










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.21 no.41 Canoas Jul./Dez. 2015
Endodontic retreatment: Analysis of three specialists' retreatment rates
Retratamento endodôntico: avaliação dos índices de três especialistas
Gustavo Golgo Kunert I; Itaborai Revoredo Kunert II; Caroline Solda III; Marina Canali Lângaro III; Alessandra Nunes Machado III; Fernando Branco BarlettaIV
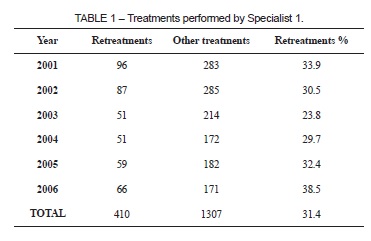
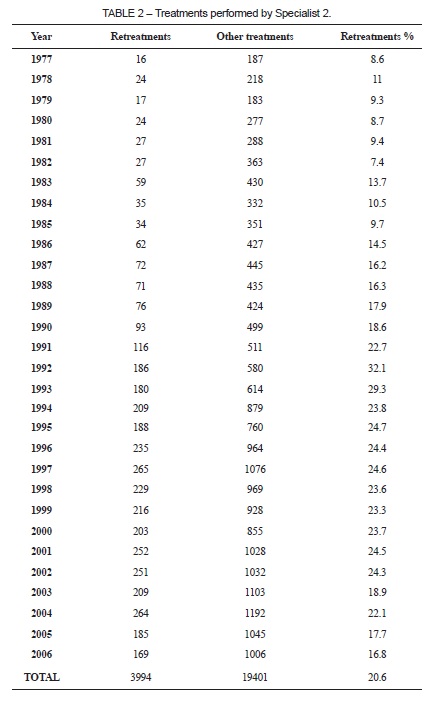
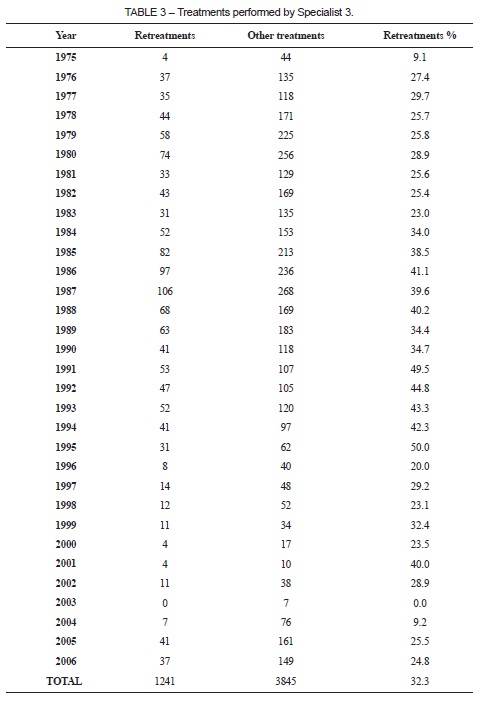
I PhD in Endodontics from Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil The authors have no conflicts of interest to declare concerning the publication of this manuscript ABSTRACT Endodontic retreatment is a clinical intervention intended to correct errors that have occurred in a treatment performed previously. There are several causes of failures. The anatomical variations between root canals and the difficulties of achieving microbial disinfection are reported as two of the main causes. However, in the dental offices of both general practitioners and specialists, it is very common that the causes of indications for endodontic retreatment are technical failures due to poorly executed treatment. In view of this, the objective of this study is to analyze the records of three specialists in Endodontics and analyze the causes for referral of their endodontic retreatment patients. Examination of 24,553 treatments conducted over varying periods revealed that cases of retreatment accounted for a considerable proportion of the routine work performed by these specialists, at an average of 23% of cases. The majority of retreatment indications were due to technical failure of the initial treatment, in combination with microbial factors caused by contamination of coronal restorations and poorly executed endodontic preparation and filling. Keywords: Endodontics; Root Canal; Retreatment; Preparation of the canal. RESUMO O retratamento endodôntico é uma intervenção clínica destinada para a correção de falhas ocorridas num tratamento anteriormente realizado. Vários são os motivos desencadeadores de insucessos. A variedade anatômica dos canais radiculares e a dificuldade de proporcionar a desinfecção microbiana são referenciadas como duas das causas principais. Entretanto, nos consultórios dentários de clínicos gerais e especialistas, é muito comum a indicação para o retratamento endodôntico por razões técnicas devido a sua mal execução. Estabelecida esta problemática, o objetivo deste estudo consiste em avaliar os prontuários de três especialistas em endodontia e verificar quais são os motivos de encaminhamentos de seus pacientes para o retratamento endodôntico. Após o exame de 24.553 tratamentos em períodos distintos, verificouse que os casos de retratamentos chegam a uma média relevante de 23% na rotina destes especialistas e que a maioria das indicações se deram por inabilidade no primeiro tratamento, aliadas ao fator microbiano causado por contaminações de restaurações coronárias, preparos e obturações endodônticas mal executadas. Palavras-chave: Endodontia; Canal Radicular; Retratamento; Preparo do Canal. INTRODUCTION Despite technical and scientific advances in endodontics and high success rates, in addition to the gradual increase of the number of specialists in the market, significant numbers of cases requiring retreatment can still be observed in dental offices 1-3. This situation raises questions about the true causes of retreatment. It is known that endodontic treatments in vital pulp achieve success rates higher than 90% when well executed. However, when periradicular lesions are present, the rate is around 86% 4. Furthermore, studies such as one conducted by Chugal et al. 5 have reported differences in success rates between cases with pulpitis and with pulp necrosis, reporting prognoses of 89.7 and 69.7%, respectively. Probable causes of failure include the following: large anatomical variations, calcification, isthmuses, lateral canals 6, intra and extra-root microbial factors 7, and systemic complications. These can greatly complicate treatment and are important factors in the failure of endodontic treatment and retreatment. Notwithstanding, retreatment of the root canal remains the first option in cases of failure of an earlier treatment. According to Simsek et al. 8 clinical success rates can vary from 50 to 90%. In view of this, identification of the factors that lead to failure is of fundamental importance to establishing the ideal conduct for endodontic treatment. The objective of retreatment is to adopt the same principles as in primary treatment, i.e. disinfection and shaping followed by hermetic sealing with filling material and adequate coronal restorative treatment, in order to accomplish a successful repair. Against this background, the aim of this study was to conduct a survey of endodontic treatment and retreatment rates in data from three specialists in endodontics, evaluating the causes of failure of these procedures. METHODOLOGY The private records of two specialists in Endodontics from Rio Grande do Sul and one specialist from São Paulo, both in Brazil, were analyzed for this study. Cases were selected on the basis of the initial clinical evaluation and periapical radiographs, according to the following criteria: Retreatment group: patients diagnosed with conditions requiring endodontic retreatment. For this group we evaluated the quality of the endodontic treatment and restoration performed previously. This group included the clinical cases of patients with or without apical periodontitis observable in the initial radiographic examinations. Other Treatments group: patients diagnosed with conditions requiring endodontic treatment of live or necrotic pulp. This group also included clinical cases of pulp necrosis, with or without periapical lesions observable in the initial radiographic examination. These data were stored in an Excel® spreadsheet, listed by annual totals. First, for each specialist we calculated their individual rate of Retreatments as a percentage of Other Treatments (live or necrotic pulp) (Tables 1, 2 and 3). We then summed the results for all three specialists and calculated the overall percentage of retreatments. These data, referred to as the general total were given by calculating the total of the 3 Retreatments groups as a percentage of the total of the three Other Treatments groups. RESULTS In the case of the first specialist, analysis of his records for the period from 2001 to 2006 revealed a total of 1,307 treatments performed (Table 1). The second specialist's records covered a period from 1977 to 2009, during which a total of 19,401 treatments were performed (Table 2). Finally, the third specialist's records showed that 3,845 treatments had been performed during the period from 1975 to 2006 (Table 3). In the general analysis, summing the figures for all three specialists' work resulted in a total of 24,553 treatments performed. Of these, 18,908 (77%) cases were indicated for initial treatment of vital or necrotic pulp and 5,645 (23%) were indicated for endodontic retreatment It was observed from these data that Specialist 1's retreatment percentage was 31.4% over a 6-year period (Table 1), Specialist 2's retreatment percentage was 20.6% over a period of 29 years (Table 2) and Specialist 3's retreatment percentage was 32.3% over a 31-year period (Table 3). Taking the overall results obtained by summing the results of all three specialists resulted in an average of 23% of treatments conducted because of a need to perform endodontic retreatment, diagnosed as poorly treated canals. DISCUSSION Endodontic retreatment is the first option in cases of endodontic failure, that is to say, teeth with clinical and radiographic manifestations of disease and/or symptoms of pain after initial treatment can be preserved in the oral cavity if retreatment is more effective than the original attempt 8. According to data from the Conselho Regional de Odontologia do Rio Grande do Sul (Rio Grande do Sul Regional Board of Dentistry), in 2015 the number of Endodontic specialists totals 874 professionals 9. In São Paulo this figure is even higher at 3,381 specialists 10. At the national level, in the same year, the Brazilian Federal Board of Dentistry has 13,557 professionals registered as specialists in Endodontics 11. One of the factors that we question in this study is the incompatibility between the increase in the number of specialists over the last 20 years and the persistence of poorly treated canals observed in daily routines. Proof of this is the rate of endodontic retreatment observed in this study, which was 23% across the three specialists analyzed over varying periods up to 2006. Some authors 2,12-15 attribute the reasons for the rate of ineffective endodontic treatment, when canals are well treated, to anatomical and microbial factors. We agree with these reports, but we find it of particular interest that these causes were at a fairly low level in our results, accounting for less than 3%. Indeed, of 24,553 treatments evaluated, the majority of failures (totaling 23% of cases seen at the clinics) were in poorly treated canals, combined with the microbial factor, which itself is the result of professional failure in conducting coronary restorations or poorly preparing and filling canals. According to Song et al 16, the main factors influencing failure of endodontic therapy are leakage through the filling material (30.4%); canals not located and therefore not treated (19.7%); insufficient fillings (14.2%); overfills (3.0%); anatomical complexity (8.7%); iatrogenic problems (2.8%); apical calcifications (1.8%) and cracks (1.2%). Bergenholtz et al. 17 also state that the causes of failure of endodontic treatments are largely due to professional negligence, in which the specialist did not correctly follow the mechanical and biological principles governing endodontic treatment. In addition to these factors, several epidemiological studies have demonstrated a high percentage of failure when root canals are treated by general practitioners. They exhibit distinctly lower success rates, at approximately 24 to 66% (18-20), compared to the success rates of treatments performed by specialists or by supervised students (70 to 95%), depending on the periapical pathology involved 21. Interpretation of the results of that study paints a disturbing picture, which is due to poorly executed canals, often treated by general practitioners 21. This issue does not appear to be restricted to Brazil, since Dugas et al. 20 and Ilić et al. 22 reported the same problem in studies conducted in Canada and Serbia respectively, where they observed high failure rates due to poorly executed endodontic and restorative treatment. The results obtained from the three specialists in Endodontics analyzed in this study show that 5,645 (23%) of their cases were the result of indications for retreatment. After retreatments performed by the three specialists analyzed in this study, their failure rates were lower, which data are in agreement with studies by Bergenholtz et al. 17 and Chevigny et al. 23, who reported successful retreatment of teeth whose canals had been inadequately filled initially. These data are similar to a systematic review by Torabinejad et al. 24, who reported a success rate of 83% in cases of retreatment after 6 years of follow-up. In view of the above, we do not question the preparation of the schools of Dentistry or of the specialization courses, which have significantly increased in number in Brazil. However, our results indicate a need for reflection. Our goal is not to generalize to all practitioners, but to propose a thorough self-assessment to those who practice this specialty. What should be done? The results show a high percentage of failures because of poor execution of endodontic treatment. Although there was a significant difference in the number of cases treated over the years by the three different specialists, it was observed that the rates of retreatments referred to their clinics were similar for two of these professionals, irrespective of period (31.4; 32.3%). Our question is about the quality of treatment in relation to the significant increase in number of specialists: why are canals still being treated negligently by fellow professionals? We could point out that, in Table 1, covering the years from 2000 to 2006, retreatment rates remained high, at an average of 31.4%. The same fact can be observed in Table 2, with data starting in the 1970s, and Table 3, from the 1970s to 2006, with a slight decline since the turn of the century. Unfortunately, over the years analyzed in this study, the significant reduction in retreatment rates that might be expected, considering the significant annual increase in specialists entering the market, has not been observed. We do not want, through this survey, to modify the principles governing endodontic therapy, rather to emphasize that it is important for professionals to reflect on the execution of their clinical practice and to prioritize an attitude of respect for patients' dignity. Rawski et al. 25 and Estrela et al. 2 have already stated that various factors, such as the cognitive, evaluation of clinical context and preparation of a treatment plan also contribute to the success or failure of endodontic therapy. It is of collective interest that dentists perform the various different specialties with appreciation, dedication and competence, without diverging from the principles that govern them. However, it is a principle of ethics and of respect for the patient that Dental professionals conduct their work in accordance with their individual limits of performance. CONCLUSIONS The average rates in a total of 24,553 clinical cases treated by three specialists were 77% for initial endodontic treatments and 23% for retreatments. Despite the increasing number of specialists in the market, the high percentage of retreatments (23%) is still striking. Most indications for retreatment were due to poorly treated canals, combined with the microbial factor, caused by contamination of poorly executed coronary restorations, endodontic preparations and fillings. Practice of Endodontics must be accompanied by a thorough knowledge of dental anatomy, professional qualification and training. REFERENCES 1. Barletta FB, Rahde NeM, Limongi O, Moura AA, Zanesco C, Mazocatto G. In vitro comparative analysis of 2 mechanical techniques for removing gutta-percha during retreatment. J Can Dent Assoc. 2007;73:65-65E. [ Links ] 2. Estrela C, Holland R, Estrela CR, Alencar AH, Sousa-Neto MD, Pécora JD. Characterization of successful root canal treatment. Braz Dent J. 2014;25:3-11. 3. Estrela C, Guedes OA, Silva JA, Leles CR, Estrela CR, Pécora JD. Diagnostic and clinical factors associated with pulpal and periapical pain. Braz Dent J. 2011;22:306-11. 4. Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:86-93. 5. Chugal NM, Clive JM, Spångberg LS. A prognostic model for assessment of the outcome of endodontic treatment: Effect of biologic and diagnostic variables. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:342-52. 6. Ricucci D, Loghin S, Siqueira JF. Exuberant Biofilm infection in a lateral canal as the cause of short-term endodontic treatment failure: report of a case. J Endod. 2013;39:712-8. 7. Rôças IN, Alves FR, Santos AL, Rosado AS, Siqueira JF. Apical root canal microbiota as determined by reverse-capture checkerboard analysis of cryogenically ground root samples from teeth with apical periodontitis. J Endod. 2010;36:1617-21. 8. Simsek N, Keles A, Ahmetoglu F, Ocak MS, Yologlu S. Comparison of different retreatment techniques and root canal sealers: a scanning electron microscopic study. Braz Oral Res. 2014;28:1-7. 9. Conselho Regional de Odontologia do Rio Grande do Sul – CRO/RS. Dados Estatísticos. Disponível em: http://www.crors.org.br/ 10. Conselho Regional de Odontologia de São Paulo – CRO/SP. Dados Estatísticos. Disponível em: http://www.crosp.org.br/ 11. Conselho Federal de Odontologia – CFO/Brasil. Dados Estatísticos. Disponível em: http://cfo.org.br/ 12. Siqueira JF. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34:1-10. 13. Nair PN, Sjögren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. J Endod. 1990;16:580-8. 14. Vera J, Siqueira JF, Ricucci D, Loghin S, Fernández N, Flores B, et al. One- versus two-visit endodontic treatment of teeth with apical periodontitis: a histobacteriologic study. J Endod. 2012;38:1040-52. 15. Ricucci D, Siqueira JF. Recurrent apical periodontitis and late endodontic treatment failure related to coronal leakage: a case report. J Endod. 2011;37:1171-5. 16. Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod. 2011;37:1516-9. 17. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjö B, Engström B. Retreatment of endodontic fillings. Scand J Dent Res. 1979;87:217-24. 18. Asgary S, Eghbal MJ, Ghoddusi J. Two-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter randomized clinical trial. Clin Oral Investig. 2014;18:635-41. 19. Siqueira JF, Rôças IN, Riche FN, Provenzano JC. Clinical outcome of the endodontic treatment of teeth with apical periodontitis using an antimicrobial protocol. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:757-62. 20. Dugas NN, Lawrence HP, Teplitsky PE, Pharoah MJ, Friedman S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J. 2003;36:181-92. 21. Masiero AV, Barletta FB. Effectiveness of different techniques for removing guttapercha during retreatment. Int Endod J. 2005;38:2-7. 22. Ilić J VM, tihaček-šojić L, Milić-lemić A.Frequency and quality of root canal fillings in an adult Serbian population. Srp Arh Celok Lek. 2014;142:663-8. 23. de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study--phase 4: initial treatment. J Endod. 2008;34:258-63. 24. Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009;35:930-7. 25. Rawski AA, Brehmer B, Knutsson K, Petersson K, Reit C, Rohlin M. The major factors that influence endodontic retreatment decisions. Swed Dent J. 2003;27:23-9.
II board-certified in Endodontics by Conselho Federal de Odontologia, Brazil
III MSc candidates in Endodontics at the School of Dentistry of Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
IV PhD in Endodontics from the School of Dentistry of Universidade de São Paulo, São Paulo, SP, Brazil
 Correspondence:
Correspondence:
Gustavo Golgo Kunert
Rua Florêncio Ygartua, 271/201
Porto Alegre, RS, Brazil
e-mail: gustavogkunert@gmail.com
