










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkStomatos
versão impressa ISSN 1519-4442
Stomatos vol.22 no.43 Canoas Jul./Dez. 2016
Unusual foraminal position in a mandibular molar
Posição foraminal atípica em molar inferior
Márcia da Silva Schmitz I; Cláudia Medianeira Londero Pagliarin I; Aline Londero II; Francisco Montagner III; Renata Dornelles Morgental I
I PhD in Endodontics from Department of Stomatology, School of Dentistry, Universidade Federal de Santa Maria (UFSM), Santa Maria, RS, Brazil
II dental surgeon from School of Dentistry, UFSM, Santa Maria, RS, Brazil
III PhD in Endodontics from Department of Conservative Dentistry, School of Dentistry, Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil
The authors have no conflicts of interest to declare concerning the publication of this manuscript.
ABSTRACT
Knowledge of possible morphological variations of the root canal system is crucial to achieve endodontic success. The radiographic apex is traditionally used as a reference point for establishing the apical limit of root canal instrumentation and obturation. However, frequently it does not coincide with the major apical foramen. This article describes the rare case of a mandibular molar with necrotic pulp and apical periodontitis exhibiting an unusual foraminal position with a distance from the radiographic apex of about 7 mm. The left mandibular molar of a 46-year-old female patient was referred for endodontic treatment. Following radiographic suspicion of apical calcification, comparison with the mandibular molar on the opposite side, electronic working length determination and visualization of a size #15 file emerging through the foramen in the working length radiograph, the anatomical variation was confirmed, and endodontic procedures were performed according to conventional techniques. Following chemomechanical preparation, intracanal medication with calcium hydroxide, and obturation, total regression of the periapical lesion was verified after 7 years of follow-up. According to the literature, the distance between the root canal foramen and the root apex may range from 0 to 3 mm, but in this specific case the distance reached 7 mm. Dentists should be aware of this atypical anatomical situation when treating mandibular molars.
Keywords: Endodontics; Root canal therapy; Tooth apex.
RESUMO
O conhecimento das possíveis variações morfológicas do sistema de canais radiculares é crucial para alcançar o sucesso endodôntico. O ápice radiográfico é usado como ponto de referência para estabelecer o limite apical da instrumentação e obturação dos canais radiculares. No entanto, é bem sabido que frequentemente ele não coincide com o forame apical maior. Este estudo apresenta um raro caso de molar inferior com necrose pulpar e periodontite apical, exibindo uma posição incomum do forame com uma distância do ápice radiográfico de cerca de 7 mm. O molar inferior esquerdo de uma paciente de 46 anos foi encaminhado para tratamento endodôntico. Após suspeita radiográfica de calcificação apical, comparação com o molar inferior do lado oposto, determinação eletrônica do comprimento de trabalho e visualização de uma lima #15 emergindo através do forame na radiografia odontométrica, a variação anatômica foi confirmada, e os procedimentos endodônticos foram realizados de acordo com técnicas convencionais. Após preparo químicomecânico, medicação intracanal com hidróxido de cálcio e obturação, a regressão total da lesão periapical foi verificada após 7 anos de acompanhamento. Segundo a literatura endodôntica, a distância entre o forame do canal radicular e o ápice radicular pode variar de 0 a 3 mm, mas neste caso específico, a distância alcançada foi de 7 mm. Os dentistas devem estar cientes desta situação anatômica atípica ao tratar molares inferiores.
Palavras-chave: Endodontia; Tratamento do canal radicular; Ápice dentário.
INTRODUCTION
Determination of working length (WL) is one of the most important steps in root canal treatment1. Failure in correctly establishing the WL may result in over-filling or under-filling and has the potential to reduce endodontic success rates by over 10%, as shown in a 10-year retrospective clinical study2. Other investigations have confirmed that the apical level of root filling has a significant influence on the outcome of root canal treatment, with the best prognosis being found for roots in which the filling reached within 2 mm of the radiographic apex3.
In this context, the apical constriction has been described as the ideal and recommended endpoint for instrumentation and obturation4. Nevertheless, there are situations in which the apical foramen may be a more useful landmark5, e.g., in the presence of apical pathosis and root resorption (6). Also, it is worth mentioning Ponce and Fernandez7, who reported that the apical constriction rarely coincides with the cemento-dentino-canal junction. It would not be feasible to clinically find this histological structure, as the extension of the cementum may vary on the walls of the cemental canal in the same tooth.
The use of the radiographic apex as a reference point in everyday clinical practice is also questionable, as several studies using different groups of teeth have reported that the major apical foramen often does not coincide with the anatomical apex5,7-9. Rather, it might be located laterally and in a distance of up to 3 mm from the root apex5. Studies involving root apices of mandibular molars have confirmed these findings10-16, as shown in Table 1. Furthermore, Kuttler (9) observed that the center of the foramen deviates more as age increases, whereas the apical constriction becomes smaller. All these variations make it difficult to localize the foramen and constriction using a radiological approach, especially when the deviation is toward the buccal or lingual aspect of the root.

The development of electronic devices capable of locating the major foramen was a great advancement. However, despite their high accuracy, as reported in in vitro and in vivo studies17, clinical efficacy depends on brands, on the use of appropriate irrigating solutions, among other factors18. A recent systematic review has recommended at least one radiographic control to detect possible errors of electronic devices19. Also, radiography is important to provide information on the anatomy of the apical region and possible variations – knowledge that is essential to determine the extent of root canal procedures.
In this study, we describe the case of a mandibular molar with necrotic pulp and apical periodontitis, which presented an unusual variation of the apical foramen position and was followed for 7 years.
CASE REPORT
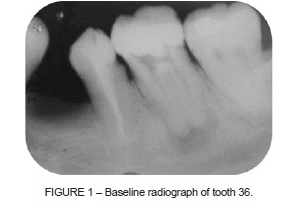
A 46-year-old Caucasian female patient with unremarkable medical history was referred for endodontic treatment of tooth 36 due to periapical inflammatory disease visible on radiograph (Figure 1).
After access cavity preparation using a #1014 spherical high-speed bur (KG Sorensen, São Paulo, SP, Brazil) and an Endo-Z bur (Dentsply-Maillefer, Ballaigues, Switzerland), rubber dam isolation was performed. Three root canals were located and copiously irrigated with 2.5% sodium hypochlorite (NaOCl) (Novaderme, Santa Maria, RS, Brazil). Cervical preflaring was performed with #2 and #3 Gates-Glidden burs (Dentsply-Maillefer). After careful root canal exploration, it was not possible to introduce a K-file (Dentsply-Maillefer) to the desired WL, i.e., 1 mm short of the radiographic apex in both the mesiobuccal (MB) and the mesiolingual (ML) canals. An electronic apex locator (Root-ZX, J. Morita Corp., Kyoto, Japan) was used and showed that the measures should be 13.5, 16.5, and 19 mm in the MB, ML, and distal canals, respectively. These measures were confirmed radiographically. Chemomechanical preparation was performed using a crown-down technique. Then, intracanal medication comprising calcium hydroxide (Calen-PMCC®, SS White, Rio de Janeiro, RJ, Brazil) was used for 15 days with a glass ionomer cement temporary restoration (Vitro Fill®, DFL Indústria e Comércio S.A., Jacarepaguá, RJ, Brazil).
Considering that previous authors (Table 1) have reported distances ≥ 3.10 mm between the root apex and the apical foramen of mandibular molars16, prognosis of tooth 36 was doubtful. The patient was warned about the need for postoperative radiographs and clinical examination twice yearly, in the search for signs and symptoms that could indicate endodontic failure and require complementary treatments.
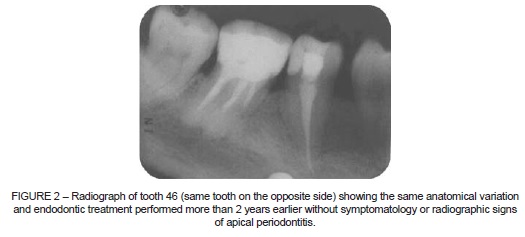
Periapical survey showed that tooth 46 (Figure 2), on the opposite side, showed root canal filling with similar WL in the mesial roots, i.e., several millimeters short of the radiographic apex. The patient reported that treatment had been performed 2 years earlier. There was no swelling, sinus tract, spontaneous/provoked pain, or periapical lesion, which indicates a successful treatment.
After 15 days of calcium hydroxide dressing in tooth 36, none of the above signs and symptoms was observed, and therefore the root canals were dried and obturation was performed using the cold lateral condensation technique with gutta-percha (Endopoints®, Paraíba do Sul, RJ, Brazil) and zinc oxide-eugenol-based sealer (Dentsply Indústria e Comércio Ltda., Petrópolis, RJ, Brazil) (Figure 3A).
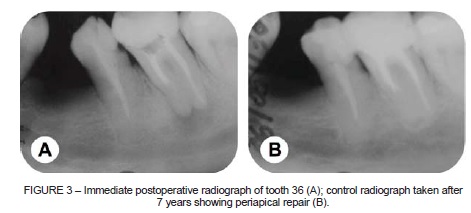
The patient did not return for the biannual clinical and radiographic control visits. Rather, she presented at the dental office complaining of pain in another tooth, 7 years after endodontic treatment of tooth 36. A new radiograph demonstrated complete periapical healing with regression of the radiolucent lesion and integrity of the lamina dura (Figure 3B).
DISCUSSION
Endodontic treatment prognosis is directly related with the anatomical and pathological characteristics of each individual. Current techniques continue to fail to overcome the complex endodontic microbiota and endless anatomical variations of the root canal system20. This article presents an endodontic case characterized by pulpal necrosis and apical periodontitis, a clinical condition with a lower rate of success when compared to cases of vital pulps3. The case also showed a distance between the apical foramen and the radiographic apex greater than the distances reported in the relevant literature (Table 1).
In the WL radiograph, a size #15 K-file was observed emerging through the foramen. As reported by Von der Lehr and Marsh21, the point where the endodontic file exits the foramen can be visualized radiographically when it opens mesially or distally. However, when the foramen has a buccal or lingual opening, the root structure is superimposed, masking its radiographic visualization. Some authors have reported that the most frequent location of the major foramen in posterior teeth is on the distal surface11,12.
In the present case, the Root-ZX electronic apex locator was used because it has been shown to provide reliable WL determination in many laboratory and clinical studies17,22. The accuracy of WL determination using only the Root-ZX device vs. combining Root-ZX measurements and WL radiographs was evaluated by Kim et al.23. There were no significant differences between the two methods, yet the accuracy rates were 84 and 96%, respectively. Electronic measurements, combined with clinical examination and radiographs of the same tooth on the opposite side, with similar characteristics, were important aspects to conduct this treatment.
Patient age should also be taken into account when considering the discrepancy between the location of the apical foramen and the root apex. Pineda and Kuttler24 analyzed 7,275 root canals of different teeth, and patients were distributed into three groups according to age: < 25 years; 35-45 years; > 55 years old. The authors observed that aging was directly related to reduction of the root canal diameter, as well as increase of the deviation of the foramen in relation to the root apex, due to the continuous deposition of cementum. Thus, the higher the age, the greater the distance.
Also, patient involvement is important for treatment planning. Professionals should explain clinical signs and symptoms and the danger of an infection with endodontic origin for the general health25. In this context, follow-up visits, even though neglected by many patients, are crucial after root canal therapy. In cases of endodontic failure in mandibular teeth, difficulties accessing the posterior region and the proximity between roots and the mandibular canal may hinder or even prevent a paraendodontic surgery.
FINAL CONSIDERATIONS
This case report is an example of an unusual foraminal position variation that had a successful outcome after endodontic treatment. Even though the present report cannot be used as reference, it sheds light on how to deal with important anatomical variations in clinical practice and may help prevent more aggressive procedures, such as apical surgery or premature extraction of teeth and replacement with dental implants.
REFERENCES
1. Wu MK, Wesselink PR, Walton RE. Apical terminus location of root canal treatment procedures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:99-103. [ Links ]
2. Stoll R, Betke K, Stachniss V. The infl uence of different factors on the survival of root canal fillings: a 10-year retrospective study. J Endod. 2005;31:783-90.
3. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16:498-504.
4. Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation, part 2. A histological study. Int Endod J. 1998;31:394-409.
5. Dummer PM, McGinn JH, Rees DG. The position and topography of the apical canal constriction and apical foramen. Int Endod J. 1984;17:192-8.
6. Simon JH. The apex: how critical is it? Gen Dent. 1994;42:330-4.
7. Ponce EH, Vilar Fernandez JA. The cemento-dentino-canal junction, the apical foramen, and the apical constriction: evaluation by optical microscopy. J Endod. 2003;29:214-9.
8. Green D. Morphology of the pulp cavity of the permanent teeth. Oral Surg Oral Med Oral Pathol. 1955;8:743-59.
9. Kuttler Y. Microscopic investigation of root apexes. J Am Dent Assoc. 1955;50:544-52.
10. Green D. Stereomicroscopic study of 700 root apices of maxillary and mandibular posterior teeth. Oral Surg Oral Med Oral Pathol. 1960;13:728-33.
11. Burch JG, Hulen S. The relationship of the apical foramen to the anatomic apex of the tooth root. Oral Surg Oral Med Oral Pathol. 1972;34:262-8.
12. Blaskovic-Subat V, Maricic B, Sutalo J. Asymmetry of the root canal foramen. Int Endod J. 1992;25:158-64.
13. Morfis A, Sylaras SN, Georgopoulou M, Kernani M, Prountzos F. Study of the apices of human permanent teeth with the use of a scanning electron microscope. Oral Surg Oral Med Oral Pathol. 1994;77:172-6.
14. Marroquin BB, El-Sayed MA, Willershausen-Zonnchen B. Morphology of the physiological foramen: I. Maxillary and mandibular molars. J Endod. 2004;30:321-8.
15. Arora S, Tewari S. The morphology of the apical foramen in posterior teeth in a North Indian population. Int Endod J. 2009;42:930-9.
16. Martos J, Ferrer-Luque CM, Gonzalez-Rodriguez MP, Castro LA. Topographical evaluation of the major apical foramen in permanent human teeth. Int Endod J. 2009;42:329-34.
17. Gordon MP, Chandler NP. Electronic apex locators. Int Endod J. 2004;37:425-37.
18. Tsesis I, Blazer T, Ben-Izhack G, Taschieri S, Del Fabbro M, Corbella S, et al. The precision of electronic apex locators in working length determination: a systematic review and meta-analysis of the literature. J Endod. 2015;41:1818-23.
19. Martins JN, Marques D, Mata A, Carames J. Clinical efficacy of electronic apex locators: systematic review. J Endod. 2014;40:759-77.
20. Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. 2004;15:348-81.
21. Von der Lehr WN, Marsh RA. A radiographic study of the point of endodontic egress. Oral Surg Oral Med Oral Pathol. 1973;35:705-9.
 Correspondence:
Correspondence:
Renata Dornelles Morgental
Departamento de Estomatologia
Universidade Federal de Santa Maria (UFSM)
Rua Marechal Floriano Peixoto, 1184
CEP 97015-372, Santa Maria
RS, Brazil
E-mail: remorgental@hotmail.com
