










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.10 no.1 Piracicaba Jan./Mar. 2011
ORIGINAL ARTICLE
The operator as a factor of success in ART restorations
Carolina da FrancaI; Viviane ColaresII; Evert van AmerongenIII
I PhD, Postdoctoral student, Faculty of Dentistry, University of Pernambuco, Brazil
II PhD, Associate Professor of Paediatric Dentistry, Faculty of Dentistry, University of Pernambuco, Brazil
III DDS, PhD, Professor of Paediatric Dentistry, Academic Centre for Dentistry in Amsterdam, The Netherlands
ABSTRACT
Aim: To evaluate the operator as a factor of success in atraumatic restorative treatment (ART) restorations. Methods: This was a clinical intervention study. The sample consisted of 271 glassionomer cement (Ketac Molar, 3M ESPE) restorations placed in 246 children aged 5 to 9 years attending public schools in Recife, Brazil. The operators were two senior undergraduate dental students and one dentist, classified as 'inexperienced' and 'experienced', respectively. Two groups of children were formed: one treated by the undergraduate students and the other treated by the dentist. The evaluation of the restorations took place at 1, 4 and 12 months by three senior undergraduate dental students. Results: Comparing the operators, a significant difference was found in class II cavities filled by students, who had a lower rate of success. There were no differences between the dentist and undergraduate dental students for class I cavities. Conclusions: The operator's experience makes a difference in the success rate of more complex ART restorations when an experienced operator receives the same training as an inexperienced operator.
Keywords: dental atraumatic restorative treatment, permanent dental restoration, longevity, primary dentition, operators.
Introduction
Atraumatic restorative treatment (ART) is an approach that was initially developed to provide preventive and restorative care to people in low-income countries. However, in the last few years, the use of ART has spread to countries such as the USA, England, Scotland and The Netherlands1. This technique has the advantages of reducing pain and fear2 and being more cost-effective than the traditional approach using amalgam3. However, the technique is still being studied aiming at increasing the survival of such restorations, especially on multi-surfaces. Some reasons for the less than satisfactory results are related to the operator.
In the literature, factors such as material4, type of cavity5-6 and cavity size7 have been associated with the longevity of ART restorations. In this paper, these factors associated with the operator will be discussed. It is important to bear in mind that, in the literature, the word 'operator' indistinctly refers to a dentist, a dental student or to any other oral health worker, each presenting different rates of successful outcomes.
Some authors cited non-compliance with the protocol for ART8, the professional qualification of the operator8, an inappropriate indication for ART9, the number of operators10, and the lack of a specific training course in ART11-13, as well as the experience of operator and assistant7, as factors that influence their performance. The training of operators (dentists) in ART has led to higher survival rates for these restorations14-15 Furthermore, in another study, when trained operators were dental students, longevity was lower16.
The operator's experience is another important factor to be considered in a deeper manner. A dentist has a wider experience of clinical interventions than a student. Despite a greater clinical experience, however, the dentist might not have had specific experience with ART restorations, or with the working conditions at schools. According to Kemoli et al.7 (2009), experienced operators and assistants in ART showed the best rate of survival for proximal ART restorations.
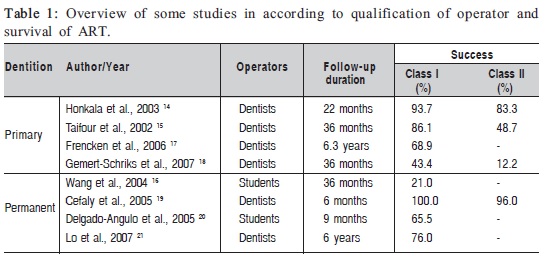
Considering dentition, some studies on permanent teeth showed the best results when the operator was a dentist and much less satisfactory results when the operator was a dental student (Table 1). In the studies with primary teeth, although the operator was always a dentist, the success rate varied greatly for both class II (from 12.2 to 83.3%) and class I (from 43.4 to 93.7%).
The aim of the present study was to evaluate the operator as a factor of success in ART restorations, especially considering clinical experience and specific training in ART restorations.
Material and methods
This study was carried out in public schools in Recife, capital of Pernambuco state, Brazil. Children aged 5 to 9 years presenting carious lesions involving one or two surfaces in primary molars were included in this study. The examination was performed using a mouth mirror and an explorer under natural light. The simplified World Health Organization (WHO) form was used to record information. Dental caries was recorded according to WHO criteria22.
The indication of ART was considered in cases of: (I) Class I or Class II cavities in primary molars, accessible by manual instruments; (II) absence of abscess or fistula near the carious tooth and no pulp exposure expected if caries was removed.
The operators were two senior undergraduate dental students and one dentist. In this study, the dentist was a practitioner with 5 years of experience. The students were senior undergraduate dental students in their final year. The dentist was an experienced and trained practitioner with over two hundred ART restorations performed, while the students had training with over thirty ART restorations but lacked experience with children and with clinical practice in general. The training consisted of getting informed about the ART technique and protocol, watching practical demonstrations of the technique and finally, applying this information in a short, supervised practice. After training, the trainee was able to perform restorations according to standard procedures. Although the training was essential for performing the ART protocol, it was limited to specific knowledge, while experience provided skills to manage the patient as a whole for both ART restorations and other clinical interventions in the school environment.
Two groups of children selected by random lottery were treated. One group was treated by the dental students and the other by the dentist. Treatment was carried out inside classrooms at the schools selected to take part in the trial. Patients were positioned on a table. After using cotton rolls to isolate the tooth, cavity opening was performed with a dental hatchet, the soft carious tissue was removed with an excavator, and the cavity and adjacent pits and fissures were filled with a glass-ionomer cement (Ketac Molar/3M ESP/ Germany). Caries removal followed the recommendations of Frencken et al.23, which preserved sound tooth tissue. Caries removal after cavity preparation was checked by conventional optical and tactile criteria. The conditioning of the cavity (using the liquid of glass-ionomer cement-Ketac Molar/3M ESPE) and adjacent pits and fissures with cotton wool pellets preceded the placement of the glass ionomer. The cavities were cleaned with three moist cotton wool pellets and dried with three other cotton wool pellets before and after the conditioning. The chair-side assistant, a dental student, mixed the glass-ionomer cement according to the manufacturer's instructions. The dental students who participated in this study had also been trained to mix the glass ionomer, but they were not experienced assistants. Class II cavities were filled after the placement of plastic bands and wedges. No local anesthesia was used. Excess material was removed by means of an applier/caver instrument, and the restoration was coated with a layer of petroleum jelly.
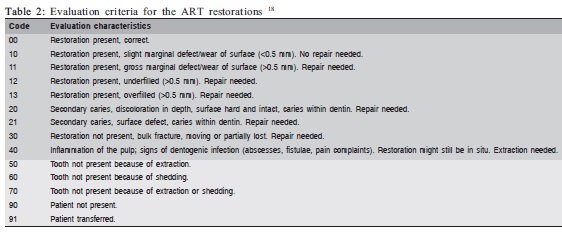
The evaluation of the restorations took place after 1, 4 and 12 months, according to previously defined criteria by Gemert-Schriks et al.18 (Table 2). Three trained and calibrated senior undergraduate dental students evaluated the restorations clinically using a CPITN probe, a mouth mirror and a headlamp. Restorations scored code 0 and 10 were considered successful, those scored codes 11-40 were considered failures, while restorations scored codes 50-90 were excluded from the analysis. A Kappa test was performed for intra- and inter-examiner evaluations. The Kappa test result was higher than 0.8. The evaluators were involved neither in the planning of the study nor in its execution.
Ethical approval was obtained from the Research Ethics Committee of the University of Pernambuco, Brazil (Protocol no. 190/08). The subjects were included in this study only after the parent or guardian had signed the respective informed consent form.
Results
The sample consisted of 271 restorations placed in 246 children of both genders aged 5 to 9 years, who were attending public schools in Recife, Brazil. The restorations were divided into two groups, 118 class I and 153 class II restorations. The loss in the sample was around 5.0%.
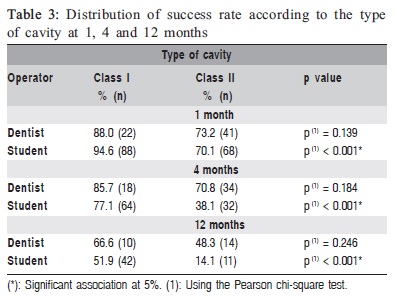
There were no statistically significant differences (p>0.05) between class I and II restorations performed by the dentist at any of the evaluation periods (1, 4 and 12 months). However, there was a lower success rate in the class II restorations performed by the students, revealing a statistically significant difference (p<0.05) (Table 3).
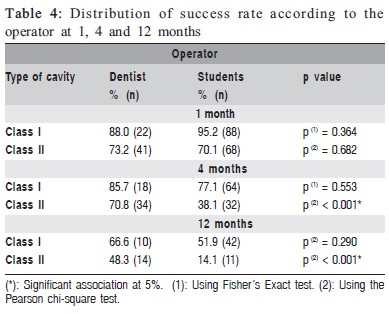
Comparing the operators, a significant difference (p<0.05) was found after 4 and 12 months in class II cavities filled by students, who had a lower rate of success. There were no significant differences (p>0.05) between the performance of the dentist and undergraduate dental students for class I restorations (Table 4).
Discussion
This study considered experience and specific training in ART restorations as factors related to operator that influence the longevity of these restorations.
The operator's experience in dental clinical procedures can give the best results in the survival of ART restorations10. The operator's professional skills, experience and training in the ART approach are decisive for treatment success because the clinical procedures will take place at schools, with the children positioned on ordinary tables, under conditions very different from those of the dental office setting.
Although the professional's general dental experience has formerly been considered a positive factor in the survival of ART restorations24, having specific ART training has subsequently been found as more efficient for the longevity of ART restorations than the dental professional's experience25.
With regard to the type of restoration and the operator, the results of the class II restorations showed a significantly lower success rate than those of class I, which is in agreement with a number of other studies4,21,26,28. However, in the present study, there was no difference between class I and II restorations performed by the dentist. Class II restorations performed by the students showed the worst results (p<0.001). This operator effect has also been observed for two-surface restorations by Gemert-Schriks et al.18, who reported that more complex restorations need more experienced operators. The suggestion is that inexperienced operators require further practice after they have completed their training. According to Kemoli and Amerongen27, prior to the operative stage of the study, any operator who had performed 50 ART restorations (half being class II and the rest of any other class) would be classified as 'experienced', and any operator who, after being trained, had done fewer than 10 but more than 5 restorations of any class would be classiûed as 'inexperienced' in the ART technique.
In the literature, the experience and training received by operators are not always clearly described, making these factors difficult to analyze. Furthermore, there are other number of factors related to the operator that are not clear in most studies such as the operator's experience with children, with the school environment or with the lack of infrastructure of the dental office.
Specific training and experience can be summed up as a combination of factors that associate the operator with success in ART, such as those cited by Frencken et al.24: the correct indication for ART, the appropriate mixing of the glass ionomer cement, and the judicious insertion of the material deep into the cavity. It seems that training and experience are complementary; while training helps the operator monitoring the protocol adopted, experience provides the clinical skills to facilitate the implementation of procedures, thus increasing the chances of success.
It may be concluded that clinical experience and specific training in ART restorations for operators remains a goal that has still to be achieved. The simple recognition that both factors are fundamental for achieving higher rates of survival of ART restorations represents per se a major step towards finding a solution to the problem of survival in ART restorations.
Acknowledgements
The authors are very grateful to the ACTA students who participated in this study, some of them as operators and others as evaluators. We also acknowledge the support given by 3M ESPE in providing the materials used in the study, and CAPES – Brazilian Ministry of Health's Federal Agency for Support and Evaluation of Graduate Education – for granting the PhD fellowship.
References
1. Topaloglu-Ak A, Eden E, Frencken JE, Oncag O. Two years survival rate of class II composite resin restorations prepared by ART with and without a chemomechanical caries removal gel in primary molars. Clin Oral Invest. 2009; 13: 325–32.
2. Carvalho TS, Ribeiro TR, Bonecker M, Pinheiro ECM, Colares V. The atraumatic restorative treatment approach: an "atraumatic" alternative. Med Oral Patol Oral Cir Bucal. 2009; 14: 668-73.
3. Seale NS, Casamassimo PS. Access to dental care for children in the United States. A survey of general practitioners. J Am Dent Assoc. 2003; 134: 1630-40.
4. Ercan E, Dülgergil T, Soyman M, Dalli M, Yildirim I. A field-trial of two restorative materials used with atraumatic restorative treatment in rural Turkey: 24-month results. J Appl Oral Sci. 2009; 17: 307-14.
5. Koenraads H, Van der Kroon G, Frencken JE. Compressive strength of two newly developed glass-ionomer materials for use with the Atraumatic Restorative Treatment (ART) approach in class II cavities. Dent Mater. 2009; 25: 551-6.
6. van't Hof MA, Frencken JE, van Palenstein Helderman WH, Holmgren CJ. The ART approach for managing dental caries: A meta-analysis. Int Dent J. 2006; 56: 345-51.
7. Kemoli AM, van Amerongen WE, Opinya G. Influence of the experience of operator and assistant on the survival rate of proximal ART restorations: two-year results. Eur Arch Paediatr Dent. 2009; 10: 227-32.
8. Frencken JE, Holmgren CJ. How effective is ART in the management of dental caries? Community Dent Oral Epidemiol. 1999; 27: 423-30.
9. Mickenautsch S, Grossman E. Atraumatic restorative treatment (ART) – factors affecting success. J Appl Oral Sci. 2006; 14(Sp. issue): 34-6.
10. Cefaly DFG, Tapety CMC, Mondelli RFL, Lauris JRP, Phantumvanit P, Navarro MFL. Three-year evaluation of the ART approach in class III and V restorations in permanent anterior teeth. Caries Res. 2006; 40: 389-92.
11. Holmgren CJ, Frencken JE. Painting the future for ART. Community Dent Oral Epidemiol. 1999; 27: 449-53.
12. Bresciani E. Clinical trials with atraumatic restorative treatment (ART) in deciduous and permanent teeth. J Appl Oral Sci. 2006; 14(Sp. Issue): 14-9.
13. Barata TJE, Bresciani E, Mattos MCR, Lauris JRP, Ericson D, Navarro MFL. Comparison of two minimally invasive methods on the longevity of glass ionomer cement restorations: short-term results of a pilot study. J Appl Oral Sci. 2008; 16: 155-60.
14. Honkala E, Behbehani J, Ibricevic H, Kerosuo E, Al-Jame G. The atraumatic restorative treatment (ART) approach to restoring primary teeth in a standard dental clinic. Int J Paediatr Dent. 2003; 13: 172-9.
15. Taifour D, Frencken JE, Beiruti N, Hof MA, Truin GJ. Effectiveness of Glass-Ionomer (ART) and Amalgam Restorations in the Deciduous Dentition: Results after 3 Years. Caries Res. 2002; 36: 437-44.
16. Wang L, Lopes LG, Bresciani E, Lauris JR, Mondelli RF, Navarro MF. Evaluation of Class I ART restorations in Brazilian schoolchildren: three year results. Spec Care Dent. 2004; 24: 28-33.
17. Frencken JE, Taifour D, Hof MA. Survival of ART and amalgam restorations in permanent teeth of children after 6.3 years. J Dent Res. 2006; 85: 622-6.
18. Gemert-Schriks MCM, Amerongen WE, Cate JM, Aartman IHA. Threeyear survival of single- and two-surface ART restorations in a high-caries child population. Clin Oral Invest. 2007; 11: 337-43.
19. Cefaly DFG, Barata THE, Tapety CMC, Bresciani E, Navarro MFL. Clinical evaluation of multisurface ART restorations. J Appl Oral Sci. 2005; 13: 15-9.
20. Delgado-Angulo EK, Ortiz EB, Sánchez-Borjas PC. Análisis de supervivencia de sellantes y restauraciones ART realizados por estudiantes de pregrado. Rev Estomatol Herediana. 2005; 15: 119-23.
21. Lo ECM, Holmgren CJ, Hu D, van Palenstein Helderman W. Six-year follow up of atraumatic restorative treatment restorations placed in Chinese school children. Community Dent Oral Epidemiol. 2007; 35: 387-92.
22. World Health Organization. Oral health surveys: Basic methods. Geneva: World Health Organization; 1997.
23. Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic restorative treatment (ART): rationale, technique, and development. J Public Health Dent. 1996; 56: 135-40.
24. Frencken JE, Makoni F, Sithole WD. ART restorations and glass ionomer sealants in Zimbabwe: survival after 3 years. Community Dent Oral Epidemiol. 1998; 26: 372-81.
25. Frencken JE, van't Hof MA, van Amerongen WE, Holmgren CJ. Effectiveness of single-surface ART restorations in the permanent dentition: a meta-analysis. J Dent Res. 2004; 83: 120-3.
26. Ersin NK, Candan U, Aykut A, Önçag O, Eronat C, Kose T. When primary molars lesions are cavitated into dentin, glass ionomer has similar 2-year survival to resin composite as a restorative material when using the "ART" technique. J Evid Base Dent Pract. 2008; 8: 24-5.
27. Kemoli AM, Amerongen WE. Inûuence of the cavity-size on the survival rate of proximal ART restorations in primary molars. Int J Paediatr Dent. 2009; 19: 423-30.
28. Ersin NK, Candan U, Aykut A, Önçag O, Eronat C, Kose T. A clinical evaluation of resin-based composite and glass ionomer cement restorations placed in primary teeth using the ART approach. J Am Dent Assoc. 2006; 137: 1529-36.
 Correspondence:
Correspondence:
Carolina da Franca
Rua Jacobina, 45/2102, Graças
Recife – PE – Brazil
E-mail: carolinafbandeira@yahoo.com.br
Received for publication: November 26, 2010
Accepted: March 28, 2011
