beckett HA, Wright PS. Construction of a gingival mask in association with an Implant-retained fixed maxillary prosthesis: a case report. Eur J Prosthodont Restor Dent. 1993;2(2):57-60.
9. von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. Clin Oral Implants Res. 2006;17(4):359-66.
10. Carvalho W, Barboza EP, Gouvea CV The use of porcelain laminate veneers and a removable gingival prosthesis for a periodontally compromised patient: a clinical report. J Prosthet Dent. 2005;93(4):315-7.
 Correspondence:
Correspondence:
Elken G. Rivaldo
Rua Pedro de Oliveira Bittencurt, 207, Bairro Tristeza
CEP 91900-230 – Porto Alegre, RS, Brazil
E-mail: elkenrivaldo@gmail.com
