










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.40 Canoas Jan./Jun. 2015
Oral health policy of the city of Porto Alegre, southern Brazil: Analysis of the database of the Outpatient Information System of the Brazilian Unified Health System
Política de saúde bucal do Município de Porto Alegre: Análise do banco de dados do Sistema de Informações Ambulatoriais do SUS
Mariana Cezar IlhaI; Tássia Silvana BorgesII; Simone Loureiro Brum ImperatoreIII; Vania Regina Camargo FontanellaIV
I is MSc candidate at the Graduate Program in Dentistry, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II is PhD candidate at the Graduate Program in Dentistry, ULBRA, Canoas, RS, Brazil
III is professor at the Graduate Program in Dentistry and head of Community Affairs Bureau, ULBRA, Canoas, RS, Brazil
IV is professor at the Graduate Program in Dentistry, ULBRA, Canoas, RS, Brazil
ABSTRACT
Specifically for the dentistry field, the pact for health expresses the relevance of the process of evaluation and monitoring of primary care programs and services. The aim of the present study was to analyze the oral health poli cy of the city of Porto Alegre, Southern Brazil, in the context of the decentralization in health care implemented by the Brazilian Unified Health System (Sistema Único de Saúde, SUS), based on the database of the Outpatient Information System (Sistema de Informações Ambulatoriais, SIA). This descriptive, quantitative, normative/evaluative study analyzed secondary data from a historical series of dental procedures conducted in Porto Alegre and recorded by the SIA-SUS from 2008 to 2012. Data were collected directly from the SIA-SUS database. Data were also obtained from city's management reports from 2010 to 2013. Results show that the coverage of both Programmatic First Dental Consultation and Collective Supervised Toothbrushing Action was lower than that established in the pact.
Keywords: Health Promotion; Unified Health System; Oral Health.
RESUMO
Especificamente para o campo da odontologia, o pacto pela saúde expressa a relevância no processo de avaliação e monitoramento de programas e serviços da atenção básica. O objetivo do presente estudo foi analisar a políti ca de saúde bucal do município de Porto Alegre no contexto da descentralização da saúde implementada pelo Sis tema Único de Saúde (SUS), a partir do banco de dados do Sistema de Informações Ambulatoriais (SIA). Este estudo foi do tipo descritivo, quantitativo, de caráter avaliativo normativo, o qual utilizou dados secundários, a partir da série histórica da produção de procedimentos odontológicos realizados em Porto Alegre e registrados pelo SIA-SUS no período de 2008 a 2012. A coleta dos dados foi realizada diretamente no banco de dados do SIA-SUS. Dados também foram retirados dos relatórios de gestão do município nos anos de 2010 a 2013. Os resultados demonstram que tanto a cobertura da Primeira Consulta Odontológica Programática quanto a Ação Coletiva de Escovação Dental Supervisionada foram inferiores ao pactuado.
Palavras-chave: Promoção da Saúde; Sistema Único de Saúde; Saúde Bucal.
INTRODUCTION
In Brazil, one of the basic guidelines from the sanitary reform movement was the decentralization of the national health policy, embedded as one of the principles of what is known as Sistema Único de Saúde (SUS, which stands for Unified Health System) by both the 1988 Federal Constitution and the Law no. 8080 of 1990, which regulated SUS. The establishment of the Norma Operacional Básica do SUS (NOB SUS, SUS Basic Operational Norms) allowed for the consolidation of this policy, with the financing standardization and the process of decentralizing the management of services and actions in the scope of the system 1-3.
The NOB SUS is a set of ordinances from the Ministry of Health that aim to define guidelines and strategies for the decentralization of health policies and contribute to the standardization and operationalization of relations between spheres of government that are not covered by organic laws of health 4,5. It was also after the implementation of these ordinances that, in 1993, the states took on more complex functions on the management of information systems (among which was the Sistema de Informações Ambulatoriais do SUS (SIA-SUS, SUS Outpatient Information System) and on the development and supervision of the physical and budget schedule for outpatient services to be presented to the Ministry of Health for payment 6. The actions are monitored according to the information supplied by municipalities through the SIA-SUS, and resources are passed directly from the Ministry of Health to the municipalities.
SpecifIcally for the dentistry field, the pact for health expresses the relevance of the process of assessment and monitoring of services and programs of primary health care 7. It includes oral health indicators, such as estimated population covered by the oral health teams of the Brazil's Family Health Strategy (Estratégia de Saúde da Família, ESF) and average reach of the Collective Supervised Toothbrushing Action 8. Efforts to reorganize oral health care have been made since 2004, when the Política Nacional de Saúde Bucal (National Oral Health Policy) was redesigned 9.
Regardless of the major changes that are suggested, primary oral health care services provided in Brazil have been little studied. One of the objectives of dentistry is to promote adequate levels of oral health for the entire population of a country, an area, or a place 5. Over the last few decades, the field of dentistry has achieved a high level of scientific and technological development, being able to solve oral health problems in developed countries. However, Brazil still lacks a well-defined oral health policy, and significant parts of the population have no access to essential clinical and preventive care on a regular basis 10.
This study aimed to analyze the oral health policy of the Municipality of Porto Alegre in the context of the decentralization in health care implemented by the SUS, using the SIA-SUS database for this purpose.
METHODOLOGY
This descriptive, quantitative, evaluative-normative study used secondary data from the historic series of dental procedures (number of procedures) carried out in Porto Alegre and registered by the SIA-SUS from 2008 to 2012. The data were collected directly from the SIA-SUS database. Selection, survey, organization, and analysis of secondary data on oral health production were carried out. Data were also collected from Porto Alegre's management reports from 2010 to 2013.
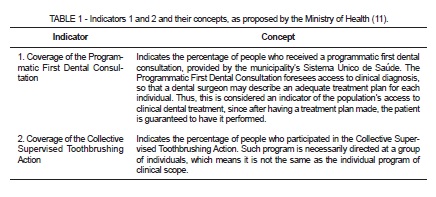
The 2010 Management Report of the oral health technical area from the Municipal Department of Health of Porto Alegre was prepared based on the figures obtained from five indicators suggested by the Ministry of Health to evaluate municipalities. Such figures were analyzed and compared to the goals that were agreed with the State Department of Health of Rio Grande do Sul in previous years. They are as follows: 1) Coverage of Programmatic First Dental Consultation; 2) Coverage of Collective Supervised Toothbrushing Action; 3) Average of Individual Basic Dental Procedures; 4) Rate of Specialized Dental Procedures in Relation to Individual Dental Actions; and 5) Rate of Extractions in Relation to Individual Basic Dental Actions. This article covers indicators 1 and 2, which are defined in Table 1.
The management report is divided by district administrations (GD, gerências distritais), which cover the following regions and neighborhoods: GDC - Centro; GDLN - Leste Nordeste; GDSCS - Sul/Centro Sul; GDGCC - Glória, Cruzeiro e Cristal; GDNEB - Norte Eixo Baltazar; GDPLP - Partenon Lomba do Pinheiro; GDNHNI - Noroeste Humaitá, Navegantes e Ilhas; and GDRES - Restinga.
Data concerning the coverage of the ESF and ESF com Saúde Bucal (SB, Oral Health) (ESF/SB) programs were also collected. Data are presented and computed as demonstrated in Table 2.

RESULTS
Table 3 shows results for the population of Porto Alegre, including population covered by the ESF, and the ESF/SB, and oral health teams from 2008 to 2012, according to data collected from SIA-SUS. Throughout the years, there was an increase in the population covered by the ESF and the ESF/SB.
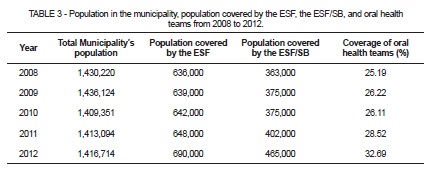
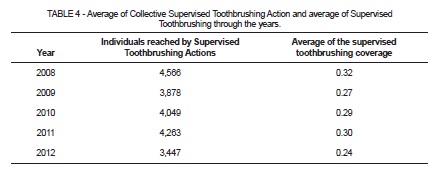
Table 4 displays data related to the reach (in number of individuals) of the Collective Supervised Toothbrushing Action and average of supervised toothbrushing from 2008 to 2012 when divided by the number of actions. Collective actions in the year 2008 reached the highest number of individuals; conversely, 2012 had the lowest number, as well as a lower average of oral health collective procedures.
Data concerning the coverage of Programmatic First Dental Consultation collected from the Porto Alegre 2010 management report are presented in Table 5. The goal agreed in 2008 suggested that municipalities offered a yearly programmatic dental consultation (and related treatment) for at least 12.5% of its population. It is noticeable that the values for the years 2008, 2009, and 2010 fall short of the intended goal.
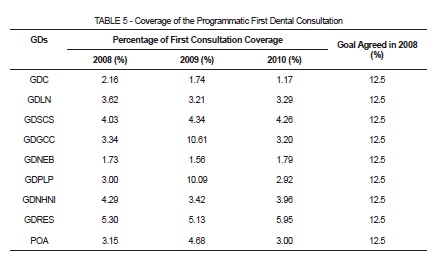
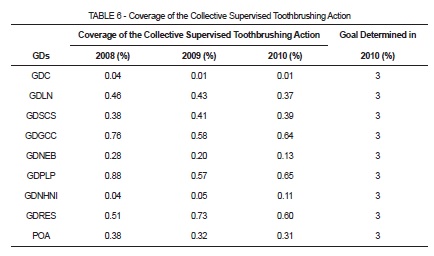
Table 6 lists the coverage of the Collective Supervised Toothbrushing Action from 2008 to 2010, highlighting that none of the district administrations reached the goal determined in 2010 during all of the timeframes evaluated.
DISCUSSION
Although the population from Porto Alegre fluctuated from 2008 to 2012, it is noticeable that the population covered by the ESF increased significantly. Likewise, the population covered by the ESF/SB increased. Nevertheless, coverage of oral health teams remains at 32%, which is considered low. Such limited coverage is also observed in the percentage of first consultations for the year studied.
Oral health teams are formed by dental assistants and dentists. The presence of an oral team within the ESF had better chances of creating a connection with the users, and consequently performing longitudinal care 8-10,12-15. Such connection may contribute to the increase in programmatic consultations and the accomplishment of the principle of integrality in care.
In 2009, there was an increase in programmatic consultations in Porto Alegre as a whole. However, the agreement over such consultations was based on a maximum number of three consultations per patient, regardless of the necessary number of procedures. In order to complete a given treatment, the same patient had to have another programmatic consultation, until all his/her needs had been met; this generated a repeated registry 16.
In addition to that, data from initial consultations might have been undercounted. The training of ESF teams aims at proper documentation of consultations, creating reliable data that may be compared to the reality faced by the local population 16.
The numbers regarding the coverage of the Collective Supervised Toothbrushing Action were way below the goal established for 2010. This may result largely from undercounted records, since the reading of the calculation method for this indicator usually raises many doubts among professionals. Nevertheless, the need for expanding both preventive actions and oral health promotion actions is clear 17.
This indicator also helps monitoring the population's level of access to collective actions to prevent oral diseases and estimates the proportion of people who had access to the topical fluoride in the toothpaste – assuming that most places that participate in the Collective Supervised Toothbrushing Action use fluoride toothpaste 11.
This action is extremely important because it focuses on maintaining health rather than treating diseases. Additionally, it targets people who do not have any diseases that require surgical intervention and should be performed at a collective level by any professional who works in primary health care 7. It is also a low cost action, requiring only toothbrush and toothpaste besides human resources.
Preventive actions of collective nature are key to promote oral health and educate people of different age groups. The relation between the number of dental surgeons and oral health technicians determines the service profile of a unit. When there is a greater presence of dental surgeons, the tendency is to have a higher number of restorative and surgical procedures. However, isolated procedures do not guarantee that the citizens are thoroughly included in oral health.
There are many challenges to overcome, especially regarding the integration of all parts involved in oral health care. It is imperative that a large group of stakeholders with singular responsibilities cooperate. The oral health care system needs them to fulfill their responsibilities, cooperate, and articulate 18.
Difficulties may be related to a tendency to keep the biomedical model, which is centered on the disease, and attempts to address the suppressed demand of a population who did not have access to oral health services through programs and projects 19,20.
Further research would be essential especially on topics such as implementation and effectiveness of quality assessments for services and care performed both individually and collectively. Moreover, it would be interesting to investigate the satisfaction level of the users and the reasons why they utilize oral health services.
CONCLUSION
The ESF/SB coverage presented a slow and gradual improvement throughout the observed period. In contrast, there was a decrease in the average supervised toothbrushing coverage. The coverage of both the Programmatic First Dental Consultation and the Collective Supervised Toothbrushing Action fell short of the established goals. Such results should be carefully analyzed, considering the previously exposed limitations of the indicators.
REFERENCES
1. Scatena JHG. Avaliação da descentralização da assistência à saúde no Estado de Mato Grosso [tese de doutorado]. São Paulo: Universidade de São Paulo; 2000.
2. Lesbaupin I. Poder local x exclusão social: a experiência das prefeituras democráticas no Brasil. Petrópolis: Vozes; 2000.
3. Oliva-Augusto MH, Costa OV. Entre o público e o privado: a saúde hoje no Brasil. Tempo Soc. 2000;1:199-217.
4. Brasil, Ministério da Saúde. Portaria nº 545 de 20 de Maio de 1993. Estabelece normas e procedimentos reguladores do processo de descentralização da gestão das ações e serviços de saúde, através da norma operacional Básica – SUS 01/93. Brasília, 1993.
5. Volpato LER, Scatena JH. Análise da política de saúde bucal do Município de Cuiabá, Estado de Mato Grosso, Brasil, a partir do banco de dados do Sistema de Informações Ambulatoriais do Sistema Único de Saúde (SIA-SUS). Epidemiol Serv Saude. 2006;15:47-55.
6. Levcovittz E, Lima LD, Machado CV. Política de saúde nos anos 90: relações intergovernamentais e o papel das Normas Operacionais Básicas. Cienc Saude Coletiva. 2001;6:269-91.
7. Bordin D, Fadel CB. Pacto pela Saúde no Brasil: uma análise descritiva da progressão dos Indicadores de Saúde Bucal. Rev-Odontol UNESP. 2012;41:305-11.
8. Brasil, Ministério da Saúde. Portaria nº 3.840. Inclui a Saúde Bucal no Monitoramento e Avaliação do Pacto pela Saúde, e estabelece as diretrizes, orientações e prazos do processo de ajuste de metas para o ano de 2011. Brasília, 2010.
9. Brasil, Ministério da Saúde, Coordenação Nacional de Saúde Bucal, Departamento de Atenção Básica, Secretaria de Atenção à Saúde. Diretrizes da política nacional de saúde bucal. Available from: http://bvsms.saude.gov. br/bvs/publicacoes/politica_nacional_ brasil_sor ridente.pdf
10. Pinto VG. Saúde bucal coletiva. 4ª ed. São Paulo: Santos; 2000.
11. Brasil, Ministério da Saúde. Orientações acerca dos indicadores de monitoramento avaliação do pacto pela saúde, nos componentes pela vida e de gestão para o biênio 2010- 2011. Conforme Portaria GM/MS nº 2669, de 03 de novembro de 2009 e Portaria GM/S nº 3.840, de 07 de dezembro de 2010. Brasília, 2011.
12. Cadastro Nacional de Estabelecimentos de Saúde (CNES). Available from: <http:// tabnet.datasus.gov.br/cgi/pacto/2013mon/Nota_Tecnica_Valores_absolutos.pdf>. Acesso em: 28/03/2015.
13. Sistema de Informação Ambulatorial (SIA-SUS). Available from: <http://189.28.128.100/ dab/docs/geral/nota_indicador_escovacao.pdf>. Acesso em: 28/03/2015.
14. Instituto Brasileiro de Geografia e Estatística. Available from: <http://www.ibge.gov. br/home/estatistica/populacao/censo2010/indicadores_sociais_municipais/indicadores_ sociais_municipais_tab_pdf.shtm>.
15. Brasil, Ministério da Saúde, Departamento de Atenção Básica, Secretaria de Atenção à Saúde. Política nacional de atenção básica. http://bvsms.saude.gov. br/bvs/saudelegis/ gm/2011/prt2488_21_10_2011.
16. Barros SG, Chaves SLA. Utilização do Sistema de informações Ambulatoriais (SIASUS) com instrumento para caracterização das ações de saúde bucal. Epidemiol Serv Saude. 2003;12:41-51.
17. Almeida GCM, Ferreira MAF. Saúde bucal no contexto do Programa de Saúde da Família: práticas de prevenção orientadas ao indivíduo e ao coletivo. Cad Saude Publica. 2008;24:2031-140.
18. Godoi H, Ferreira de Mello ALS, Caetano JC. Rede de atenção à saúde bucal: organização em municípios de grande porte de Santa Catarina, Brasil. Cad Saude Publica. 2014;30:318-32.
19. Aquilante AG, Aciole GG. Construindo um "Brasil Sorridente"? Olhares sobre a implementação da Política Nacional de Saúde Bucal numa região de saúde do interior paulista. Cad Saude Publica. 2015;31:82-9.
20. Leake JL, Birch S. Public policy and the market for dental services. Community Dent Oral Epidemiol. 2008;36:287-95.
 Correspondence:
Correspondence:
Mariana Cezar Ilha
Av. Farroupilha, 8001, Bairro São José
CEP 92425-900, Canoas, RS, Brasil
e-mail: marianacilha@outlook.com
