










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.40 Canoas Jan./Jun. 2015
Natal and neonatal teeth: A report of three cases
Dentes natais e neonatais: relato de três casos
Ana Regina RomanoI; Marina Sousa AzevedoII; Andréia Drawanz HartwigIII; Carolina Camporese França-PintoIII; Maximiliano Sérgio CenciIV
I is PhD and associate professor, Department of Social and Preventive Dentistry, School of Dentistry, Universidade Federal de Pelotas (UFPel), Pelotas, RS, Brazil
II is doctoral student of Pediatric Dentistry, Department of Social and Preventive Dentistry, School of Dentistry, UFPel, Pelotas, RS, Brazil
III are MSc students of Pediatric Dentistry, Department of Social and Preventive Dentistry, School of Dentistry, UFPel, Pelotas, RS, Brazil
IV is PhD and associate Professor, Department of Operative Dentistry School of Dentistry, UFPel, Pelotas, RS, Brazil
ABSTRACT
The occurrence of natal and neonatal teeth is relativity rare. General dental practitioners should be aware of these conditions and be prepared to provide appropriate care for patients. The aim of this study is to describe two cases of neonatal teeth and one case of natal teeth, highlighting the importance of the treatment decision. In all of these cases the teeth were part of the normal series of primary dentition. In case 1 the tooth was extracted because of a possibility of aspiration. In cases 2 and 3 the teeth were monitored and parents were instructed about the necessary care, especially the need for good oral hygiene. In conclusion, each patient must be evaluated individually with radiographic and clinical examinations and the best treatment option should always be chosen taking into account parents' views.
Keywords: Natal teeth; Infant, Newborn; Tooth, Deciduous.
RESUMO
A ocorrência de dentes natais e neonatais é relativamente rara. Os cirurgiões-dentistas devem estar preparados para fornecer o cuidado adequado aos pacientes com essa condição. O objetivo deste estudo foi apresentar dois casos de dentes neonatais e um de dentes natais e destacar a importância da decisão do tratamento. Em todos os casos apresentados, os dentes faziam parte da série normal da dentição decídua. No caso 1 o dente foi extraído devido à possibilidade de aspiração. Nos casos 2 e 3, os dentes foram monitorados e os pais foram informados da necessidade de higiene bucal adequada. Concluindo, cada paciente deve ser avaliado individualmente através de exames clínicos e radiográficos. A escolha pela melhor opção de tratamento deve sempre levar em consideração a opinião dos pais.
Palavras-chave: Recém-Nascido; Dentes Natais; Recém-Nascido; Dente Decíduo.
INTRODUCTION
Congenital teeth, fetal teeth, predecidual teeth and dentition praecox are all terms that have been used for natal and neonatal teeth. Teeth present in the mouth at birth are called natal teeth while teeth that appear within the first 30 days of life are neonatal teeth 1. Incidence rates of natal and neonatal teeth range from 1 : 2,000 to 1 : 3,5002,3. According to Bondenhoff and Gorlim 4, 85% of these teeth are mandibular incisors (although they can also occur in other areas of the mouth), and the most common number of elements is one or two. Some authors report a predilection for females 5.
Only 1% to 10% of natal and neonatal teeth are supernumerary and more than 90% of natal and neonatal teeth are prematurely erupted elements of the deciduous series 1,2. Before the ideal treatment can be chosen, it is necessary to determine whether the tooth is supernumerary or part of the normal dentition. The most commonly recommended treatment is extraction and it is necessary to inform parents about all aspects involved in this situation. The decision to extract a natal and/or neonatal tooth should be evaluated on a case by case basis, taking into account scientific knowledge, clinical common sense, and parental opinion 1.
One common complication caused by natal/neonatal teeth is ulceration of the ventral surface of the tongue, caused by the sharp incisal edge of a tooth. This condition is also known as Riga-Fede disease 6. Other complications reported include injury to the mother's breast and inconvenience during breastfeeding. The possibility of swallowing and aspiration, which has been described previously, should also be a major concern. The baby's mother should be asked whether the tooth is causing injury to her breasts or to the baby's mouth. The degree of mobility and the presence of ulcerations in the child's mouth are other important clinical characteristics that should be considered during examination and taken into account before any treatment decisions are made.
The objective of this paper is to report on and discuss three cases of natal/ neonatal teeth in one female and two male children, describing the treatments and their consequences.
CASE REPORTS
Written informed consent was obtained from the mothers of all children before the first clinical examination.
Case 1
A 17-day-old male child was referred to the Department of Pediatric Dentistry at the Federal University of Pelotas for evaluation because of a neonatal mandibular right central incisor present in the oral cavity since 3 days of age (Figure 1A). The child's mother reported that she was born of a normal full term delivery with no complications and that there were no other similar cases in the family. On examination, the tooth was found to be very mobile, to the extent that its point of insertion could be seen when it was moved. The tooth had a milky white color and the surface of the enamel was rough. Ulcerations of the tongue or mucosa were not observed and the child's mother did not report any difficulties with breast feeding.
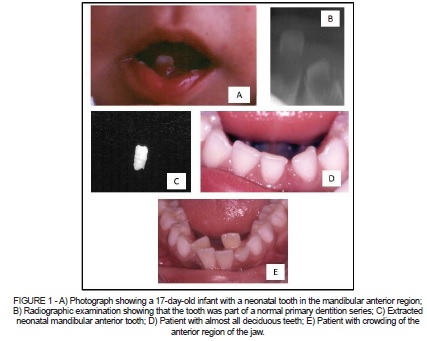
A radiograph was taken, showing that the tooth was part of the normal series of primary dentition (Figure 1B). The final diagnosis was a neonatal tooth.
The treatment initially proposed was conservative monitoring, but three days later the mobility of the tooth had increased further. The mother was told that there was a high risk of early exfoliation and she agreed to having the child's tooth extracted. Local anesthesia was administered with 0.3 ml of 2% lidostesim (Dentsply Pharmaceutical®, São Paulo, Brazil) and the tooth was removed with the aid of gauze and a syndesmotome (Figure 1C). There were no complications during the post-operative period.
The patient was monitored until eruption of his permanent central incisors. At age 7 crowding was observed in the anterior region of the jaw (Figure 1D, 1E), with the three mandibular central incisors taking the space of the four lower central incisors.
Case 2
A one-week-old male baby was brought to be examined in our clinic by his parents and two neonatal mandibular central incisors of normal size and color and little mobility were found on examination (Figure 2A). The teeth had been present since the boy was two days old and were therefore diagnosed as neonatal. Radiographic examination revealed that the teeth belonged to the normal series (Figure 2B). His mother reported that the teeth were not interfering with the breastfeeding process. It was decided that the teeth should be left in place and monitored. The mother was instructed to take special care with the baby's oral hygiene, to bring her child back for weekly follow-up appointments and to call if she had any concerns.
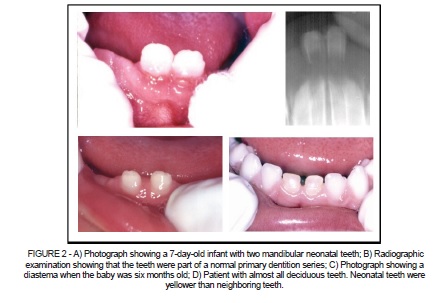
At all follow-up visits the mother reported no differences and no difficulties with the baby's hygiene or breast feeding and mobility was observed to decrease over time. The follow-up routine was then changed to monthly visits. At six months the baby's teeth had become yellowish and exhibited mobility and a diastema was present (Figure 2C). The child's mother reported that she had been following the recommended hygiene steps.
The patient was followed up to 2 years of age, when he had almost all of his deciduous teeth and so it was possible to compare the two neonatal teeth with their neighbors. The diastema had closed and the crowns were yellowish and a little shorter than the others (Figure 2D). They were, however, carrying out the functions of chewing and maintaining the spacing perfectly, thus contributing to the normal development of the arch.
Case 3
A female baby was brought to our clinic after pediatrician referral due to a natal mandibular left central incisor that was present from birth. Intraoral examination revealed a milky white color and an apparently unmineralized crown; the tooth also exhibited great mobility (Figure 3A). However, no ulcerations were observed in the mucosa or on the tongue.
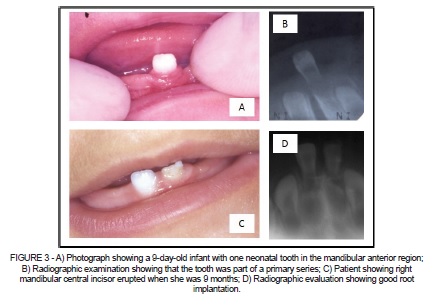
After clinical and radiographic examination, a diagnosis of a natal tooth from the deciduous series was reached and the tooth was monitored, with the mother's agreement (Figure 3B). She was also instructed with regard to oral hygiene practices.
When the baby girl was nine months old her right mandibular central incisor was of normal size and color. The left one was smaller and yellowish (Figure 3C, 3D).
DISCUSSION
The etiology of natal and neonatal teeth is still unknown 7. Superficial position of the germ, infection, malnutrition, febrile states, hormonal stimulation and hereditary transmission have been reported as causative factors 1. No common factors were identified as etiologic agents in the three cases reported here.
An association between this rare occurrence and certain systemic disorders has been observed, including congenital pachyonychia (Jadassohn-Levandowsky Syndrome), chondroectodermal dysplasia, occulo-mandibulo-dyscephaly with hypotrichosis and other problems such as cleft palate or lip 4,8. None of these disorders were observed in the cases reported here. A rare case of natal teeth associated with fibrous hyperplasia was reported recently. According to the authors, the development of reactive fibrous hyperplasia may be due to microtrauma caused by eruption of the tooth 9. All the natal and neonatal teeth described in this article were lower primary central incisors, which are the teeth most often involved. Natal and neonatal teeth generally erupt in the anterior mandibular area, but there are several reports of unusual sites of eruption. It has been observed that 85% of natal and neonatal teeth erupt in mandibular incisor positions, 11% in maxillary incisor positions, 3% in mandibular canine positions and 1% in maxillary canine and molar positions 10.
The clinical characteristics of the natal/neonatal teeth that were observed in this study included discoloration, smaller tooth size and poor or absent root development. These characteristics are common in other cases described in the literature 11 and other characteristics can also be seen, such as poor development, small size and conical shape, yellowish-brown or whitish opaque color, hypoplastic enamel or dentin, although these teeth can also occasionally be of normal size and shape.
Treatment should take into account whether the teeth are part of the normal series or are supernumerary, and radiographic examination is an essential auxiliary tool for differential diagnosis 1,11,12. When teeth are supernumerary, they should be extracted and when teeth are part of the normal dentition and considered mature, they should be preserved and maintained in healthy conditions in the baby's mouth using all available clinical resources 1.
The dentist should decide between tooth maintenance and extraction based on the aspects just mentioned. When maintenance of a natal tooth from the normal series is possible, this should be the first choice, because early removal of teeth may lead to over-crowding of permanent teeth. When maintenance is chosen, an assessment should be made of the need for grinding, smoothing the tooth surface or covering it with composite resin to prevent ulcerations of the baby's tongue or the mother's breasts. If the decision is taken to maintain a neonatal tooth, parents should be advised of the need for adequate dental hygiene and use of fluoride and periodical professional follow-up should be scheduled 1.
Some authors also warn of the need to be alert to the possibility of dislocation and consequent aspiration or swallowing of these teeth, because of the mobility that can be present. Other factors that should also be considered include the possibility of trauma to the child's oral tissues, such as ulceration of the ventral surface of the tongue, which is known as Riga-Fede disease 13, or of the opposing arch, or of the mother's breasts during feeding. Additionally, neonatal teeth are part of the differential diagnosis for ruling out other entities, such as Bohn's nodules 5.
When the treatment chosen is extraction, the risk of hemorrhage because of hypoprothrombinemia, commonly present in newborns, must be considered 1,11. Brendsen and Wakkerman 10 also warn of this risk if extractions are performed prior to 10 days of life and vitamin K is not administered. In most cases, these teeth are extracted with topical anesthesia, but removal of a neonatal tooth may be performed under general anesthesia in cases in which the infant has high fever and significant swelling with abscess formation which requires emergency drainage to provide respiratory clearance 10. Furthermore, it is necessary to ensure that the underlying papilla and Hertwig´s epithelial root sheath are removed by gentle curettage during extraction 14, since otherwise root development will continue.
Another situation that should be monitored is when a natal/neonatal tooth belonging to a normal series is extracted, which generally occurs before canine eruption, as happened in Case 1 described here. In such cases careful follow up is required because premature loss of this tooth can contribute to loss of arch space and could therefore cause crowding of the permanent dentition 15.
FINAL CONSIDERATIONS
Finally, each patient must be independently evaluated with radiographic examination and application of clinical judgment to decide on the best treatment, always taking into account parents' view, after they have been properly informed of all relevant aspects. Periodic follow-up to ensure preventive oral health care is always essential, irrespective of the treatment option chosen. The child should be referred to a pediatrician if there is suspicion of associated systemic disorders or syndromes.
REFERENCES
1. Cunha RF, Boer FA, Torriani DD, Frossard WT. Natal and neonatal teeth: review of the literature. Pediatr Dent. 2001;23:158-62. [ Links ]
2. El Khatib K, Abouchadi A, Nassih M, Rzin A, Jidal B, Danino A, et al. Natal teeth: apropos of five cases. Rev Stomatol Chir Maxillofac. 2005;106:325-7.
3. Dyment H, Anderson R, Humphrey J, Chase I. Residual neonatal teeth: a case report. J Can Dent Assoc. 2005;71:394-7.
4. Bodenhoff J, Gorlin RJ. Natal and neonatal teeth: folklore and fact. Pediatrics. 1963;32:1087-93.
5. Freudenberger S, Santos Díaz MA, Bravo JM, Sedano HO. Intraoral findings and other developmental conditions in Mexican neonates. J Dent Child. 2008;75:280-6.
6. Anegundi RT, Sudha R, Kaveri H, Sadanand K. Natal and neonatal teeth: a report of four cases. J Indian Soc Pedod Prev Dent. 2002;20:86-92.
7. Malki GA, Al-Badawi EA, Dahlan MA. Natal teeth: a case report and reappraisal. Case Rep Dent. 2015;2015:147580. Epub 2015 Feb 4.
8. Portela MB, Damasceno L, Primo LG. Unusual case of multiple natal teeth. J Clin Pediatr Dent. 2004;29:37-9.
9. Sethi HS, Munjal D, Dhingra R, Malik NS, Sidhu GK. Natal tooth associated with fibrous hyperplasia – a rare case report. J Clin Diagn Res. 2015;9:ZD18-9.
10. Kamboj M, Chougule RB. Neonatal tooth--how dangerous can it be? J Clin Pediatr Dent. 2009;34:59-60.
11. Basavanthappa NN, Kagathur U, Basavanthappa RN, Suryaprakash ST. Natal and neonatal teeth: a retrospective study of 15 cases. Eur J Dent. 2011;5:168-72.
12. Mhaske S, Yuwanati MB, Mhaske A, Ragavendra R, Kamath K, Saawarn S. Natal and neonatal teeth: an overview of the literature. ISRN Pediatr. 2013;18:562-9.
13. Hegde RJ. Sublingual traumatic ulceration due to neonatal teeth (Riga-Fede disease). J Indian Soc Pedod Prev Dent. 2005;23:51- 2.
14. Maheswari NU, Kumar BP, Karunakaran, Kumaran ST. "Early baby teeth": folklore and facts. J Pharm Bioallied Sci. 2012;4(Suppl 2):329-33.
15. Hebling J, Zuanon ACC, Vianna DR. Dente natal: a case of natal teeth. Odontol Clín. 1997;7:37-40.
 Correspondence:
Correspondence:
Marina Sousa Azevedo, Faculdade de Odontologia
Universidade Federal de Pelotas
Rua Gonçalves Chaves, 457, 5º andar
CEP 96015-560
Pelotas, RS, Brasil
e-mail: marinasazevedo@hotmail.com
