










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkBrazilian Journal of Oral Sciences
On-line version ISSN 1677-3225
Braz. J. Oral Sci. vol.10 n.2 Piracicaba Apr./Jun. 2011
ORIGINAL ARTICLE
Influence of the construction bite vertical and horizontal dimensions on dentoskeletal structures induced by the Klammt appliance in Class II treatment
Renata de Cassia GonçalvesI; Ary dos Santos PintoII; Dirceu Barnabé RaveliII; Luiz Gonzaga Gandini JuniorII; Aparecida Fernanda MelotiI
I PhD Student; Department of Orthodontics, Araraquara Dental School, UNESP – Univ. Estadual Paulista, Brazil
IIProfessor, Department of Orthodontics, Araraquara Dental School, UNESP – Univ. Estadual Paulista, Brazil
ABSTRACT
Aim: To evaluate the influence of construction bite in the dentoskeletal changes induced by Klammt Appliance. Methods: The sample consisted of 17 children, with Class II malocclusion and initial mean age of 8.5 years. The construction bite was obtained using an Exactobite on edge-toedge anteroposterior relationship with 3 mm interincisal clearance. The height of the acrylic was determined by initial overbite associated to interincisal clearance and measured with digital caliper. The amount of advancement was obtained and measured by initial overjet in the lateral radiography. Pearson's correlation, linear regression and ANOVA were used to determine the relationship between dentoskeletal and construction bite variables. Results: The increase in the height of the acrylic promotes a greater inhibition of the forward displacement of the nasal spine and reduction in the facial growth index. The increase in the mandibular advancement induces more downward displacement of nasal spine and pogonion; a counter-clockwise rotation of palatine plane; an increase in mandibular length, maxillary alveolar height and interincisal angle; a decrease in mandibular alveolar height, the intermaxillary discrepancy and overjet; and palatal tipping of upper incisors. Conclusions: The different dimensions of the construction bite influence the dentoskeletal changes induced by the appliance in Class II treatment.
Keywords:activator appliances, malocclusions, Angle Class II, cephalometry.
Introduction
Activator appliances change the function and the position of the mandible in order to transmit forces to the dentition and the basal bone1. The construction bite determines the amount of sagittal and vertical mandibular displacement of the appliance activation1-4. During the registration of the construction bite, the new position of the jaw must be analyzed in the three dimensions3,5-6.
The construction bites differ among studies in relation to the sagittal, vertical and transverse dimensions and the number of steps in advancement. Depending on the amount of anterior advancement of the mandible and the height of the acrylic occlusal shelf the Klammt appliance promote different dentoskeletal effects3,5.
The purpose of this study was to evaluate the influence of the vertical and horizontal dimensions of the construction bite in the dentoskeletal changes induced by Klammt Open Elastic Activator during the treatment of Class II division 1.
Material and methods
This study was approved by Research Ethics Committee of the Araraquara Dental School, UNESP, Brazil (protocol number 72/04) and informed consent was obtained from the parents of all children.
Sample Selection
Seventeen patients (7 boys, 10 girls) with initial mean age of 8.5 years for both genders were selected in the orthodontic clinical screening of the Araraquara Dental School, UNESP, Brazil. The initial mean age was 9.1 years for boys and 8.1 years for girls. The following selection criteria were used: Caucasian; Class II division 1 malocclusion characterized by initial value of the ANB angle greater than 4º and full Class II molar relationship; retrognathic mandible; permanent central and lateral incisors erupted or in the process of eruption; overjet larger than 3.5 mm; mesofacial or brachyfacial pattern. Additional criteria used the initial skeletal age under the pre-peak growth period as determined using the cervical vertebra maturation method described by Lamparski7.
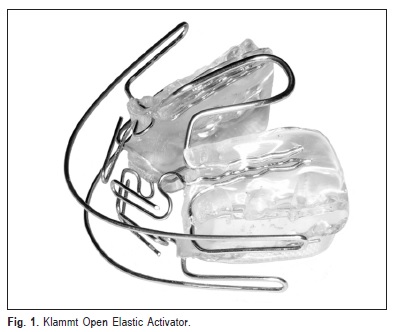
Characteristics of the appliances
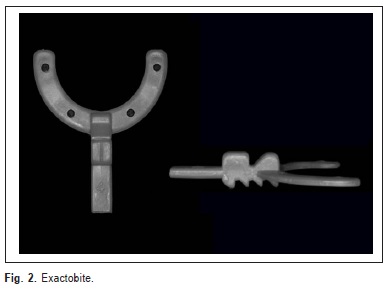
The appliance consisted of two acrylic resin blocks connected by a palatal arch, two upper and two lower anterior palatal guide wires, one upper and one lower labial arch and an acrylic occlusal shelf in contact with the occlusal surfaces of the canines and the posterior teeth (Figure 1). The construction bite registration was obtained using the Exactobite (Forestadent, Milton Keynes, Buckinghamshire, UK) in order to obtain a standardized registration for all patients in an edge-to-edge occlusion with 3 mm interincisal clearance (Figure 1). The forward positioning was determined by the initial overjet of the patient and the height of the acrylic is obtained by the initial overbite associated to the interincisal clearance of the Exactobite device. All children were instructed to use the appliance full time, except for meals and sports. The period of treatment was 13 to 14 months.
Cephalometric analysis
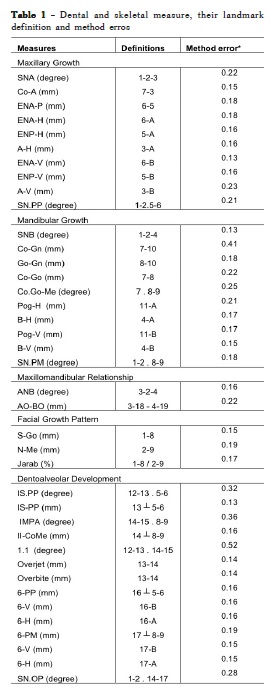
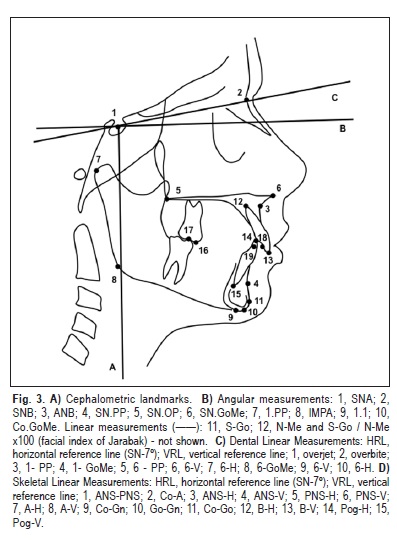
The lateral cephalometric radiographs were taken with the teeth in occlusion and the lips in a relaxed position using the Rotograph Plus MR05 Device (Villa Sistem Medical – Dental Line, Buccinasco, Mi, Italy). The radiographs were obtained in the beginning of the treatment and after 13 to 14 months of treatment. All cephalograms were digitized in the Numonics Accugrid light box and the measurements were obtained using the Dentofacial Planner Plus 2.02 (Dentofacial Planner Software Inc., Toronto, Canada) (Table 1, Figure 3).
Construction bite analysis
The vertical registration of the construction bite was obtained by measuring the heights of the acrylic occlusal shelf of the appliance with a digital caliper on both sides in the region of the molars (posterior) and canines (anterior). This height was obtained by the initial overbite associated to the interincisal clearance (3 mm) of the Exactobite device. The horizontal registration of the construction bite was measured by the amount of forward mandibular advancement according to the initial overjet obtained in the cephalometric radiographs. The analysis of the amount of mandibular advancement was obtained considering 10% of magnification in the measurement of the initial overjet obtained in the cephalometric radiograph.
Statistical analysis
It was used the SPSS software package (“Statistical Package for the Social Sciences" for Windows, version 14.0, SPSS Inc., Chicago, IL, USA). The method error was assessed using the Dahlberg's formula (Table 1). Descriptive statistics was calculated for description sample (Table 2) and description of the dimensions of the construction bite (Table 3). Pearson correlation coefficient was used to determine the relationship between the dimension of the construction bite and the dentoskeletal changes, linear regression model adjusted and ANOVA of the model was used to verify the dentoskeletal variables related to the dimensions of the construction bite and their predictive values (Tables 4-6).
Results
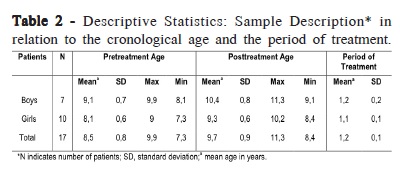
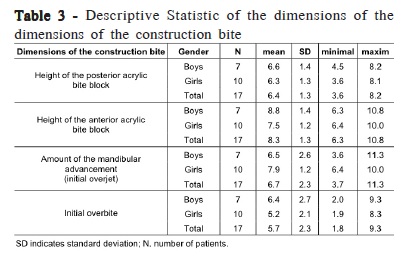
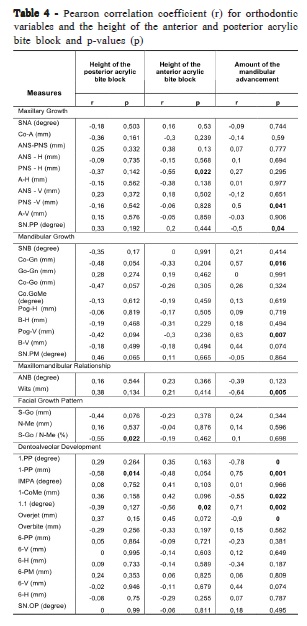
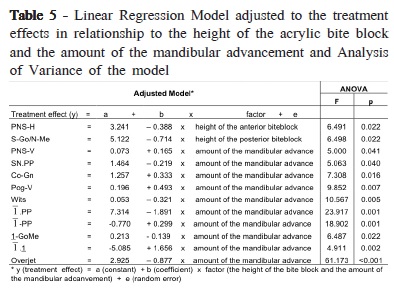
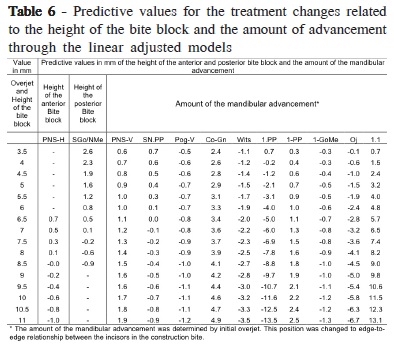
Table 2 shows the pretreatment age, the posttreatment age and the period of treatment using the appliance of Klammt for boys, girls and all children together. The table 3 shows the height of the posterior acrylic bite block (mean value=6.4 mm), the height of the anterior acrylic bite block (mean value= 8.3 mm), the amount of the mandibular advancement, i.e., initial overjet (mean value=6.7 mm) and initial overbite (mean value= 5.7 mm), characterizing the dimensions of the construction bite. Table 4 shows the variables that were related to the height of the anterior and posterior acrylic bite block determined by Pearson's correlation coefficient. Table 5 shows the treatment effects in relation to the height of the acrylic bite block and the amount of mandibular advancement adjusted by linear regression model and analysis of variance of the model. Table 6shows the predictive values for the treatment changes related to the height of the bite block and the amount of the advancement through the linear adjusted models.
Discussion
The initial mean age of all children was 8.5 years and the final mean age was 9.7 years. The initial mean age of the boys was 9.1 years and of the girls was 8.1 years. The final mean age of the boys was 10.4 years and of the girls was 9.3 years. The mean period of treatment was 1.2 years. The functional appliance relies on three basic functional components to promote vertical and sagittal skeletal and dentoalveolar changes: the biteplane or acrylic block (control of the eruption); the vestibular shields or screens (linguofacial muscle balance); and the construction bite (mandibular repositioning)8.
The acrylic blocks provide control of the vertical dentoskeletal development in various ways. One way of vertical control, is having the acrylic block in the posterior region, which provides disocclusion of the teeth removing the dental intercuspation and releasing the mandibular growth, thus improving the Class II relationship8-9. This kind of the vertical control is more indicated for the use of the Klammt activator because this appliance has no acrylic component in the anterior region. Another way of vertical control is inhibition of the eruption of the posterior teeth obtained by trimming the acrylic occlusal shelf in the lower occlusal surface. This not only permits relative increase of mandibular dentoalveolar height, but also results in relatively greater anterior movement of the posterior mandibular teeth, improving the Class II molar relationship. Finally, the vertical control could be obtained by restriction of the incisor eruption accomplished by the acrylic anterior coverage, promoting its relative intrusion and reduction of the overbite. The combination of trimming the posterior occlusal acrylic and the presence of the anterior acrylic allow eruption of the posterior lower teeth and inhibit the eruption of the anterior teeth. This combination is most indicated type of vertical control to the Bionator of Balters.
The mode of bite jumping depends on the “construction bite", which decides its position in the sagittal, vertical and transversal planes. In the vertical dimension, the magnitude of the construction bite (low, moderate and high) determines the amount of bite opening (i.e. the amount of downward position of the condyle)10. The literature shows that the height of the acrylic block can vary from 2 to 15 mm in the molar region according to the overbite3,8. Andresen's and Haupl's original concept maintains that condylar adaptation is induced by a loose appliance in which mandible is anteriorly displaced with the bite opening of 4 mm, or a minimal magnitude that is not beyond postural rest position. Contrary to the concept of minimal vertical opening, the viscoelastic properties of muscle and the stretching of soft tissue are decisive for activator action. This primarily requires dislocating the mandible not only in an anterior positioning, but also creating bite opening up to 10-15mm, well beyond the postural rest position. Between these two extremes, there are the modest bite opening of 4-6 mm, in an attempt to achieve the combined isometric muscle contraction and soft tissue stretching10.
In the present study, the height of the acrylic bite block was standardized using the initial overbite associated to the interincisal clearance (3 mm) of the Exactobite device. Thereby, it was obtained an acrylic bite block with a mean height of 8.3 mm in the canine region and 6.4 mm in the molar region (Table 3). Otherwise, when the construction bite is obtained by an incisal edge-to-edge position, it produces an acrylic bite block with height of 4.8 mm in the incisor area and molar separation of 3.7 mm3.
Previous studies9,11 with activator appliance showed an acrylic block with a height of 1-5 mm in the molar region. Woodside12 reported the use of an acrylic block with a minimum of 10 mm and a maximum of 15 mm of height. Furthermore, some researchers13-14 used an acrylic block with a height ranging from 2 to 5 mm in the incisor region. Regarding the Klammt appliance, some authors15-18used an acrylic block that was obtained using the edge-to-edge position in the incisor area, whereas Surber19, used 1 mm interincisal clearance in cases of increased overjet.
Our results showed that the increase in the height of the anterior acrylic block promotes inhibition of the anterior displacement of the posterior nasal spine, and the increase in the height of the posterior acrylic block promotes a decrease of the facial growth index (Tables 4-6). Luder11, and Noro et al.20 reported that the largest increase in the vertical dimension of the construction bite seems to be more effective to promote the horizontal mandibular growth.
In this study, the acrylic block was not trimmed in the inferior occlusal surface in order to control the eruption of posterior teeth8. In this case, the presence of the acrylic promoted a disocclusion between the upper and lower posterior teeth contributing for the sagittal correction21. This way, the vertical dentoalveolar development could be controlled without changing the inclination of the mandibular plane and also provide an additional increment of mandibular growth to the Class II correction9,12,22 In the first six months of use the Klammt appliance, there was a disocclusion in the posterior region. Therefore, in the last six months of use of the appliance, there was a natural contact between the upper and lower posterior teeth. This contact was observed when the overjet and the overbite were corrected. On the other hand, when the acrylic block is trimmed in the inferior occlusal surface of the molar region, both the alveolar growth and the eruption of the molar teeth are stimulated. Thus, this strategy may result in a modification of the mandibular plane inclination that tends to change the facial growth pattern, increasing the lower anterior facial height8-9.
The amount of the mandibular advancement depends on the size of the overjet can vary according to anatomical structures, such as the initial relationship of the molars, canines and incisors3. In the sagittal plane, the mandible might be advanced with varied magnitudes, from minimal, moderate, incisal edge-to-edge to even reverse overjet. The molar and canine relationships vary by region from the class I position (neutral position of occlusion) to the class III position (overcompensation of normal occlusion). The incisor relationships can be determined by the position of normal overjet, i.e., the lower incisors can be positioned from 1 to 3 mm behind the upper incisors (minimal advancement); moderate advancement (4 to 6 mm), the incisal edge-to-edge relationship; overjet reverse (the incisal relationship of class III or approximately 3 mm distal to the most protrusive position)3,9-10.
Mandibular advancement can be obtained by the following manners: 1) maximum advancement: single step advancement of 100% initial overjet throughout the treatment period9,17; 2) advancement in two steps, with a first advancement of 50% overjet during the first half of the total period of treatment and a second advancement of the remaining 50% during the second half of the period of treatment; and 3) incremental advancement (step-by-step advancement), with an advance of just 3mm every six weeks to reach the final position23-24.
Mandibular advancement to an edge-to-edge relationship between the incisors is suggested by some authors15-17,19 for the Klammt appliance. According to Solano-Reina18, mandibular advancement must not exceed the most protrusive position. Perez-Garcia et al.25 recommend advancement of the mandible to half the distance between the incisal edges, partly correcting the overjet and a second advancement correcting the remaining overjet.
In this study, the mandibular advancement obtained was maximum and single in a horizontal relationship of the incisors. In other words, the incisal face of the lower incisors was positioned in the same direction of the incisal face of the upper incisor. This position was obtained with the upper incisor touching the unique step of the upper part of the Exactobite device and the lower incisors were positioned in the second step of the lower part of this device. This horizontal position of upper and lower incisors provided a mean mandibular advancement of 6.7 mm (Table 3). The analysis of the amount of mandibular advancement should consider a 10% of magnification (0.67 mm) in the measurement of the initial overjet obtained in the cephalometric radiograph. All mandibular advancements were obtained in a symmetric way so the transverse relationship between the maxilla and the mandible was unchanged.
The results of this study showed the predictive values between the dimensions of the construction bite and the dentoskeletal effects using Linear Regression Model adjusted and Analysis of Variance of the model. Although the sample size was small these predictive values could be used as referential taking into consideration the limitations of this fact. The results showed that the larger mandibular advancement promotes greater vertical displacement of the posterior nasal spine and of the pogonion; counter-clockwise rotation of the palatal plane; increase in the total mandibular length, in the anterior maxillary alveolar height and in the interincisal angle; reduction in the intermaxillary discrepancy, in anterior mandibular alveolar height and in the overjet; and palatal tipping of the upper incisors (Tables 4-6).
The initial mean chronological age was 8.5 years for all patients. The initial mean chronological age was 9.1 years for boys and 8.1 years for girls (Table 2). Therefore, the analysis of the cervical vertebrae maturation showed that all patients, boys and girls, were in the pre-peak growth period. The initial mean overjet was 7.9 mm for females and 6.5 mm for males, showing a slight greater mandibular advancement in girls than in boys. On the other hand, it was observed an initial mean overbite of 5.2 mm for females and 6.4 mm for males, resulting in a greater deepbite for the boys than girls and consequently larger height of the anterior acrylic block in boys than in girls. There was no difference in the height of the posterior acrylic bite block in both genders (Table 3).
Mamandras and Allen26 observed greater total mandibular length in the larger anterior pogonion advancement group than in the small-advancement group. The greater length resulted in significantly more growth and consequently a straighter profile for these patients.
Table 6 gives the predictive values obtained in this study for the amount of dentoskeletal change that should be expected with Klammt treatment for every 0.5 mm of increase in the dimensions of the construction bite.
Based on the obtained results, it may be concluded that the different vertical and horizontal dimensions of the construction bite influence the dentoskeletal changes induced by the appliance in Class II treatment.
Acknowledgements
This study was supported by the FAPESP [2006/01138-2].
References
1. Bishara SE, Ziaja RR. Functional appliances: a review. Am J Orthod Dentofacial Orthop. 1989; 95: 250-58. [ Links ]
2. Clark WJ. Introduction to Twin Blocks. In: Clark W. Twin block functional therapy. Applications in dentofacial orthopaedics. Borgaro: Mosby-Wolfe; 1995.
3. Hamano Y, Ahlgren J. A cephalometric study of the construction bite of the activator. Eur J Orthod. 1987; 9: 305-313.
4. Skay J. Construction bite. How important is it? Inter J Orthod. 1984; 22: 19.
5. Bondi M, Scotti L. [Individualized bite construction for the activator]. Mondo Ortod. 1986; 11: 19-26.
6. Marín Manso GMFY, R.; Massón Barceló, R.M. Registro de mordida: Algunas consideraciones Rev Cubana Estomatol. 2005; 42. Available from: http://scielo.sld.cu/pdf/est/v42n2/est05205.pdf. [Access 2008 Jun].
7. Lamparski DG. Skeletal age assessment utilizing cervical vertebrae [thesis]. Faculty of the School of Dental Medicine, University of Pittsburgh; 1972.
8. Vig PS, Vig KW. Hybrid appliances: a component approach to dentofacial orthopedics. Am J Orthod Dentofacial Orthop. 1986; 90: 273-85.
9. Pfeiffer JP, Grobety D. A philosophy of combined orthopedic-orthodontic treatment. Am J Orthod. 1982; 81: 185-201.
10. Shen G, Hagg U, Darendeliler MA. Skeletal effects of bite jumping therapy on the mandible – removable vs. fixed functional appliances. Orthod Craniofac Res. 2005; 8: 2-10.
11. Luder HU. Skeletal profile changes related to two patterns of activator effects. Am J Orthod. 1982; 81: 390-6.
12. Woodside DG. Some effects of activator treatment on the mandible and the midface. Trans Eur Orthod Soc. 1973: 443-7.
13. Pancherz H. The mandibular plane angle in activator treatment. Angle Orthod. 1979; 49: 11-20.
14. Wieslander L, Lagerstrom L. The effect of activator treatment on class II malocclusions. Am J Orthod Dentofacial Orthop. 1979; 75: 20-6.
15. Eckardt L, Kanitz G, Harzer W. [The dental and skeletal changes in early Class II treatment with a Klammt open activator]. Fortschr Kieferorthop. 1995; 56: 339-46.
16. Klammt G. [The open activator]. Dtsch Stomatol. 1955; 5: 322-7.
17. Klammt G. [Working with the elastic open activator]. Fortschr Kieferorthop. 1969; 30: 305-10.
18. Solano Reina E. [Elastic activator appliances: Bimler's elastic appliance and Klammt's elastic activator]. Orthod Fr. 1992; 63: 373-80.
19. Surber H. [Preliminary therapeutic results with Klammt's “elastic open activator"]. Fortschr Kieferorthop. 1970; 31: 239-48.
20. Noro T, Tanne K, Sakuda M. Orthodontic forces exerted by activators with varying construction bite heights. Am J Orthod Dentofacial Orthop. 1994; 105: 169-79.
21. Altuna G, Woodside DG. Response of the Midface to Treatment with Increased Vertical Occlusal Forces - Treatment and Posttreatment Effects in Monkeys. Angle Orthod. 1985; 55: 251-63.
22. Harvold EP, Vargervik K. Morphogenetic response to activator treatment. Am J Orthod. 1971; 60: 478-90.
23. Banks PW, Wright J, O'Brien, K. Incremental versus maximum bite advancement during Twin-block therapy: A randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2004; 126: 583-8.
24. DeVincenzo JP, Winn MW. Orthopedic and orthodontic effects resulting from the use of a functional appliance with different amounts of protrusive activation. Am J Orthod Dentofacial Orthop. 1989; 96: 181-90.
25. Pérez-García LM, Saez Luna M.; Cadtillo Hernández R, Rolando Soto Cantero L, Grau Avalo R. Câmbios cefalométricos con el uso del activador de Klammt em diferentes magnitudes de protrusión mandibular. Rev Cubana Estomatol 2003, 40. Available from: http://bvs.sld.cu/revistas/est/ vol40_2_03/est02203.htm. [Access 2008 Ago].
26. Mamandras AH, Allen LP. Mandibular response to orthodontic treatment with the Bionator appliance. Am J Orthod Dentofacial Orthop. 1990; 97: 113-20.
 Correspondence:
Correspondence:
Renata de Cassia Gonçalves
Departamento de Ortodontia,
Faculdade de Odontologia de Araraquara, UNESP
Rua Humaitá, 1680 CEP: 14.801-903 - Araraquara, SP - Brasil
Phone: +55 (16) 3301-6342 Fax: +55 (16) 3301-6329
E-mail: renatacgoncalves@yahoo.com.br
Received for publication: October 29, 2010
Accepted: 31, 2011
