










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.20 no.38 Canoas Jan./Jun. 2014
Effectiveness of a desensitizing dentifrice in obliterating dentinal tubules: an in vitro study
Efetividade de um dentifrício dessensibilizante na obliteração dos túbulos dentinários: estudo in vitro
Caroline Grings I; Maria Teresa Martins Fasolo II; Henrique Castilhos Ruschel III
I DDS from the School of Dentistry of Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II Lato Sensu degree in Periodontology from Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil, and an MSc degree in Periodontology from ULBRA, Canoas, RS, Brazil; professor at the School of Dentistry of ULBRA, Canoas, RS, Brazil
III Lato Sensu degree in Cell Biology, Histology and Microscopic Anatomy from ULBRA, Canoas, RS, Brazil, a MSc degree in Pediatric Dentistry from Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil, and a PhD degree in Pediatric Dentistry from Universidade de São Paulo (USP), São Paulo, SP, Brazil. He is a professor at the School of Dentistry of ULBRA, Canoas, RS, Brazil.
The authors have no conflicts of interest to declare concerning the publication of this manuscript.
ABSTRACT
The most widely used method for treatment of dentin hypersensitivity is daily brushing with desensitizing dentifrices, particularly those containing active ingredients capable of obliterating the dentinal tubules, such as arginine. The present study sought to assess the action of a desensitizing dentifrice on dentin in vitro. Twenty dentin samples were obtained from 10 sound, freshly extracted third molars. The dentin specimens were distributed across four groups: group 1, one application of the dentifrice only, using a finger and rubbing for 1 minute; group 2, two daily applications of the dentifrice, by brushing, for 2 days; group 3, two daily applications of the dentifrice, by brushing, for 3 days; and group 4, no treatment. Samples were analyzed by scanning electron microscopy. There was no obliteration of dentinal tubules in the specimens from group 1. In group 2, partial or complete obliteration of dentinal tubules was observed in all specimens. In group 3, complete obliteration of tubules was observed in all specimens. We conclude that twice-daily application of the tested dentifrice by brushing, for 2 days or longer, led to obliteration of dentinal tubules. This effect may contribute to a reduction in dentin hypersensitivity.
Keywords: Dentin Hypersensitivity, Desensitizing Dentifrices, Tooth Sensitivity.
RESUMO
O método mais empregado no tratamento da hipersensibilidade dentinária é a escovação diária com dentifrícios dessensibilizantes, principalmente aqueles que contêm elementos ativos com capacidade de obliterar os túbulos dentinários, como a arginina. O objetivo deste trabalho foi avaliar a ação, in vitro, de um dentifrício dessensibilizante sobre a dentina. Obtiveram-se 20 amostras de dentina a partir de 10 terceiros molares hígidos recém-extraídos. As amostras de dentina foram distribuídas em quatro grupos: grupo 1, uma única aplicação do dentifrício dessensibilizante por fricção com o dedo, durante um minuto; grupo 2, duas escovações diárias com o dentifrício dessensibilizante, durante dois dias; grupo 3, duas escovações diárias com o dentifrício dessensibilizante, durante três dias; grupo 4, sem tratamento. As amostras foram analisadas em microscópio eletrônico de varredura. Não houve obliteração dos túbulos dentinários em nenhuma das amostras do grupo 1. No grupo 2, observou-se obliteração parcial ou total dos túbulos dentinários em todas as amostras. No grupo 3, houve obliteração dos túbulos em todas as amostras de dentina. Conclui-se que o dentifrício dessensibilizante levou à obliteração tubular quando utilizado a partir de dois dias, com duas escovações diárias, podendo esta ação contribuir para a redução da hipersensibilidade dentinária.
Palavras-chave: Hipersensibilidade Dentinária, Dentifrícios Dessensibilizantes, Sensibilidade Dentária.
INTRODUCTION
In recent decades, oral conditions such as dentin hypersensitivity have increasingly become an object of discussion in dental research 1,2. Dentin hypersensitivity is defined as a short, sharp pain arising from exposed dentin in response to typically thermal, evaporative, tactile, osmotic or chemical stimuli and which cannot be ascribed to any other form of dental defect or pathology 2,3. Pain does not occur spontaneously and does not persist after removal of the stimulus 3-5.
Studies have reported a wide range of prevalence for dentin hypersensitivity, from 3% to 73% 6,7. This variation is attributable to differences in the methods used for diagnosis and in study design 1,7.
Several theories have been proposed in attempts to explain dentin hypersensitivity 1,2,8,9. In current dental practice, the hydrodynamic theory is widely accepted as an explanation of the mechanism of pain in dentin hypersensitivity 2,3,8. Not all exposed dentin is sensitive 10. Exposed dentin is coated by the smear layer, and the dentinal tubules are occluded by calcium phosphate deposits derived from saliva 10. Sensitivity occurs when the smear layer that coats the dentinal tubules is removed, exposing them to the oral environment 10,11.
Hypersensitivity lesions are most prevalent in the buccal cervical areas of the teeth 4,12. Loss of crown enamel occurs due to wear of the tooth surface through events of a physical (abrasion) or chemical (erosion) nature 13-16. Some authors suggest that a process known as abfraction may occur in the buccal cervical area of the tooth 2. Tooth wear is usually not due to the action of a single physical or chemical agent, but rather due to an interaction between two or more etiological agents acting in synergy 13,15-17. The gingival recession, which causes exposure of the root surface, appears to be multifactorial, with traumatic tooth brushing being particularly associated with this condition 4,12,16,18,19.
Two proposed treatment mechanisms are currently available for dentin hypersensitivity: physical occlusion of the dentin tubules, which accounts for the majority of treatment modalities, or chemical blockade of pulp tissue nerve transmission, using potassium-based compounds to depolarize neural synapses 4,5,10,20-25.
Physical occlusion of the dentinal tubules can be accomplished with a series of agents that deposit obliterating material directly onto the tubules 5,21,25. Dentifrices containing strontium-based and, more recently, arginine-based active ingredients are seemingly capable of inducing tubular obliteration 1,5,21,26,27.
Arginine has been added as an active ingredient to established dentifrice formulations. Using this method, a dentifrice containing 8% arginine, calcium carbonate, and 1450 ppm fluoride was developed 1. This dentifrice formulation has proven activity on the dentin, producing tubular obliteration and reducing sensitivity 5,21,26,27. The mechanism of action of arginine-based desensitizing dentifrices has been attributed to the formation of an arginine, calcium carbonate, and phosphate plug directly atop the tubules, occluding and obliterating them 5.
The present study assessed the in vitro effects on dentin of a desensitizing dentifrice containing 8% arginine, calcium carbonate, and 1450 ppm fluoride, after several different protocols of application.
METHODOLOGY
Tooth selection
Ten sound, freshly extracted third molars were selected. After extraction, the teeth were immediately stored in 3% glutaraldehyde, for 14 days, until the time of use. The selected teeth were free of restorations, caries, or enamel defects.
The patients who donated their teeth for this study were aged 22 to 35 years and all provided written informed consent for the use of their teeth.The present study was approved by the Research Ethics Committee (CEP-ULBRA) with judgment number 30173.
Collection and preparation of dentin specimens
The root portion of each selected tooth was placed within a segment of PVC tubing (diameter 2 cm, height 2.5 cm) and embedded in self-curing acrylic resin so as to leave the cementoenamel junction exposed. The crown enamel on the buccal and palatal/lingual surfaces of each tooth was worn down using a high-speed diamond bur (model 1811.4138, KG Sorensen, Cotia-SP, Brazil) under constant cooling. A double-sided flexible diamond disc (KG Sorensen, Cotia-SP, Brazil) was then used to separate the buccal and palatal/ lingual portions of each tooth from the remaining dental structure. Thus, two specimens were obtained from each tooth, for a total of 20 specimens. The area of exposed dentin in each specimen was approximately 4x5 mm.
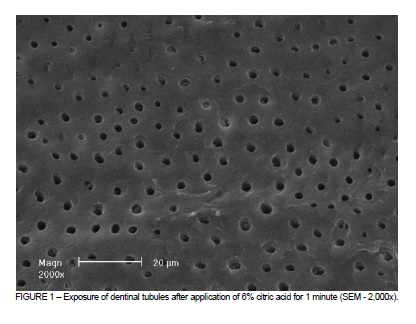
All specimens underwent application of 6% citric acid with a microbrush (KG Sorensen, Brazil), for 1 minute, in an attempt to remove the smear layer and expose the dentinal tubules. After application, the specimens were rinsed with water to remove any remaining acid, and submerged in an ultrasonic bath with distilled water for 30 min.
Treatment of dentin specimens
The desensitizing dentifrice tested in this study contains 8% arginine, calcium carbonate, and 1450 ppm fluoride (Colgate® Sensitive Pro-Alívio™, Colgate-Palmolive Co., Brazil).
The 20 dentin specimens were randomly divided across four groups according to the type of treatment. All treatments were performed by the same investigator. Each group comprised five dentin specimens: group 1, one application of the dentifrice only, using a finger and rubbing for 1 minute, as per manufacturer instructions; group 2, two daily applications of the dentifrice, by brushing, for 2 days; group 3, two daily applications of the dentifrice, by brushing, for 3 days; and group 4, no treatment (control group).
Specimens in groups 2 and 3 were brushed with a soft-bristled toothbrush (Medfio, Curitiba, Paraná, Brazil), twice daily, for 1 minute each, with a 12-interval between brushings. Specimens from groups 1, 2, and 3 were stored in individual containers with 5 mL artificial saliva, which was obtained from a compounding pharmacy. Before placing in artificial saliva, each sample was rinsed with water to remove any excess dentifrice. These containers were stored at 37°C throughout the 3-day experiment period, in an attempt to simulate the oral environment.
Specimen preparation for scanning electron microscopy
Samples were dehydrated in graded ethanol baths (50, 70, and 95%, 10 min in each concentration) followed by two 10-min baths in 100% ethanol, and were then stored in a desiccator at 37°C for 24 hours to complete dehydration. Finally, they were attached to stubs and metal-coated for scanning electron microscopy (SEM) analysis.
Scanning electron microscopy analysis
The specimens were imaged with a Philips XL 20 scanning electron microscope (Philips, The Netherlands), at 2,000x, 5,000x, and 10,000x magnification.
RESULTS
Complete exposure of the dentinal tubules as a result of acid conditioning is clearly visible in control group (Figure 1).
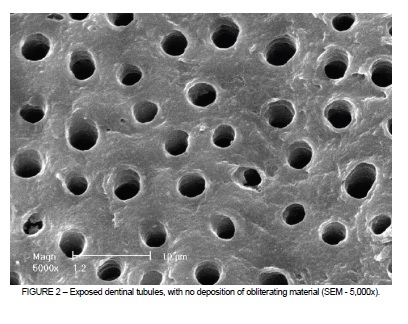
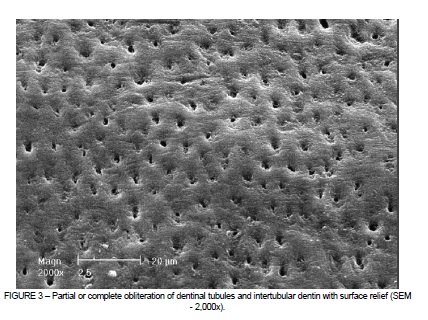
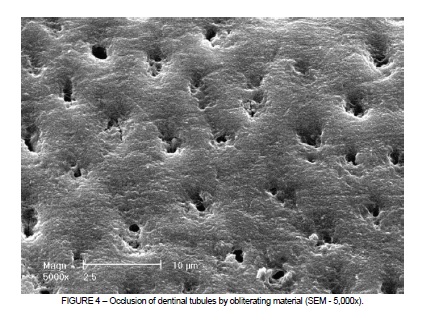
Dentinal tubule obliteration was not achieved in any of the specimens in group 1 (Figure 2). In group 2, partial or complete obliteration of the dentinal tubules was observed, with surface relief in areas of intertubular dentin (Figures 3 and 4).
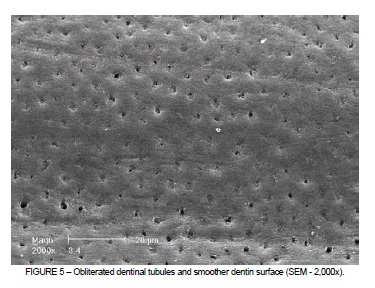
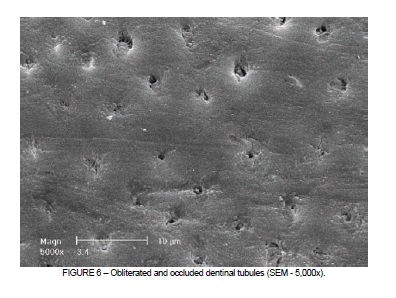
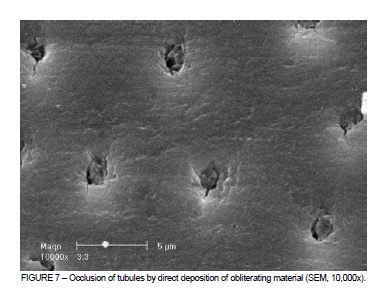
Specimens in group 3 exhibited greater obliteration of dentinal tubules and a smoother dentin surface as compared with group 2. Most specimens in group 3 were completely obliterated; only a few were partially obliterated. Deposition of obliterating material within the tubules was visible on SEM analysis (Figures 5, 6, and 7).
DISCUSSION
Dentin hypersensitivity is a condition that affects patient quality of life. Most individuals who seek treatment do so in search of relief for their pain 3. Preferably, reversible procedures should be attempted before irreversible modalities 1,3,6,20. These less-invasive treatment options include the use of desensitizing dentifrices 5,20,21,23-25.
Daily use of desensitizing dentifrices should be recommended as the first-line treatment of choice for dentin hypersensitivity, as it is a noninvasive, cost-effective, and readily available method 3,5,12,21. Furthermore, tooth brushing is a globally accepted dental hygiene method that is part of the daily routine of many patients, and thus requires no changes in habits 3,12.
Topical application of desensitizing dentifrices for reduction of dentin hypersensitivity has been assessed elsewhere 26, but further research is still required. In the present study, a single application of desensitizing dentifrice was not able to obliterate the dentinal tubules in any of the tested specimens. Nevertheless, a previous in vitro study reported that a single application of desensitizing dentifrice for one minute was able to induce obliteration of the dentinal tubules 21. Further research should assess whether the reduction of dentin hypersensitivity observed after a single application of desensitizing dentifrice is attributable to the formation of a mechanical barrier atop the dentin rather than by a true effect on the dentinal tubules. In the present study, group 1 specimens, which were rinsed after a single application of dentifrice and then stored in artificial saliva for 3 days, were no different control group specimens, which were not treated with dentifrice.
In groups 2 and 3, the desensitizing dentifrice successfully obliterated the dentinal tubules by deposition of obliterating material within the tubules. Effective treatment of dentin hypersensitivity with desensitizing dentifrices, with sustained effect, requires that patients brush their teeth with the dentifrice at least twice daily 3,26. The mechanism of action of this dentifrice is believed to involve the formation of an arginine, calcium carbonate, and phosphate plug directly onto the exposed dentinal tubules, thus occluding them over the course of the treatment 5.
The longer the use of desensitizing dentifrice, the greater the benefit obtained in terms of obliteration of dentinal tubules and, consequently, reduction of dentin hypersensitivity 1,26. In the present study, effects were observed with as little as 2 days of twice-daily use.
An interesting finding observed in group 2 was a "surface relief" effect on the dentin, which suggests deposition of material not only within the tubules, but also in areas of intertubular dentin. The "smoother" surface observed in group 3 might be explained by an abrasive effect of the dentifrice, as specimens in this group were exposed to an additional day of brushing. Further studies are required to elucidate these findings.
Wang et al. 24 assessed the efficacy of an arginine-containing dentifrice in occluding the dentinal tubules by performing an acid challenge after application of the dentifrice. After immersion in acid for 5 minutes, the dentinal tubules remained occluded by the dentifrice, but less so than before the acid challenge. Olley et al. 27 assessed tubular occlusion after an acid challenge in dentin samples treated with desensitizing dentifrices. The specimens were brushed twice daily with two different dentifrices, one having arginine as its active ingredient and the other containing strontium instead. Acid challenge was performed after brushing. The authors found that, after 3 and 4 dias of twice-daily brushing followed by acid challenge, the strontium-based dentifrice was significantly superior to the arginine-based dentifrice in terms of dentinal occlusion. Further studies are required to assess the long-term effect of these dentifrices and ascertain whether the obliterating layer of material deposited atop the dentinal tubules resists the dietary acid challenge.
In the present in vitro study, the use of desensitizing dentifrice led to partial or complete occlusion of the dentinal tubules after 2 days of twice-daily brushing. Taking into account that desensitizing dentifrices could be used as a first-line treatment for dentin hypersensitivity, the patterns of dentinal tubule occlusion after 2 days of application were satisfactory.
CONCLUSIONS
In conclusion, taking into account the limitations of an in vitro study, a single application of desensitizing dentistry by rubbing with the fingertip for 1 minute was not sufficient to obliterate dentinal tubules. Conversely, twice-daily brushing with the dentifrice produced obliteration of the dentinal tubules within 2 days. Further studies are required to assess the long-term effectiveness of the dentifrice used in this study and analyze whether the obliterating material formed after 2 days of brushing with the dentifrice is able to resist the acid challenge of a potentially erosive diet.
REFERENCES
1. Cummins D. Dentin hypersensitivity: from diagnosis from a breakthrough therapy for everyday sensitivity relief. J Clin Dent. 2009;20(1):1-9. [ Links ]
2. Addy M. Dentine hypersensitivity: new perspectives on an old problem. Int Dent J. 2002;52(5):367-75.
3. Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc. 2003;69(4):221-6.
4. Markowitz K, Pashley DH. Discovering new treatments for sensitive teeth: the long path from biology to therapy. J Oral Rehab. 2008;35(4):300-15.
5. Docimo R, Montesani L, Maturo P, Costacurta M, Bartolino M. Comparing the efficacy in reducing dentin hypersensitivity of a new toothpaste containing 8.0% arginine, calcium carbonate, and 1450 ppm fluoride to a commercial sensitive toothpaste containing 2% potassium ion: an eight-week clinical study in Rome, Italy. J Clin Dent. 2009;20(1):17- 22.
6. He S, Wang Y, Li X, Hu D. Effectiveness of laser therapy and topical desensitising agents in treating dentine hypersensitivity: a systematic review. J Oral Rehab. 2011;38(5):348- 58.
7. Que K, Ruan J, Fan X, Liang X, Hu D. A multi-centre and cross-sectional study of dentine hypersensitivity in China. J Clin Periodontol. 2010;37(7):631-7.
8. Brännström M, Aström A. A study on the mechanism of pain elicited from the dentin. J Dent Res. 1964;43(4):619-25.
9. Kawabata M, Hector MP, Davis GR, Parkinson CR, Rees GD, Anderson P. Diffusive transport within dentinal tubules: an X-ray microtomographic study. Arch Oral Biol. 2008;53(8):736-43.
10. Pashley DH. Dentine permeability and its role in the pathobiology of dentine sensitivity. Arch Oral Biol. 1994;39(Suppl.):73S-80S.
11. Vongsavan N, Matthews B. The relationship between the discharge of intradental nerves and the rate of fluid flow through dentine in the cat. Arch Oral Biol. 2007;52(7):640-7.
12. Rösing CK, Fiorini T, Liberman DN, Cavagni J. Dentine hypersensitivity: analysis of self-care products. Braz Oral Res. 2009;23(1):56-63.
13. Vanuspong W, Eisenburger M, Addy M. Cervical tooth wear and sensitivity: erosion, softening and rehardening of dentine; effects of pH, time and ultrasonication. J Clin Periodontol. 2002;29(4):351-7.
14. Lussi A, Merget B, Shellis PR, Wang X. Analysis of the erosive effect of different dietary substances and medications. Br J Nutr. 2012;107(2):252-62.
15. Wetton S, Hughes J, Newcombe RG, Addy M. The effect of saliva direved from different individuals on the erosion of enamel and dentine. A study in vitro. Caries Res. 2007;41(5):423-6.
16. Teleffsen G, Liljeborg A, Johannsen A, Johannsen G. The role of the toothbrush in the abrasion process. Int J Dent Hyg. 2011;9(4):284-90.
17. West NX, Hopper SM, O'Sullivan D, Hughes N, North M, Macdonal EL, Davies M, Claydon NC. In situ randomised trial investigating abrasive effects of two desensitising toothpastes on dentine with acidic challenge prior to brushing. J Dent. 2012;40(1):77- 85.
18. Tugnait A, Clerehugh V. Gingival recession – its significance and management. J Dent. 2001;29(6):381-94.
19. Addy M. Oral hygiene products: potential for harm to oral and systemic health? Periodontol 2000. 2008;48(1):54-65.
20. Davies M, Paice EM, Jones SB, Leary S, Curtis AR, West NX. Efficacy of desensitising dentifrices to occlude dentinal tubules. Eur J Oral Sci. 2011;119(6):497-503.
21. Petrou I, Heu R, Stranick M, Lavender S, Zaidel L, Cummins D, Sullivan RJ, Hsueh C, Gimzewski JK. A breakthrough therapy for dentine hypersensitivity: how dental products containing 8% arginine and calcium carbonate work to deliver effective relief of sensitive teeth. J Clin Dent. 2009;20(1):23-31.
22. Orchardson R, Gillam DG. Managing dentine hypersentivity. J Am Dent Assoc. 2006;137(7):990-8.
23. Orsini G, Procaccini M, Manzoli L, Giuliodori F, Lorenzini A, Putignano A. A Doubleblind randomized-controlled trial comparing the desensitizing efficacy of a new dentifrice containing carbonate-hydroxyapatite nanocrystals and a sodium fuoride-potassium nitrate dentifrice. J Clin Periodontol. 2010;37(6):510-7.
24. Wang Z, Sa Y, Sauro S, Chen H, Xing W, Ma X, Jiang T, Wang Y. Effect of desensitising toothpastes on dentinal tubule occlusion: a dentine permeability measurement and SEM in vitro study. J Dent. 2010;38(5):400-10.
25. Shen SY, Tsai CH, Yang LC, Chang YC. Clinical efficacy of toothpaste containing potassium citrate in treating dentin hypersensitivity. J Dent Sci. 2009;4(4):173-7.
26. Hamlin D, Mateo LR, Dibart S, Delgado E, Zhang YP, De Vizio W. Comparative efficacy of two treatment regimens combining in-office and at-home programs for dentin hypersensitivity relief: a 24-week clinical study. Am J Dent. 2012;25(3):146-52.
27. Olley RC, Pilecki P, Hughes N, Jeffery P, Austin RS, Moazzer R, Barlett D. An in situ study investigating dentine tubule occlusion of dentifrices following acid challenge. J Dent. 2012;40(7):585-93.
 Correspondence:
Correspondence:
Caroline Grings
Rua Augusto Jung, 101
CEP 93510-340, Novo Hamburgo, RS, Brazil
E-mail: carolineggrings@hotmail.com
