










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.10 no.1 Piracicaba Jan./Mar. 2011
ORIGINAL ARTICLE
Quantitative light-induced fluorescence (QLF) in relation to other technologies and conventional methods for detecting occlusal caries in permanent teeth
Antônio Carlos PereiraI; Hafsteinn EggertssonII; Carlos González-CabezasIII; Domenick T. ZeroII; George J. EckertIV; Fábio Luiz MialheI
I Department of Community Dentistry, Piracicaba Dental School, University of Campinas, SP, Brazil
II Indiana University School of Dentistry, Indianapolis, IN, USA
III University of Michigan School of Dentistry, Ann Arbor, MI, USA
IV Indiana University School of Medicine, Indianapolis, IN, USA
ABSTRACT
Aim: The aim of this in vitro study was to compare the reproducibility and accuracy of quantitative light-induced fluorescence (QLF) in relation to other technologies and conventional methods for detecting occlusal carious lesions. Methods: Ninety-six extracted permanent molar teeth were selected. Three examiners carried out examinations using Visual examination (VI), bitewing radiographs (RX), QLF, electrical conductance measurement (ECM), and DIAGNOdent. Twentyfive percent of the teeth were re-examined for repeatability. Stereomicroscopic examination was used as the gold standard. Results: Intra- and inter-examiner agreement ranged from 0.43 to 0.89. Areas under ROC curves were 0.82, 0.54, 0.84, 0.79 and 0.88, respectively, for VI, RX, QLF, ECM and DIAGNOdent examinations, with RX significantly lower than the other methods. No significant statistical difference was found when comparing the areas under ROC curve of visual inspection and QLF. Conclusions: Although QLF and other technologies for early caries detection may offer some advantages, this study did not find significant improvement in occlusal caries detection when compared to visual examination.
Keywords: dental caries, detection, diagnosis, pits and fissures, quantitative light-induced fluorescence, visual scoring of caries, radiograph, fluorescence, accuracy, ECM.
Introduction
Over the past 40 years there have been changes in the epidemiological pattern of dental caries around the world. These changes have been characterized by a reduction in prevalence and severity of carious lesions1-2. The reduction has been surface dependent, and the occlusal surfaces of teeth are the sites most frequently affected by dental caries1-2. The reduction in caries progression has resulted in changes in the morphology and pattern of lesions, making it more difficult for the clinician to detect and assess the extent of the lesion3.
Detection of carious lesions in their earliest stages has important implications for preventing their progression before cavitation occurs. Unfortunately, traditional diagnostic systems for detecting caries lesions, such as visual inspection and radiography, have limited accuracy and sensitivity when diagnosing occlusal caries at the pre-cavitated level3-4. To improve the accuracy of diagnosis, non-invasive instrumentbased techniques have been developed for detecting and quantifying demineralization5-7. These techniques include methods based on electrical conductance measurement and laser- or light-induced fluorescence properties associated with demineralized dental tissues. At the same time, proposals have been put forward for improvement in the visual examination, which include the detection of caries lesions in pre-cavitated stages7-9.
However, in relation to light-induced fluorescence (QLF), few studies have been published evaluating the diagnostic performance of the method on occlusal surfaces and comparing it with traditional and other techniques for caries detections8-9. Therefore, the aim of this study was to evaluate in vitro the performance of QLF for detecting occlusal caries and compare the results with visual examination criteria adopted by Ekstrand6-7, and with other technologies in permanent molars without cavitation.
Material and methods
The study was approved by the Research Ethics Committee of the Piracicaba Dental School, University of Campinas, registration number 027/2004. Ninety-six extracted permanent molar teeth exhibiting complete root formation were selected from an institutional teeth depository. The occlusal surfaces were visually diagnosed for caries and ranged from sound to varying degrees of fissure discoloration and possible microscopic breakdown of the surface structure (extractions especially for orthodontic reason). None of the teeth showed macroscopic signs of cavity formation. The teeth were stored in 0.1% thymol solution for less than 3 months from the time of extraction. Teeth with dental fluorosis, tetracycline stain, hypoplasia or dental restorations were excluded. The teeth were cleaned with a prophylaxis brush using pumice slurry, rinsed with a 3-way syringe, and after the ECM examination, mounted in blocks in sets of 3 teeth. The occlusal surfaces were photographed (×4 magnification), and one site on each tooth was selected and marked on the photograph for identification during examinations. The teeth were stored under refrigeration in de-ionized water in individual plastic containers.
Three examiners participated in this study. All the examiners underwent a training session, which consisted of two-hours of theoretical training and four-hours of practice on extracted teeth. Additionally, a pilot study was conducted, using 9 supplementary teeth.
Examinations
Visual Examination
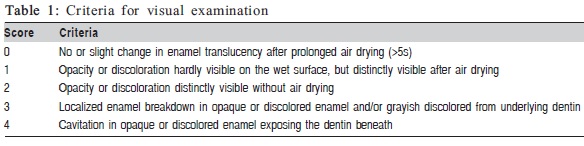
Visual examination was carried out using only a dental operating light and air-drying up to 5 s. No explorer was used during the examination. Each surface was scored using the criteria described by Ekstrand et al.7, as presented in Table 1.
Radiographic Examination
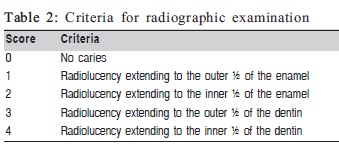
The teeth were radiographed under standardized conditions and the exposures were made using a Trophy General Electric GE 1000 Intraoral x-ray machine, operating at 70 kVp and 8 mA. The blocks of teeth were placed in a holder, specially designed to provide standardized projection geometry during exposure. The focus-film distance was 21 cm and a 15- mm-thick soft tissue equivalent material was placed between the cone end and the blocks of teeth. The classification criteria for radiographic examination are shown in Table 2.
Quantitative Light-induced Fluorescence (QLF)
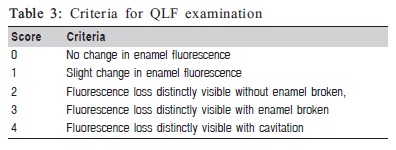
Images of occlusal surfaces of tooth specimens were captured using a portable intra-oral camera device connected to a computer (QLF, Inspektor Research Systems BV, Amsterdam, The Netherlands). Each occlusal surface was illuminated with 13 mW/cm2 of the violet-blue light (wave length: 290-450 nm) and the images were captured through a yellow 520 nm high-pass filter using a custom-made software (QLF, Inspektor Research Systems BV). The images were scored subjectively from the stored images displayed on a CRT monitor. The scoring criteria are shown in Table 3.
Electrical Conductance Measurement (ECM)
Electrical conductance method was performed using the Electronic Caries Monitor III (ECM III, LODE, Groningen, The Netherlands). The ECM examination had to be done before mounting to allow for a reference electrode to be attached to the root complex for measurement. Before each measurement the occlusal surface of the tooth was moistened with de-ionized water then gently air-dried and a toothpaste gel was syringed into the fissure system as a conducting medium. The reference electrode was attached to the root and the measurement electrode probe placed in contact with the fissure enamel at the site identified in the photograph, activating the co-axial air flow (7.5 L/min) until stable readings were obtained. ECM readings ranged from 0.00 indicating low conductance, to 99.99 being the highest measurable conductance. A score of 15 or lower was considered to indicate the presence of caries. Each site was examined three times, and the average of these readings was considered as a definitive score.
Laser Fluorescent (LF) Examination
Laser fluorescence measurements were made using the DIAGNOdent device (Kavo, Biberach, Germany). The device was calibrated before use on the standardized porcelain chip provided by the manufacturer. Using probe tip A, the machine was then calibrated against a sound area on each tooth separately, by holding the tip against a sound smooth surface and pressing the ring button until calibration was completed. The conical probe tip was then positioned perpendicularly over each selected site and slightly rotated around its long axis. Each site was measured 3 times using the abovementioned procedures, and the average of these readings (0- 99 range) was considered as a definitive score.
Histological Validation
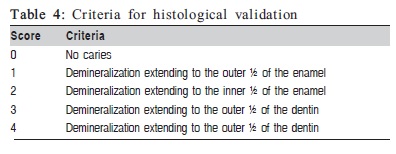
After all assessments were completed, the teeth were removed from the blocks, and approximately 150 to 200- μm-thick buccolingual sections made using a Silverstone- Taylor microtome (Silverstone-Taylor, Scientific Fabrications Co., Lafayette, CO, USA), by cutting through the pre-selected site in the occlusal surface. The histologic examination was done with a stereomicroscope at ×40 magnification. Both sides of each tooth section and the more severe side scored for the specimen. Three examiners underwent a training session, which consisted of 2 h of theoretical training and 4 h of practice on extracted teeth. Additionally, a pilot study was conducted, using nine supplementary teeth. All examiners were university teachers who had graduated more than 10 yr previously, had experience in clinical teaching, and had up to 4 yr of experience in clinical practice10. Caries was defined as being present when demineralization was observed, seen as white or discolored (yellow/brown) area. The histological criteria for caries lesion depth are presented in Table 4.
Statistical Analysis
To assess the intra-examiner agreement, 25 teeth were re-examined. Intra- and inter-examiner reproducibility for the ordinal visual, radiographic and QLF scores were assessed using weighted kappa statistics11. Intra- and inter-examiner reproducibility for ECM and DIAGNOdent were assessed using intraclass correlation coefficients (ICC)12. In order to compare the sensitivity, specificity, accuracy, and area under the ROC curve (AUC) between methods, a bootstrap sampling procedure was used. A bootstrap sample was obtained by randomly selecting specimens with replacement, preserving the percentages of true positives and true negatives in the sample distribution. The estimates were obtained for each of the 1000 bootstrap samples for each method, and the difference between methods was calculated. Bootstrap sampling allows p-values and confidence intervals to be generated for the differences between methods10. The sensitivity, specificity, and accuracy were calculated for the D1 diagnostic threshold (histology score > 1) with the cutoff > 0 ratings for visual and cut-off 3 2 for QLF measurements. For ECM site measurements, the cut-off for all lesions was < 15 and for DIAGNOdent, the cut-off limits for all lesions were values 3 5, adopted by Lussi et al.13 Area under the ROC curve, an indicator of overall diagnostic performance which does not require cut-offs for the diagnostic methods, was computed using the c-statistic from logistic regression models for each examiner and for each method. SPSS and SAS statistical software packages were used for statistical analysis.
Results
The histological examination revealed that 41 sites (43%) were sound; 31 (32%) had demineralization in enamel and 24 (25%) had demineralization extending into dentin.
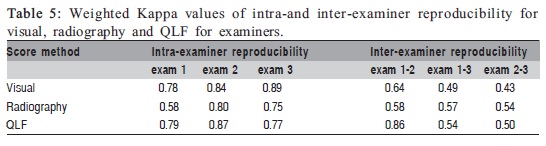
Table 5 shows weighted kappa values for intra- and inter-examiner reproducibility for the visual examination, radiography, and QLF ranked scoring systems. Weighted kappas for intra-examiner repeatability ranged from 0.58 to 0.89 and QLF presented the best results for examiner 2. In relation to inter-examiner reproducibility, QLF presented better results than visual and radiography methods.
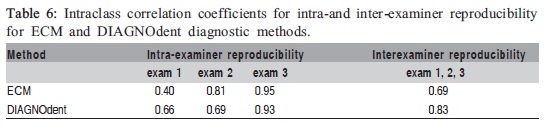
Table 6 presents the values of intraclass correlation coefficients for intra- and inter-examiner reproducibility for DIAGNOdent and ECM diagnostic methods. Intra-examiner agreement for both ECM and DIAGNOdent varied widely among examiners, with ICCs ranging from 0.40 to 0.95, but it was clearly higher for one of the examiners (range: 0.93- 0.95). Inter-examiner agreement was higher for DIAGNOdent (ICC=0.83) than for ECM (ICC=0.69).
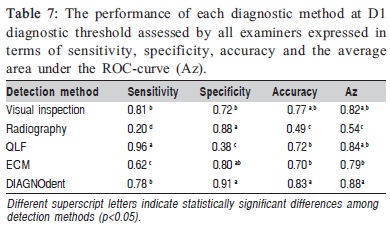
The performance of each diagnostic method in terms of sensitivity, specificity, accuracy and the area under the ROCcurve (Az) are shown in Table 7. LF presented the best sensitivity but the worst specificity values. DIAGNOdent had a higher Az, accuracy, and sensitivity than ECM; higher accuracy than QLF, and higher specificity than visual. QLF presented the best sensitivity but the worse specificity values.
The radiographic method was significantly worse than any of the other methods for Az, accuracy, and sensitivity while it had higher specificity than the visual and QLF methods.
Discussion
In the present study, the traditional visual diagnosis of occlusal caries presented high sensitivity (0.81) and specificity (0.72) values. These findings are similar to those obtained by other studies3,6-7,14-16, that showed high sensitivity values (0.80-0.98) and moderate to high specificity values (0.38-0.98) at D1 and D2 diagnostic thresholds. The visual criteria used in the present and in these studies were those proposed by Ekstrand et al.6 The better performance of the visual inspection compared with other methods assessed in this study, should also be compared with the traditional visual examination, as none of the teeth in the study had macroscopic cavitation, and therefore would have been called sound. It should also be born in mind that the majority of teeth had narrow and deep fissures typical of third molars. Some authors have demonstrated that in teeth with narrow fissures, the overall sensitivity, specificity and the percentage of correctly diagnosed teeth decreased 30% on average, in comparison with those that had wide fissures14.
Studies comparing the areas under ROC curve for QLF and visual inspection have shown conflicting results. Some authors affirm that visual inspection is as good as QLF when the dentist is instructed to detect the early signs of caries, and have not found significant differences in the areas under ROC curve between the methods17-18.
On the other hand, QLF has been found to detect more non-cavitated caries lesions than visual inspection using the criteria of Ekstrand8. However, due to its time-consuming image processing and analysis and higher cost, authors questioned the practicality of QLF for regular use in the dental office at the present stage. Furthermore, it has been suggested that the use of QLF technology must be combined with visual clinical examination since QLF detects any hypocalcified area, including developmental defects and dental fluorosis17.
The poor performance of bitewing radiography in the present study may be attributed to several reasons: the majority of the studies evaluating the performance of radiographic methods in detecting occlusal caries lesions serially sectioned the teeth in the buccolingual direction, the probability of a carious lesions being found is greater and the diagnostic performance of the method would potentially be better6-7,10,19.
Several in vivo and in vitro studies have demonstrated that QLF presented better repeatability and reproducibility values for the quantification of smooth-surface caries than in pit and fissures ones20-22. However, it is interesting to note that studies have found higher levels of intra/inter-examiner reliability for QLF when detection of occlusal caries lesions was done through quantitative analysis using the QLF analysis software than when using qualitative interpretation of the images, as was the case of the criteria utilized in the present study8-9,23. These differences could also be attributed to the threshold value chosen for a caries lesion to be considered absent or present. A review of the effectiveness of QLF to detect occlusal caries lesions showed that intra and interexaminer reproducibility values were above of 0.90 when the evaluations were based on D3 diagnostic threshold24.
In the present study, the criteria used for QLF demonstrated a good performance in detecting occlusal caries lesions, represented by the area under ROC curve (Az) and no significant statistical difference in Az was found with visual inspection and DIAGNOdent. DIAGNOdent showed the highest accuracy at D1 diagnostic threshold (0.83), which in agreement with the published literature13,19,25.
Strong positive correlation between the histological examination and DIAGNOdent was observed, although it was lower than those obtained by other authors16,19,26. The performance of this method could be dependent on the cutoff points used, as a probable source of variation, which could explain the different results in the performance of this method. Here, the cut-off chosen was a value of 5 which is lower than the recommended value of 15 for clinically detected early lesions. This correction is to compensate for the fluorescence decrease that occurs in teeth stored in different media, including the solution used for tooth storage in this study27.
An important difference between QLF and the other methods evaluated was its lower specificity, which could lead to more false-positive diagnosis and consequently overtreatments. Low specificity values for QLF have been reported previously18,28.
The sensitivity and specificity values for ECM found in the present study were lower than those found by other studies6,15-16,29. However, the estimated area under the ROC curve for occlusal caries detection agreed with the data presented by other authors16,29-30. Only a moderate correlation was found between depth of the lesions and the numerical ECM reading. These results were in agreement with those obtained by Ricketts et al.30-31 but were lower than data presented in other studies6-7. This could be attributed to the differences in the histological scores used.
Although QLF, ECM and DIAGNOdent provide an appealing high-tech approach in the dental office, the present results do not suggest they are a significant improvement over a well-trained eye using the new visual criteria. Therefore, although the advantages of QLF, ECM and DIAGNOdent provide quantitative information, allowing the progression or arrest of carious lesions to be monitored in the course of time, the effectiveness of these emerging technologies only for detecting occlusal enamel and dentinal lesions in comparison with traditional methods is questionable. However, the higher specificity values found by some of these technologies indicated that those diagnostic methods were more accurate than the visual method for detecting sound surfaces. Considering the decrease in the prevalence of caries in many populations around the world, these methods could be used as adjuncts in sites where there is clinical uncertainty, thereby decreasing the probability of over-treatment. While QLF and ECM methods have several advantages, they are expensive, and a less expensive device, such as DIAGNOdent, would probably find greater acceptance by clinicians. Further studies should focus on the applicability and effectiveness of new visual methods, using different classification criteria, and the combination of these with emerging technologies.
In conclusion, although QLF and other technologies for early caries detection present some advantages, this study did not find significant improvement in occlusal caries detection when compared to visual examination system.
References
1. Hugoson A, Koch G, Hallonsten AL, Norderyd J, Aberg A. Caries prevalence and distribution in 3-20-years-olds in Jönköping, Sweden, in 1973, 1978, 1983, 1993. Community Dent Oral Epidemiol. 2000; 28: 83-9. [ Links ]
2. Hugoson A, Koch G. Thirty year trends in the prevalence and distribution of dental caries in Swedish adults (1973-2003). Swed Dent J. 2008; 32: 57-67.
3. Bader JD, Shugars DA, Bonito AJ. A systematic review of the performance of methods for identifying carious lesions. J Public Health Dent. 2002; 62: 201-13.
4. Pretty IA, Maupomé G. A closer look at diagnosis in clinical dental practice: Part 3. effectiveness of radiographic diagnostic procedures. J Can Dent Assoc. 2004; 70: 388-94.
5. Lussi A, Imwinkelried S, Pitts NB, Longbottom C, Reich E. Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res. 1999; 33: 261-6.
6. Shi XQ, Welander U, Angmar- Månsson B. Occlusal caries detection with Kavo DIAGNOdent and radiography: an in vitro comparison. Caries Res. 2000; 34: 151-8.
7. Zandona AF, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc. 2006; 37: 1675-84.
8. Ekstrand KR, Ricketts DNJ, Kidd EAM. Reproducibility and accuracy of three methods for assessment of demineralization depth on the occlusal surface: an in vitro examination. Caries Res. 1997; 31: 224-31.
9. Ekstrand KR, Ricketts DNJ, Kidd EAM, Qvist V, Schou S. Detection, diagnosing, monitoring and logical treatment of occlusal caries in relation to lesion activity and severity: an in vivo examination with histological validation. Caries Res. 1998; 32: 247-54.
10. Kühnisch J, Ifland S, Tranaeus S, Hickel R, Stösser L, Heinrich-Weltzien R. In vivo detection of non-cavitated caries lesions on occlusal surfaces by visual inspection and quantitative light-induced fluorescence. Acta Odontol Scand. 2007; 65: 183-8.
11. Kühnisch J, Ifland S, Tranaeus S, Angmar-Månsson B, Hickel R, Stösser L et al.. Establishing quantitative light-induced fluorescence cut-offs for the detection of occlusal dentine lesions. Eur J Oral Sci. 2006; 114: 483-8.
12. Landis J R, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33: 159-74.
13. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979; 86: 420-8.
14. Pereira AC, Eggertsson H, Martinez-Mier EA, Mialhe FL, Eckert GJ, Zero DT. Validity of caries detection on occlusal surfaces and treatment decisions based on results from multiple caries-detection methods. Eur J Oral Sci. 2009; 117: 51-7.
15. El-Housseiny AA, Jamjoum H. Evaluation of visual, explorer, and a laser device for detection of early occlusal caries. J Clin Pediatriat Dent. 2001; 26: 41-8.
16. Pereira AC, Verdonschot EH, MCDNJM Huysmans. Caries detection methods: can they aid decision making of invasive sealant treatment? Caries Res. 2001; 35: 83-9.
17. Côrtes DF, Ellwood RP, Ekstrand KR. An in vitro comparison of a combined FOTI/visual examination of occlusal caries with other caries diagnostic methods and the effect of stain on their diagnostic performance. Caries Res. 2003; 37: 8-16.
18. van der Veen MH, de Josselin de Jong E. Application of quantitative lightinduced fluorescence for assessing early caries lesions. Monogr Oral Sci. 2000; 17: 144-62.
19. Kano-Wilson LH, Ferreira Zandona AG. Comparing ICDAS, Diagnodent, QLF, and neksDUO in occlusal caries detection. J Dent Res. 2007: 86(Spec Issue A): Abstract 2554.
20. Tranaeus S, Shi XQ, Lindgren LE, Trollsås K, Angmar-Månsson B. In vivo repeatability and reproducibility of the quantitative light-induced fluorescence method. Caries Res. 2002; 36: 3-9.
21. Pretty IA, Hall AF, Smith PW, Edgar WM, Higham SM. The intra-and inter-examiner reliability of quantitative light-induced fluorescence (QLF) analyses. Br Dent J. 2002; 193: 105-9.
22. Heinrich-Weltzien R, Kühnisch J, Ifland S, Tranaeus S, Angmar-Månsson B, Stösser L. Detection of initial caries lesions on smooth surfaces by quantitative light-induced fluorescence and visual examination: an in vivo comparison. Eur J Oral Sci. 2005; 113: 494-8.
23. Pretty IA, Ellwood RP. Comparison of paired visual assessment and software analyses of changes in caries status over 6 months from fluorescence images. Caries Res. 2007; 41: 115-20.
24. Pretty IA. A review of the effectiveness of QLF to detect early caries lesions. Indianapolis, Indiana: Indiana University Press; 2005. p.253-90.
25. Baseren NM, Gokalp S. Validity of a laser fluorescence system (DIAGNOdent) for detection of occlusal caries in third molars: an in vitro study. J Oral Rehabil. 2003; 30: 1190-4.
26. Bamzahim M, Shi XQ, Angmar-Månsson B. Occlusal caries detection and quantification by DIAGNOdent and Electronic Caries Monitor: in vitro comparison. Acta Odontol Scand. 2002; 60: 360-4.
27. Francescut P, Zimmerli B, Lussi A. Influence of different storage methods on laser fluorescence values: a two-year study. Caries Res. 2006; 40: 181-5.
28. Ferreira-Zandoná AG, Ando M, Eggerston H. Clinical validation of caries detection methodologies: preliminary results. J Dent Res. 2004; 83 (Spec issue A): 2812a.
29. Lussi A, Firestone A, Schoenberg V, Hotz P, Sitch H. In vivo diagnosis of fissure caries using a new electrical resistance monitor. Caries Res. 1995; 29: 81-7.
30. Ricketts DNJ, Kidd EAM, Wilson RF. The effect of airflow on site-specific electrical conductance measurements used in the diagnosis of pit and fissure caries in vitro. Caries Res. 1997; 31: 111-8 .
31. Ricketts DNJ, Kidd EAM, Wilson RF. The electronic diagnosis of caries in pits and fissures: site specific stable conductance readings or cumulative resistance readings? Caries Res. 1997; 31: 119-24.
 Correspondence:
Correspondence:
Antonio Carlos Pereira
Faculdade de Odontologia de Piracicaba
FOP/UNICAMP
Departamento de Odontologia Social
Av. Limeira 901 - Areão - 13414-903 Piracicaba, SP, Brazil
E-mail: apereira@fop.unicamp.br
Received for publication: July 27, 2010
Accepted: February 10, 2011
