










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.40 Canoas Jan./Jun. 2015
Eruption cyst associated with tooth rotation on deciduous dentition: A case report
Cisto de erupção associado com giroversão dentária na dentição decídua: relato de caso
Patrícia Bernardes Gonçalves WeberI; Mariana Cezar IlhaII; Tássia Silvana BorgesIII; Henrique Castilhos RuschelIV; Paulo Floriani KramerIV; Simone Helena FerreiraV
I is a DDS from the School of Dentistry, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II is an MSc candidate (Pediatric Dentistry) at the School of Dentistry, ULBRA, Canoas, RS, Brazil
III is an MSc in Health Promotion from Universidade de Santa Cruz do Sul (UNISC), Santa Cruz do Sul, RS, Brazil, and a PhD candidate at the School of Dentistry, ULBRA, Canoas, RS, Brazil
IV are PhDs in Pediatric Dentistry from Universidade de São Paulo (USP), São Paulo, SP, Brazil, and associate professors at the School of Dentistry, ULBRA, Canoas, RS, Brazil
V is an MSc in Public Health from ULBRA, Canoas, RS, Brazil, and an associate professor at the School of Dentistry, ULBRA, Canoas, RS, Brazil
ABSTRACT
The eruption cyst is a benign soft tissue anomaly that may occur during eruption of deciduous or permanent teeth. It is usually asymptomatic and its treatment involves clinical follow-up of dental eruption. However, it may become infected or cause discomfort and pain. In such cases, surgical treatment is recommended. The present report aimed to describe a clinical case of eruption cyst located on the deciduous mandibular incisors' area of a four-month-old female infant since her birth. After surgical treatment a change was observed in the position (rotation) of the tooth associated with the cystic lesion. Rotation of the mandibular incisor persisted during the deciduous dentition development.
Keywords: Tooth Eruption; Odontogenic Cyst; Deciduous Tooth.
RESUMO
O cisto de erupção é uma anomalia benigna de tecidos moles que pode ocorrer durante a erupção dos dentes permanentes ou decíduos. Ele é geralmente assintomático e seu tratamento envolve acompanhamento clínico da erupção dental. No entanto, ele pode se tornar infectado ou causar desconforto e dor. Em tais casos, é recomendado tratamento cirúrgico. O presente relato teve como objetivo descrever um caso clínico de cisto de erupção localizado na área dos incisivos inferiores decíduos presente em um bebê de quatro meses de idade desde seu nascimento. Após o tratamento cirúrgico foi observada uma mudança na posição (rotação) do dente associado com a lesão cística. A rotação do incisivo inferior persistiu durante o desenvolvimento da dentição decídua.
Palavras-chave: Erupção Dentária; Cisto Odontogênico; Dente Decíduo.
INTRODUCTION
Throughout infancy, oral cavity disorders are characterized by events deriving from physiological responses, developmental alterations, and pathogeneses 1. An eruption cyst, classified as odontogenic cyst, is a developmental alteration that originates from the separation of the follicle that covers the crown of an erupting tooth due to the accumulation of fluid or blood in the dilated space 2,3.
Evidence indicates that eruption cysts may occur on both dentitions and are generally located on deciduous mandibular incisors and permanent first molars 1,2,4. Studies made on deciduous dentition demonstrate a low prevalence of the abovementioned alteration, which may vary from 1.0 to 1.8% 5,6.
From a histological perspective, an eruption cyst presents itself as an infiltration of inflammatory cells. The lining in the deepest portion consists of a thin layer of nonkeratinized pavimentous stratified epithelium 7. Similar microscopic characteristics may be found in dentigerous cysts: a fibrous connective tissue covered by a thin layer of nonkeratinized cell epithelium 2. The analysis of the cystic content may show the existence of cholesterol crystals with slightly yellowish color and low viscosity 8,9.
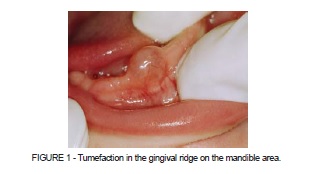
From a clinical perspective, an eruption cyst presents itself as a soft tumefaction in the mucosa of the ridge, dome-shaped, pitted on palpation, and with the translucent color of the gingival mucosa that covers the crown of the erupting tooth. The eruption cyst is usually asymptomatic and tends to present a spontaneous resolution without any type of treatment. However, when infected or traumatized it causes pain and discomfort on palpation. In case of symptomatic cyst or significant delay on dental eruption, surgical treatment should be considered 10,11.
The aim of this study is to describe a clinical case of eruption cyst on an infant since her birth. The case was associated with the rotation of the tooth affected by the cystic lesion.
CASE REPORT
A four-month-old female infant without systemic alterations was referred from a consultation at the university hospital to the pediatric clinic of the School of Dentistry of Universidade Luterana do Brasil, located in the city of Canoas, southern Brazil. The mother reported a volume increase on the anterior area of the ridge of the mandible since the birth of the infant. The baby presented irritation and discomfort during breastfeeding. After the introduction of the bottle, there was further increase of volume on the area.
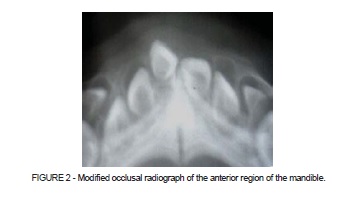
At physical examination, a soft tissue tumefaction was observed over the alveolar ridge on the anterior region of the mandible. It presented a pinkish color, similar to the adjacent oral mucosa (Figure 1). Radiographic evaluation was conducted through the modified occlusal technique using a 3x4 film (Figure 2). The preliminary diagnosis for the patient was eruption cyst.
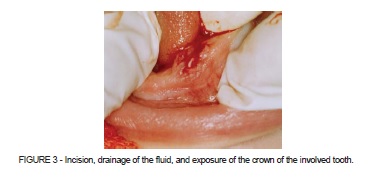
The treatment plan involved local surgical intervention and monitoring of the eruptive process. The intervention consisted of topical anesthesia (xylocaine 5%) and infiltration anesthesia (lidocaine 2% with vasoconstrictor). Following anesthesia, an incision was made using a scalpel blade number 15 in order to expose the crown of the affected tooth and drain the fluid from inside the cyst (Figure 3).
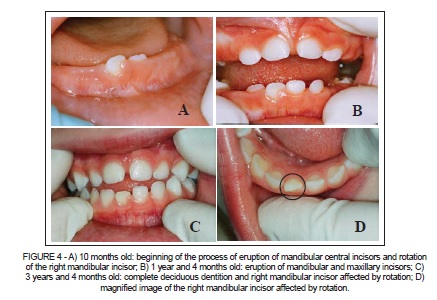
After a six-month period, when the patient was ten months of age, the beginning of the mandibular incisors' eruptive process and the rotation of the right mandibular incisor associated with the cystic lesion were observed (Figure 4A). Longitudinal follow-up showed the development of deciduous dentition and the change in the position of the deciduous incisor (Figure 4).
DISCUSSION
The etiopathogeny of eruption cysts involves theories that include degenerative changes in the reduced epithelium of the enamel organ, presence of reminiscences of the dental lamina, or presence and accumulation of fluid around the dental follicle 9,12.
This type of lesion is more frequent among children, although rarely observed in newborns, since the eruption of deciduous teeth begins in the sixth month of life 1,8. Gender predilection is controversial. Some authors suggest higher prevalence of eruption cysts among male individuals 4,10,11, while others do not observe difference in gender 1-3,8.
The cystic content may vary in color. It may have a pinkish (natural color of the gum) or bluish aspect (due to blood overflow in the follicular space, caused by trauma). Such characteristics are associated with eruption hematomas 4. Furthermore, eruption cysts are not identified through radiographs since they are located on soft tissues, with no bone involvement 2,4. Conversely, dentigerous cysts present a well-defined radiolucent area in a half-moon shape on the crown of the unerupted tooth 2,7.
In most cases the eruption cyst is asymptomatic, disappearing spontaneously once exposed to mastication 1,4,6,7,10. Conservative treatment may be performed, such as massaging the gum and using teethers to provide relief for the infant 1,6 as well as allowing the eruption of deciduous teeth to occur in a few months' time with the spontaneous disappearance of the lesion 10. However, if the cyst causes pain or discomfort on palpation, mastication, and breastfeeding, or if it is infected, surgical treatment should be indicated 1,10.
In the case presented in this study, there were reports of discomfort since birth and also damage to breastfeeding. Furthermore, introducing the bottle led to an exacerbation of the lesion, according to the parents. Surgical treatment consisted of an incision to drain the accumulated fluid and expose the crown of the involved tooth.
After surgical intervention, it was noticed that the deciduous mandibular incisor erupted affected by rotation. The lack of bone support, associated with the pressure resulting from the growth of the cystic lesion at an early stage of the mandibular incisor's formation, may have been responsible for the change in the position of the dental crown. In the consulted literature there are no reports of tooth rotation associated with eruption cysts. Rotation does not imply significant changes in patient's function, occlusion and aesthetic aspects. Clinical follow-up might be considered in these cases.
FINAL CONSIDERATIONS
Although they present low prevalence, eruption cysts may cause pain and discomfort in infants, in addition to changes in the dental eruption process. Early diagnosis may avoid changes in position or in the eruptive axis of the tooth as the cystic lesion grows. The rotation of the deciduous mandibular incisors may be one of the sequelae.
REFERENCES
1. Coser RM, Flávia FM, Melo BP, Quaglio JM. Características clínicas do cisto de erupção. Rev Gaucha Odontol. 2004;52:180-3. [ Links ]
2. Dhawan P, Khochhar GK, Chachra S, Advani S. Eruption cysts: a series of two cases. Dent Res J. 2012;9:647-50.
3. Neville BW, Damm DD, Allen CM, Bouquot JE. Patologia oral e maxilofacial. 2ª ed. Rio de Janeiro: Guanabarra Koogan; 2008. 569p.
4. Singh B, Bajaj P, Singh G. Presentation of two simultaneous eruption cysts haematomas in relation with two adjacent permanent teeth, causing tumour scare. Indian J Dent Sci. 2011;3:16-8.
5. Calvet CO, Quadros OS. Estudo da prevalência de cistos odontogênicos de desenvolvimento. Rev Facul Odontol Porto Alegre. 2002;43:8-14.
6. Baldani MH, Lopes CMDL, Scheidt WA. Prevalência de alterações bucais em crianças atendidas nas clínicas de bebês públicas de Ponta Grossa - PR, Brasil. Pesqui Odontol Bras. 2001;15:302-7.
7. Boj JR, Poirier C, Espasa E, Hernandez M, Jacobson B. Eruption cyst treated with a laser powered hydrokinetic system. J Clin Pediatr Dent. 2006;30:199-202.
8. Navas RMA, Mendoza MGM, Leonardo MR, Silva RAB, Herrera HW, Herrera HP. Congenital eruption cyst: a case report. Braz Dent J. 2010;21:259-62.
9. Bodner L, Goldstein J, Sarnat H. Eruption cyst: a clinical report of 24 new cases. J Clin Pediatr Dent. 2004;28:183-6.
10. Shaul H, Chatra L, Shenai P, Rao PK, Veena KM, Prabhu RV et al. Eruption cyst: a case report. Pac J Med Sci. 2013;11:34-8.
11. Zarakas M, Tsinidou K, Triantafyllou C, Megalogianni E, Tosios KI. Double eruption cyst in a newborn boy case report and review of the literature. Hell Arch Oral Maxilofac Surg. 2012;13:41-8.
12. Ricci HA, Parisotto TM, Giro EMA, Costa CAS, Hebling J. Eruption cysts in the neonate. J Clin Pediatr Dent. 2008;32:243-6.
 Correspondence:
Correspondence:
Tássia Silvana Borges
Rua Joana Machado, 103/302, Camobi
CEP 97105-180
Santa Maria, RS, Brasil
e-mail: tassia.s.borges@hotmail.com
