










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.20 no.38 Canoas Jan./Jun. 2014
A new condylar fracture fixation technique
Uma nova técnica de fixação de fratura condilar
Thiago Aragon Zanella I; Roger Corrêa de Barros Berthold II; Claiton Heitz III
I Graduate student in Oral and Maxillofacial Surgery, Department of Oral and Maxillofacial Surgery, Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil
II Master's candidate in Oral and Maxillofacial Surgery, Department of Oral and Maxillofacial Surgery, PUCRS, Porto Alegre, RS, Brazil
III Professor and head of the Department of Oral and Maxillofacial Surgery, PUCRS, Porto Alegre, RS, Brazil
The authors have no conflicts of interest to declare concerning the publication of this manuscript.
ABSTRACT
Mandibular condyle fractures are common and the best approach to treating them has been extensively discussed in the literature. There are basically two different approaches to treatment of condyle fractures: the functional method and the surgical method. In the case described here, the patient underwent general anesthesia for open reduction and internal fixation. After a submandibular approach to access the fracture site, a bur was used to make a perforation in the base of the condylar segment and a long screw (11 mm) was inserted in place leaving a portion protruding from the bone (6 mm). A groove was made in the lateral part of the mandibular ramus to accommodate the extra osseous portion of the screw. After reduction and stabilization of the condylar segment, a 2.0 mm miniplate was installed over the screw leaving the screw head in an inferior position to maximize retention. The patient enjoyed a rapid postoperative recovery and early jaw function was restored in a short period of time.
Keywords: Mandibular Condyle, Mandibular Fractures, Mandibular Injuries.
RESUMO
Fraturas de côndilo são comuns, e a melhor maneira de tratá-las tem sido extensivamente discutida na literatura. Há basicamente dois métodos distintos para tratar fraturas de côndilo, o método funcional e o método cirúrgico. No presente estudo, o paciente foi submetido à anestesia geral para realizar o método de redução aberta com fixação interna. Após ser realizada uma abordagem submandibular para acessar a região da fratura, uma perfuração, usando broca, foi realizada na base do segmento condilar e um parafuso longo (11 mm) foi inserido, deixando uma parte (6 mm) extra-ósseo. Um sulco foi feito na parte lateral do ramo mandibular para alocação da parte extra-óssea do parafuso. Após redução e estabilização do segmento condilar, uma miniplaca de 2.0 mm foi instalada por cima do parafuso deixando a cabeça do parafuso mais inferiormente para maximizar a retenção. O paciente teve uma recuperação pós-operatória rápida, e função a função mastigatória foi reestabelecida.
Palavras-chave: Côndilo Mandibular, Fraturas Mandibulares, Traumatismos Mandibulares.
INTRODUCTION
Mandibular condyle fractures are common and account for 19-52% of all mandibular fractures 1. The best way to treat condylar fractures has been an issue of contention since the early 1940s 2. The introduction of rigid internal fixation devices has further complicated the question of whether to employ an open or closed technique for condylar fractures 3. There are two different treatment approaches for these fractures: functional or surgical 3,4. Functional treatment consists of closed reduction with maxillomandibular fixation for a period of approximately 14 days 5. Surgical treatment consists of open reduction via an intra-oral or extra-oral approach using internal semi-rigid or rigid fixation. The indications for surgical treatment are: ramus shortened by more than 5 mm, greater than 30° angles on the fractured condyle and no contact between fragments, although when the bone fragments have suffered smaller displacements surgical treatment can still be used 5. There are descriptions of techniques for condyle fracture fixation in the literature; for example, two straight 2.0 mm miniplates, or one 2.0 mm miniplate. Open reduction and stabilization of the condyle can present a challenge for oral and maxillofacial surgeons, especially if the condyle has suffered severe medial displacement and offers a narrow neck for plate fixation. The objective of this article is to report on a clinical case in which a novel condylar fracture fixation technique was employed.
CASE REPORT
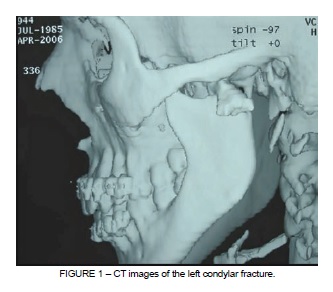
A patient was referred to the oral and maxillofacial surgery department at the Cristo Redentor Hospital in Porto Alegre, Brazil. He presented with limited jaw opening and pain and swelling on the left side of the mandible. The patient was diagnosed with a fracture of the left condyle on the basis of CT scan findings (Figure 1).
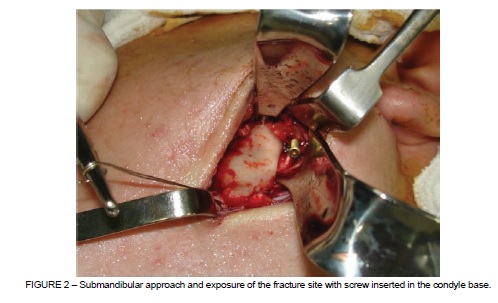
The patient underwent general anesthesia for open reduction and internal fixation. Erich arch bars were installed for transoperative maxillomandibular fixation. A submandibular approach was taken and the skin flap was elevated. The superficial muscular aponeurotic system (SMAS) was blunt dissected and the facial artery and vein were identified, plugged and retracted out of the surgical field. Masseter muscle fibers were separated longitudinally and the periosteum was incised. A bicortical perforation was made in the mandibular angle and a 1.0 stainless steel wire was passed through the hole to enable downwards traction of the mandibular ramus, with the aim of providing better visualization and reduction of the condylar segment. The fracture site and the base of the condylar segment were then visible. Next, a perforation was made with a bur in the base of the condylar segment and a long screw (11 mm) was inserted, leaving a portion (6 mm) protruding from the bone (Figure 2).
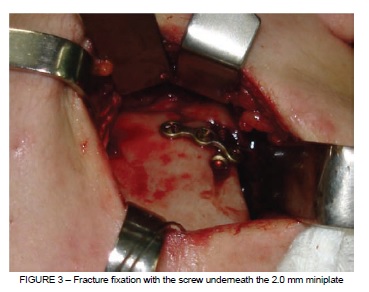
A needle holder attached to the screw was then used to reduce the condylar segment, and a bur mark was made in the mandibular ramus to define the position of the head of the screw after reduction. A groove was then cut into the lateral part of the mandibular ramus, to a size corresponding to the extra osseous portion of the screw, using a number 6 round carbide bur, in order to accommodate the extra osseous portion of the screw. After reduction and stabilization of the condylar segment, a 2.0 mm miniplate was installed over the screw, with the screw head in an inferior position to maximize retention (Figure 3). Surgical access was than sutured by planes.
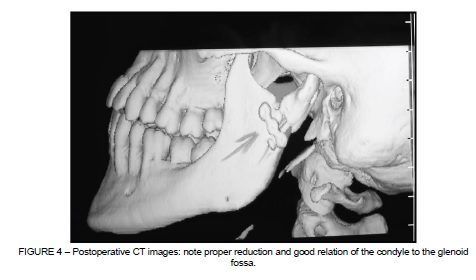
The patient enjoyed rapid postoperative recovery and jaw function was restored in a short period of time (Figure 4). The Erich arch bars were left in place for 14 days, without maxillomandibular fixation, to allow for jaw exercises to increase mouth opening, using two elastics, one on each side. The patient was instructed to adhere to a soft diet for a period of 14 days, in order to minimize bite force generated by mastication of solid foods. The patient made periodic visits to the oral and maxillofacial surgery department and no bite relapse or fractures of the fixation devices were observed over a two year follow-up period.
DISCUSSION
The introduction of rigid internal fixation has altered the outcomes of surgical interventions in oral and maxillofacial traumatology, particularly those conducted to treat the mandible 2. There are clear indications and contraindications for rigid fixation of condylar fractures. Valiati et al. 1, among others, has stated that rigid fixation is contraindicated for fractures of the head and neck of the condyle. The possibility of necrosis of the condylar segment and lack of bone mass for hardware fixation are the reasons for this conclusion 6. Significant displacement of the condylar segment is the main indication for rigid fixation, but correct reduction and stabilization of these fractures can present transoperative challenges, due to medial dislocation caused by traction of the medial pterygoid muscle and the shortened mandibular ramus, which impairs visualization 7,8.
In the case described in this article, insertion of the screw facilitated manipulation and proper fracture reduction, which in turn optimized use of surgery time. The traction wire attached to the mandibular angle made it easier to accomplish condyle reduction, but care must be taken not to pull too strongly, because this can lead to bite displacement, which is why tooth relationships must be checked throughout the surgical procedure 9. It is imperative that the perforation for screw fixation on the condylar segment be made between cortical and medullar bone, since if this is not done there is a high chance that the screw will work loose 10. The 3-hole, 2.0 mm plate was used in this case, but an L-shaped plate can be even more useful for controlling the condylar segment during fixation 11. Plate fixation can sometimes be hampered by a submandibular approach that makes it difficult to drill perpendicular to the plate 12. A retromandibular approach can be taken in order to overcome this possible complication 2.
The patient was given certain instructions to follow during the postoperative period. Erich arch bars are routinely used in our setting for transoperative maxillomandibular fixation and for jaw exercises or to correct bite relapse in the postoperative period. After 14 days, arch bars are usually removed if there are no occlusive complications. In the case described, the patient was not subjected to any period of postoperative maxillomandibular fixation, just a 14-day period on a soft diet, and no plates or screw fracture were seen over 2-year postoperative follow-up 3.
CONCLUSION
The technique applied in the case presented here proved to be a valid method for condylar fracture fixation, taking into consideration the patient's rapid functional recovery. Notwithstanding, further studies with larger samples are needed to validate the technique.
REFERENCES
1. Valiati R, Ibrahim D, Abreu MER, Heitz C, Oliveira RBO, Pagnoncelli RM. The treatment of condylar fractures: to open or not to open? A critical review of this controversy. Int J Med Sci. 2008;5(6):313-8. [ Links ]
2. Vasnaver A, Ahcan U, Rozman J. Evaluation of surgical treatment in mandibular condyle fractures. J Craniomaxillofac Surg. 2012;40(8):647-53.
3. Luo S, Li B, Long X, Deng M, Cai H, Cheng Y. Surgical treatment of sagittal fracture of mandibular condyle using long-screw osteosynthesis. J Oral Maxillofac Surg. 2011;69:1988-94.
4. Kyzas PA, Saeed A, Tabbenor O. The treatment of mandibular condyle fractures: A meta-analysis. J Craniomaxillofac Surg. 2012;40(8):e438-52.
5. Hayward JR, Scott RF. Fractures of the mandibular condyle. J Oral Maxillofac Surg. 1993;51(1):57-61.
6. Bellinger DH, Henny FA, Peterson LW. Fracture of the mandibular condyle. J Oral Surg. 1943;1:48-58.
7. Thoma KH. Fracture and dislocation of the mandibular condyle: method for treatment in 32 cases. J Oral Surg. 1945;3:3
8. Talwar RM, Ellis III E, Throckmorton GS. Adaptation of the masticatory system after bilateral fractures of the mandibular condyle process. J Oral Maxillofac Surg. 1998;56(4):430-9.
9. Kisnisci R. Management of fractures of the condyle, condylar neck, and coronoid process. Oral Maxillofac Surg Clin North Am. 2013;25(4):573-90
10. Choi KY, Yang JD, Chung HY, Cho BC. Current concepts in the mandibular condyle fracture management part II: open reduction versus closed reduction. Arch Plast Surg. 2012;39(4):301-8
11. Chrcanovic BR. Open versus closed reduction: diacapitular fractures of the mandibular condyle. Oral Maxillofac Surg. 2012;16(3):257-65.
12. Jing J, Han Y, Song Y, Wan Y. Surgical treatment on displaced and dislocated sagittal fractures of the mandibular condyle. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(6):693-9.
 Correspondence:
Correspondence:
Claiton Heitz
Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS)
Faculdade de Odontologia, Bloco 6, Av. Ipiranga, 6681
CEP 90616-900, Porto Alegre, RS, Brazil
E-mail: profheitz@hotmail.com
