










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.22 no.42 Canoas Jan./Jun. 2016
Benzodiazepines for conscious sedation in the dental office
Utilização de benzodiazepínicos para obtenção de sedação consciente no ambiente odontológico
Theodoro Weissheimer I; Alexandre da Silveira Gerzson II; Henderson Eduarth Schwengber III; Angelo Menuci Neto IV
I dental student at Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II PhD in Oral and Maxillofacial Surgery and Traumatology from Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil; MSc and board-certified in Oral and Maxillofacial Surgery and Traumatology from/by Universidade Sagrado Coração (USC), Bauru, SP, Brazil; board-certified in Implantodontics by Associação Brasileira de Odontologia do Rio Grande do Sul (ABORS), Porto Alegre, RS, Brazil; and professor at School of Dentistry, ULBRA, Canoas, RS, Brazil
III board-certified in Psychiatry and Forensic Psychiatry by Associação Brasileira de Psiquiatria, Rio de Janeiro, RJ, Brazil; psychiatrist (residency in Psychiatry at Escola de Saúde Pública do Estado do Rio Grande do Sul/Hospital Psiquiátrico São Pedro, Porto Alegre, RS, Brazil) and forensic psychiatrist at Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA) and Instituto Psiquiátrico Forense Doutor Maurício Cardoso, Porto Alegre, RS
IV board-certified in Oral and Maxillofacial Surgery and Traumatology by PUCRS, Porto Alegre, RS, Brazil; and MSc in Implantodontics from USC, Bauru, SP, Brazil
The authors have no conflicts of interest to declare concerning the publication of this manuscript.
ABSTRACT
Conventional behavioral conditioning techniques are usually sufficient for management of patients with fear and anxiety during dental treatment. When such techniques do not produce the expected results, dental anxiety can be managed using drug-based treatments known as conscious sedation. Anxiety can complicate dental procedures because of effects such as increased blood pressure, hyperventilation, and fainting. Medications such as benzodiazepines can be used to avoid these complications. When used properly, dental procedures are safer and there are fewer difficulties for both patient and clinician. These drugs' mechanisms of action are exerted on the central nervous system and ultimately result in depression of excitatory cells. Effects vary, depending on the dose administered and the drug used, and can include sedation, hypnosis, muscle relaxation, anticonvulsant effects, coronary dilation, and neuromuscular blockade. With wide safety margins and few contraindications, the benzodiazepines most commonly used by dentists are diazepam, as a mild sedation-inducing anxiolytic, midazolam, to induce sleep and amnesia, and alprazolam, lorazepam, and triazolam, each with their appropriate properties and preferred dosages. This literature review allows us to conclude that benzodiazepines are an effective therapeutic option for management of patients with anxiety during dental treatment and are available for use in both inpatient and outpatient settings.
Keywords: Conscious sedation; Benzodiazepines; Dental anxiety.
RESUMO
As técnicas convencionais de condicionamento de comportamento geralmente se mostram suficientes para o manejo de pacientes que apresentam medo e ansiedade frente ao tratamento odontológico. Quando tais técnicas não apresentam os resultados esperados, podemos utilizar terapias medicamentosas conhecidas como sedação consciente para a diminuição da ansiedade odontológica. A ansiedade pode se tornar uma complicação nos procedimentos odontológicos devido aos seus efeitos, como aumento da pressão arterial, hiperventilação e lipotimias. Para evitar tais complicações, podemos fazer uso de benzodiazepínicos, que, quando empregados de forma correta, acabam por tornar o procedimento odontológico muito mais prático e seguro, tanto para paciente como para o profissional. O mecanismo de ação desses medicamentos se dá por uma ação no sistema nervoso central, causando, em última análise, uma depressão das células excitatórias. Seus efeitos variam de acordo com a dose administrada e o medicamento utilizado, podendo causar sedação, hipnose, relaxamento muscular, ação anticonvulsivante, ação dilatadora coronariana e de bloqueio neuromuscular. Com uma ampla margem de segurança e poucas contraindicações, entre os benzodiazepínicos mais utilizados pelos cirurgiões-dentistas, podemos citar: o diazepam, como um ansiolítico indutor de sedação leve; o midazolam, como um indutor de sono e amnésia; o alprazolam, o lorazepam e o triazolam, cada qual com suas devidas propriedades e posologias de eleição. Podemos concluir, por meio desta revisão de literatura, que os benzodiazepínicos são uma opção terapêutica eficiente para o manuseio de pacientes com ansiedade frente ao tratamento odontológico, sendo uma técnica disponível para utilização tanto em ambiente hospitalar como em consultório.
Palavras-chave: Sedação consciente; Benzodiazepínicos; Ansiedade ao tratamento odontológico.
INTRODUCTION
Anxiety and fear of dental treatment are factors in dental surgeons' clinical practice. Although the concept is considered vague, anxiety is defined as fear in the absence of a real object, caused by external and (primarily) internal agents and characterized by apprehension, nervousness, tension, and worry1,2.
Dentistry involves many different sources of patient anxiety. The noise and vibrations of rotary instruments, brusque movements by dentists themselves, exposure of patients to sharp instruments, reports from friends and relatives of negative experiences, and patients' level of knowledge about the procedures that are conducted. In addition to these are factors such as the image of the dental surgeon, known as white coat syndrome, while previous traumatic experiences suffered by the patient, invasive dental procedures such as extractions and restorative and endodontic treatments, and surgical/periodontal treatments are among the greatest causes of dental anxiety3,4.
Several different methods have been employed to assess anxiety levels in patients. One such method is administration of questionnaires on anxiety that use a series of questions and a scoring system to assess the patient's level of anxiety (e.g. the Corah dental anxiety scale)5. The principal clinical manifestations that can be observed in anxious patients are increased blood pressure and heart rate, diaphoresis, trembling, and arrhythmia. There is also evidence that patients with high anxiety levels may be prone to greater perception of sensitivity to pain1.
In attempts to improve comfort in clinical dental practice and increase safety for both patient and clinician, studies have been conducted to eliminate use of general anesthesia in clinical dental settings and introduce drug options for use in combination with local anesthetics, in a technique known as conscious sedation2,6.
In dentistry, the concept of conscious sedation is defined as a minimum level of depression of consciousness, preserving the patient's ability to maintain their own respiration continuously and to respond to the dental surgeon's verbal commands and physical stimuli during dental procedures6.
Benzodiazepines are the medications most used for this technique. Benzodiazepines are drugs that act on the limbic system of the cerebral cortex, as a whole. The cortical regions are involved with voluntary movement and sensory integration, consciousness, abstract thinking, memory, and learning. These drugs bind to specific receptor units in the central nervous system (CNS), potentiating their effects and resulting in prolonged neuronal hyperpolarization with rapid inhibition or attenuation of transmission of nerve impulses, causing depression of the CNS and producing varying degrees of anxiolytic effects, sedation, anterograde amnesia, relaxation of skeletal musculature, and anticonvulsant activity. Although minimal cardiovascular and respiratory effects have been observed, these drugs are practically incapable of causing any type of respiratory or cardiovascular collapse when administered at their correct dosages and when other agents of CNS depression are not present in patients who do not have any kind of contraindication to use of these drugs6-9.
The principal benzodiazepines used in dentistry are diazepam, midazolam, lorazepam, alprazolam, and triazolam.
Anxiety can be considered an obstacle to healthcare. The impact that it can have on patients' lives is considerable, is not restricted to clinical dental settings, and can even be the decisive factor in compliance with and success of treatment10-12.
The objective of this study is to conduct a review of the literature to define benzodiazepines and the drugs in this category most widely used in dentistry, their mechanisms of action, indications and contraindications and their posologies, in order to provide a basis for greater understanding among dental surgeons with regard to the treatment options available for their patients.
LITERATURE REVIEW
Sedation is characterized as a reduction in a patient's activity and excitability and the American Society of Anesthesiologists (ASA) has produced a three-level classification: minimal, moderate, and deep sedation.
When under minimal and moderate sedation, the patient has the capacity to respond to mild tactile stimuli and verbal communication, and cardiovascular and respiratory functions are preserved with no need for assistance. When under deep sedation, the patient is unable to easily respond to verbal commands, but will respond to painful stimuli, and cardiovascular function is normally maintained, but spontaneous respiratory function may be impaired and assistance may be needed13.
Benzodiazepines are drugs with anxiolytic properties and in dentistry they are prescribed to control anxiety and fear because they have proven efficacy, low toxicity, few contraindications, and little capacity for causing dependence. Certain precautions are necessary during planning for procedures, including careful patient history, control with oximetry, provision of basic life support equipment and the knowledge needed to use it. The effects vary depending on the dose administered and the drug chosen for the treatment, but they can include sedative action, hypnotic effects, muscle relaxation, reduction of saliva flow and vomit refl ex, anticonvulsant action, coronary dilation, and neuromuscular blockade. Forms of administration include oral, intravenous, intramuscular, intranasal, sublingual, or rectal, but in dentistry the oral route is most often employed because of the ease of administration and convenience for the patient6,14.
A study that compared the efficacy of medication with benzodiazepines administered via oral and intravenous routes found there were no statistically significant differences in the results obtained in terms of patient cooperation during procedures, demonstrating that oral administration of these drugs produces good results15.
Although benzodiazepines have low toxicity, they can have certain adverse effects depending on the dose administered and the specific drug utilized14. These effects can include reactions such as somnolence, excessive sedation, paradoxical reactions, disturbed motor coordination, confusion and transitory loss of memory, double vision, headaches, and the possibility of physical and psychological dependence if administered for prolonged periods16,17.
A study conducted by Penfield & Rasmussen (1950) indicated that about 75% of the sensory cortex processes impulses originate in orofacial structures such as, for example, lips, mandible, tongue, and teeth. It is therefore possible that this predominant cerebral processing of orofacial sensations may contribute to the aversive anxiety that many patients manifest with respect to dental treatment18.
Benzodiazepines are drugs that act to potentiate the gamma aminobutyric acid (GABA) inhibitory system, which controls psychosomatic reactions to stimuli generated by stress. Benzodiazepine molecules bind to specific subunits of inhibitory GABA-a receptors found in the CNS. When activated, the GABA-a receptor increases the frequency with which chloride channels in nerve cells open, increasing entry of chloride ions and provoking a hyperpolarized state in the cell membrane, which, in the final analysis, results in reduced propagation of the excitatory impulse18-21.
As such benzodiazepine medications act to facilitate GABAergic transmission, increasing the affinity of GABA for its binding site. In the absence of GABA, benzodiazepines produce minor or practically null effects on the capacity to transport chloride into the interior of nerve cells18,20.
Studies of administration of benzodiazepine medications have assessed their efficacy and safety and confirmed that use of these drugs achieves the effects required by dental surgeons with a wide safety margin22-24.
It is important to point out that although there are few contraindications against their use, it is still necessary for the dental surgeon to choose the drug that fits best with the patient's requirements based on age, weight, medical history, and duration of clinical treatment, always assessing each on an individual basis according to their requirements in order to choose the best therapeutic option for each case.
CONTRAINDICATIONS AND CLINICAL PRECAUTIONS
These drugs can be metabolized in a range of different tissues and organs, but the primary site of metabolism is the kidneys. Patients with renal problems may have an altered profile of clearance of these drugs from the body, with reduced excretion and increased plasma concentrations, which makes prolonged use unfeasible in such patients25.
Elderly patients may also have abnormalities affecting the routes through which these drugs are absorbed and excreted due to changes in pH, reduced hepatic metabolism, and increased CNS sensitivity to their effects. It is recommended that for these patients the dose administered should be reduced and the benzodiazepine chosen should be one that is not metabolized slowly25,26.
There can also be abnormalities in the routes of these drugs' excretion in obese patients because benzodiazepines are highly liposoluble and can accumulate in adipose tissues. The drug can then return to the bloodstream, causing an effect known as the "hangover" effect25.
Care should be taken when prescribing benzodiazepines to pregnant women. Studies have reported evidence that use of these medications during the first trimester of pregnancy could be associated with an increased risk of cardiac malformations and cleft lip and palate defects27. However, more recent studies did not find this association28. Use of benzodiazepines during the third trimester is associated with neonatal hypotonia: "flaccid baby syndrome"29. In view of the potential risks, careful history-taking and consultation with the patient's obstetrician are required to arrive at the best choice of drug.
In patients who drink alcohol, use of benzodiazepines should be analyzed with care. Ethanol has additive effects on benzodiazepines in the CNS and accelerates hepatic metabolism of these drugs. Use of short-acting variants of these drugs may not have the desired effects25.
Care should also be taken to avoid occurrence of drug interactions, since the pharmacological properties of one or both medications could be increased or reduced. For example, use of benzodiazepines in combination with drugs such as cimetidine, erythromycin, disulfiram, oral contraceptives, and certain groups of antifungals, may inhibit biotransformation of the benzodiazepine, resulting in higher plasma concentrations and, as a consequence, excessive sedation20,30.
Some patients can exhibit paradoxical effects when given benzodiazepines. The reasons why these reactions occur are not clear and the majority of cases are considered idiosyncratic, involving less than 1% of the patients to whom these drugs are given. The characteristics of these reactions include increased conversation initiated by the patient, excitement and excessive movements, and even hostility and rage. Pediatric patients and the elderly are more prone to these effects and so are patients with psychiatric and/ or personality disorders31.
Patients with glaucoma, myasthenia gravis, or allergy to benzodiazepines, breastfeeding mothers, patients receiving psychiatric treatment, or CNS-depressant treatments, and patients with mental deficiencies should also have their cases evaluated before being given benzodiazepines and it may be necessary to consult clinicians specialized in other areas of healthcare to assess their use15.
Patients who are given these drugs should be instructed not to drink alcoholic beverages for a period lasting from 24 hours before to 48 hours after administration of the benzodiazepine and not to drive or operate heavy machinery under the effects of the medication, and should also be escorted to and from the treatment session20.
BENZODIAZEPINES: PROPERTIES E INDICATIONS
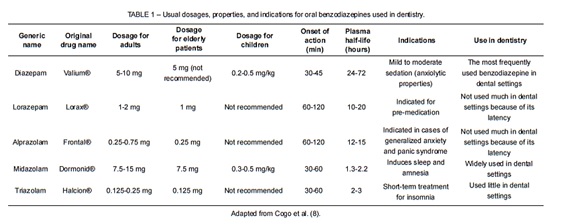
In Brazil, the benzodiazepine medications most used in dental settings are diazepam, midazolam, alprazolam, lorazepam, and triazolam. Table 1 lists their properties and indications and preferred posologies.
Diazepam
Diazepam is the benzodiazepine most frequently used in dentistry because it is the safest member of this class of drugs for use by clinicians with little experience in conscious sedation techniques. The normal administration protocol is 5 or 10 mg orally, 1 hour before the procedure and, for more severe cases of anxiety, 5 or 10 mg administered orally the night before the procedure and another 5 or 10 mg administered orally 1 hour before the dental procedure. Sedation varies from mild to moderate and its anxiolytic property is greater than its capacity for sedation. Onset of action is from 30 to 45 minutes after administration and its clearance half-life is from 24 to 72 hours, due to production of active metabolites, although the clinical effects disappear from 2 to 3 hours after administration8.
After absorption, diazepam is transported to adipose tissues where it is stored and from where it can return to the bloodstream, causing sedation again20.
For pediatric patients, the usual dose varies from 0.2 to 0.5 mg/kg of body weight, but it is recommended that a pediatric dentist and even the patient's pediatrician should be consulted when planning sedation in these cases30, and while this is not the firstchoice drug for elderly patients because of the hangover effect, the usual dose varies from 2 to 5 mg, and both of these age groups demand greater care when prescribing diazepam because of production of active metabolites and their respective excretory system limitations32.
Midazolam
Midazolam is most used in procedures with short duration or in situations in which we intend to induce the patient to sleep; not a first-choice option because of the amnesia effect, (although in certain situations this can actually become a beneficial property since the patient will forget the "moment of trauma") and because there is a need for more sophisticated infrastructure, including oximetry control, when compared with diazepam8,32.
Midazolam has a short clearance half-life, varying from 1.3 to 2.2 hours33, doses can be from 7.5 to 15, or 0.3 to 0.5 mg/kg of body weight in pediatric patients, and are administered 30 minutes before procedures8,20,33.
In contrast with diazepam, midazolam is more soluble in water, does not produce active metabolites and does not therefore provoke repeat sedation, has much faster induction and shorter duration clearance, but, still compared with diazepam, midazolam has a greater sleep induction property than anxiolytic effect20.
Alprazolam
This is another therapeutic option, but it is more commonly administered to patients who have severe cases of generalized anxiety and panic syndrome, and it is not used very much in dental offices because of its long period of latency34. Plasma concentrations are obtained from 1 to 2 hours after administration and it is completely eliminated from the body after 12 to 15 hours. The most often administered doses of alprazolam vary from 0.5 to 0.75 mg in adult patients8 and 0.25 to 0.75 mg in elderly patients35, and it is not recommended for use with pediatric patients.
Lorazepam
Generally used as a premedication, lorazepam also has a long period of latency, which makes use in the dental office problematic. Doses range from 1 to 2 mg, with onset of action from 1 to 2 hours later. It has slow induction and the clearance half-life varies from 10 to 20 hours and, even though it is more liposoluble than diazepam, it does not produce active metabolites20,36.
The effects pass after an interval ranging from 6 to 8 hours after administration has elapsed37 and one of its principle characteristics is the possibility of inducing anterograde amnesia, defined as forgetting events after a certain point in time taken as a reference. For elderly patients the dose varies from 1 to 4 mg and it is not recommended for use with pediatric patients32.
Triazolam
Used very little in Brazil, generally for short-term insomnia treatment, triazolam has a rapid onset of action and short duration. Onset of action occurs around 30 minutes after administration and duration is from 2 to 3 hours20. Habitual doses of triazolam are from 0.125 to 5 mg for adult patients32 and 0.125 mg for elderly patients, orally or sublingually, and once more it is not recommended for pediatric patients8.
Use of benzodiazepine medications is regulated in Brazil by the Ministry of Health Sanitary Vigilance Authority's directive (344/98: May 12th, 1998). Dispensation of benzodiazepines is controlled by the Ministry of Health and special prescriptions must be used, with class B prescription notification, using a specific (blue) document with 30-day validity, each of which can request dispensation of a maximum of five vials of medication for external use (injectable) or three units for internal use (oral route)6.
It is important to emphasize that careful analysis of the patient, taking into account all individual characteristics, is necessary to ensure that the drug treatment is successful and, consequently, that the dental treatment is also successful, thereby guaranteeing better quality and safety for both patient and professional and ensuring that all equipment needed is available in advance, irrespective of the treatment planned.
CONCLUSIONS
When correctly indicated, benzodiazepines treat the symptoms of anxiety, making dental treatment safer for patients and clinicians.
The effects caused by benzodiazepines can include sedative action, hypnotic effects, muscle relaxation, reduction of saliva flow and vomit reflex, anticonvulsant action, neuromuscular blockade, and coronary dilation.
As long as indications and contraindications are respected, these medications can be used by dental surgeons with a wide safety margin, producing few side effects and with practically null capacity to cause dependence.
Dental surgeons have a range of drugs to choose from for provoking conscious sedation in dental settings using benzodiazepines. The most frequently used of these is diazepam, which is most often employed as a mild anxiolytic and is the safest benzodiazepine for use by clinicians with less experience in this type of technique. In turn, midazolam is used to induce sleep and amnesia, alprazolam is more often used for cases of generalized anxiety and panic syndrome, lorazepam is generally used for premedication, and triazolam is generally used for short-term insomnia treatment. All of these have their own characteristics and posologies that must be respected by the dental surgeon when choosing between them.
These medications' advantages outweigh their disadvantages and as long as none of the steps required for use of benzodiazepines are ignored, they offer a very safe and effective option for use in dental clinical practice.
REFERENCES
1. Medeiros LA, Ramiro FMS, Lima CAA, Souza LMA, Fortes TMV, Groppo FC. Avaliação do grau de ansiedade dos pacientes antes de cirurgias orais menores. Rev Odontol UNESP. 2013;42:357-63. [ Links ]
2. Goulart JCF, Pinheiro MD, Rodrigues RV, Santos FS, Martins AT, Scannavino FLF. Infl uence of anxiety on blood pressure and heart rate during dental treatment. Rev Odonto Cienc. 2012;27:31-5.
3. Gaujac C, Santos HT, Garção MS, Silva Júnior J, Brandão JRMCB, Silva TB. Sedação consciente em odontologia. Rev Odontol UNICID. 2009;21:251-7.
4. Maggirias J, Locker D. Psychological factors and perceptions of pain associated with dental treatment. Community Dent Oral Epidemiol. 2002;30:151-9.
5. Tambellini MM, Gorayeb R. Escalas de medo odontológico em crianças e adolescentes: uma revisão de literatura. Paideia. 2003;13:157-61.
6. Oliveira MC, Aleixo RQ, Rodrigues MTV. Use of benzodiazepines in oral and maxillofacial surgery. Saber Cientif Odontol. 2010;1:53-67.
7. Cavalcante LB, Sanabe ME, Marega T, Gonçalves JR, Abreu-e-Lima FCB. Conscious sedation: a backup resource for providing dental care to uncooperative children. Arq Odontol. 2011;47:45-50.
8. Cogo K, Bergamaschi CC, Yatsuda R, Volpato MC, Andrade ED. Conscious sedation with benzodiazepines in dentistry. Rev Odontol UNICID. 2006;18:181-8.
9. Yagiela JA, Dowd FJ, Johnson BS, Mariotti AJ, Neidle EA. Farmacologia e terapêutica para dentistas. 6ª ed. Rio de Janeiro: Elsevier; 2011.
10. Oosterink FM, de Jongh A, Aartman IH. What are people afraid of during dental treatment? Anxiety-provoking capacity of 67 stimuli characteristic of the dental setting. Eur J Oral Sci. 2008;116:44-51.
11. Lahmann C, Schoen R, Henningsen P, Ronel J, Muehlbacher M, Loew T, et al. Brief relaxation versus music distraction in the treatment of dental anxiety: a randomized controlled clinical trial. J Am Dent Assoc. 2008;139:317-24.
12. Shapiro M, Melmed RN, Sgan-Cohen HD, Eli I, Parush S. Behavioural and physiological effect of dental environment sensory adaptation on children's dental anxiety. Eur J Oral Sci. 2007;115:479-83.
13. American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non- Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96:1004-17.
14. Teixeira TF, Quesada GAT. Anxiolytic therapy for odontologic patients. Saude. 2004;30:100-3.
15. Chen M, Hill MH, Patrianakos TD, Ku ES, Chen ML. Oral diazepam versus intravenous midazolam for conscious sedation during cataract surgery performed using topical anesthesia. J Cataract Refract Surg. 2015;41:415-21.
16. Andrade ED. Terapêutica medicamentosa em odontologia. 2ª ed. São Paulo: Artes Médicas; 2006.
17. Taylor D, Paton C, Kapur S. Depression and anxiety. In: Taylor D, Paton C, Kapur S. The Maudsley prescribing guidelines in psychiatry. 12th ed. Oxford: Wiley-Blackwell; 2015. p. 343-52.
18. Penfield W, Rasmussen T. The cerebral cortex of man: a clinical study of localization of function. New York: Macmillan; 1950. Lane Medical Lectures.
19. Loeffl er PM. Oral benzodiazepines and conscious sedation: a review. J Oral Maxillofac Surg. 1992;50:989-97.
20. Ranali J, Volpato MC, Ramacciato JC. Sedação consciente em implante dental. Rev Implant News. 2005;2:105-87.
21. Stahl SM. Anxiety disorders and anxiolytics. In: Stahl SM. Stahl's essential psychopharmacology: neuroscientific basis and practical application. 4th ed. Cambridge: Cambridge University Press; 2013. p. 388-419.
22. Singh N, Pandey R, Saksena A, Jaiswal J. A comparative evaluation of oral midazolam with other sedatives as premedication in pediatric dentistry. J Clin Pediatr Dent. 2003;26:161-4.
23. Barclay MK, Hunter KMacD, Wendy McM. Midazolam and diazepam compared as sedatives for outpatient surgery under local analgesia. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 1985;59:349-55.
24. Milgrom P, Quarnstrom FC, Longley A, Libed E. The efficacy and memory effects of oral triazolam premedication in highly anxious dental patients. Anesth Prog. 1994;41:70-6.
25. Franco GCN, Cogo K, Montan MF, Bermagaschi CC, Groppo FC, Volpato MC, et al. Interações medicamentosas: fatores relacionados ao paciente (Parte I). Rev Cir Traumatol Buco-Maxilo-Fac. 2007;7:17-28.
26. Guimarães FS. Hipnóticos e ansiolíticos. In: Fuchs FD, Wannmacher L. Farmacologia clínica. Fundamentos da terapêutica racional. 2ª ed. Rio de Janeiro: Guanabara Koogan; 1998, p. 360-70.
27. Dolovich LR, Addis A, Vaillancourt JM, Power JD, Koren G, Einarson TR. Benzodiazepine use in pregnancy and major malformations or oral cleft: meta-analysis of cohort and case-control studies. BMJ. 1998;317:839-43.
28. Wikner BN, Stiller CO, Bergman U, Asker C, Källén B. Use of benzodiazepines and benzodiazepine receptor agonists during pregnancy: neonatal outcome and congenital malformations. Pharmacoepidemiol Drug Saf. 2007;16:1203-10.
29. Mcelhatton PR. The effects of benzodiazepine use during pregnancy and lactation. Reprod Toxicol. 1994;8:461-75.
30. Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Farmacologia. 5ª ed. Rio de Janeiro: Elsevier; 2004.
31. Mancuso CE, Tanzi MG, Gabay M. Paradoxical reactions to benzodiazepines: literature review and treatment options. Pharmacotherapy. 2004;24:1177-85.
32. Donaldson M, Gizzarelli G, Chanpong B. Oral sedation: a primer on anxiolysis for the patient. Anesth Prog. 2007;54:118-29.
33. Chen Q, Wang L, Ge L, Gao Y, Wang H. The anxiolytic effect of midazolam in third molar extraction: a systematic review. PLoS One. 2015;10:e0121410. doi:10.1371/ journal.pone.0121410
34. Pecknold JC, Swinson RP, Kuch K, Lewis CP. Alprazolam in panic disorder and agoraphobia: results from a multicenter trial. III. Discontinuation effects. Arch Gen Psychiatry. 1988;45:429-36.
35. Matear DW, Clarke D. Considerations for the use or oral sedation in the institutionalized geriatric patient during dental interventions: a review of the literature. Spec Care Dentist. 1999;19:56-63.
36. Álvarez AM, Alvarez M. Sedacíon oral: fundamentos clínicos para su aplicacíon en odontología. Rev CES Odontol. 2006;19:62-73.
37. Goodchild JH, Feck AS, Silverman MD. Anxiolysis in general dental practice. Dent Today. 2003;22:106-11.
 Correspondence:
Correspondence:
Theodoro Weissheimer
Faculdade de Odontologia
Departamento de Graduação
Universidade Luterana do Brasil – Campus Canoas
Rua Farroupilha, 8001, Prédio 59, Bairro São José
CEP 92425-900, Canoas
RS, Brazil
E-mail: theodoro.theo@hotmail.com
