










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.10 no.2 Piracicaba Abr./Jun. 2011
ORIGINAL ARTICLE
Caries experience associated to social and preventive factors in children of a pastoral community from Limeira-SP
Maria Julia Pereira Coelho FerrazI; Dagmar de Paula QueluzII; Marcelo Corrêa AlvesIII; Carla Cristina Gonçalves dos SantosIV; Miriam Yumi MatsuiV
I MS, PhD, Post-doctorate researcher, Department of Community Dentistry, Piracicaba Dental School, State University of Campinas, Brazil
IIMSPH, PhD, Professor, Department of Community Dentistry, Piracicaba Dental School, State University of Campinas, Brazill
IIIMS, PhD student, Department of Morphology, Piracicaba Dental School, State University of Campinas, Brazil
IVSpeech Therapist, Limeira, SP, Brazil
VMS Student, São José dos Campos School of Dentistry, UNESP – Univ. Estadual Paulista, Brazil
ABSTRACT
Aim: To evaluate caries experience and prevalence associated to social and preventive factors in 3-6-year-old children of a Pastoral Community from Limeira, Brazil. Methods: A cross-sectional study was carried out through an epidemiologic research about the oral conditions of 110 children registered at the Children's Pastoral Community from the city of Limeira, SP, Brazil. Intraoral examination was performed by a trained dentist and the parents/caregivers filled out a questionnaire in order to outline the children's profile with respect to gender, parental education and oral health. Results: Differences related to gender were not detected (p= 0.3404). The most frequent periods of breastfeeding were 0 to 2 months (36.36%) and 2 to 6 months (35.45%), corresponding to 71.81% of the cases. The time bottle feeding pointed to two most frequent categories: 1) more than 12 months (35.45%) and 2) between 2 and 6 months (22.63%). Regarding parental education, the majority of the sample has not completed primary school (38.32%). It was observed a larger number of decayed teeth in male children (63.39%). Caries experience was significantly higher in children who were breastfed for only 2 months of life (41.96%). Children that did not use baby bottle or did not use a baby bottle for more than 1 year presented a smaller dmft, corresponding to 29.17% and 28.33%, respectively. Time of use of bottle and pacifier presented a significant association (p<0.05). Conclusions: The implementation of adequate strategies and actions is needed to reinforce oral health conditions in risk groups.
Keywords: dental caries, epidemiology, dental health surveys, school health services, dmft index, health promotion, oral health.
Introduction
With the advent of the Unified Health System (SUS) in the end of the 1980´s, a new challenge to the Brazilian public systems of oral health assistance was introduced, since the implementation of initiatives was recommended to follow models based on epidemiologic information of oral health1.
In order to monitor changes and trends in dentistry, Emerich and Castiel(2009)2 emphasized the new perspective for the dentist in the Family Health Program. The challenge is to prepare engaged professionals with a comprehensive view: the objective of their practice must be a collective goal, taking in account their social context and innumerable aspects of life and not just the detection of restricted signals and symptoms.
In Brazil, few studies concerning the prevalence of caries in primary dentition have been done in the past years, though the importance of the detection of decayed teeth for the evaluation of oral condition in children3. Dental caries is an important factor for the development of pain and functional disorders, which compromises esthetically the mouth4-5.
The most recent epidemiological survey of oral health promoted by the Ministry of Health confirmed the trend of decline of caries in Brazilian schoolchildren6.Therefore, it is important to understand the diversity related to needs in the field of dental care arises as a fundamental task for the planning of oral health services, aiming at greater equity7.
The multifactorial etiology of caries disease allows various types of interpretations about changes in caries prevalence according to time and level of development of the country. Some shifts would have originated from alterations in feeding habits (especially sugar consumption), alterations in oral hygiene, increased contact with fluoride, alteration in ecology and/or virulence of bacterial plaque microflora and change in protection mechanisms, including the immunological condition8-9.
Regarding the access to dental services, the difficulty in obtaining proper treatment results in accumulated experience of decayed, missing or filled permanent teeth (dmft). The most disadvantaged strata of the society is characterized by the need of treatment, while the strata of society with higher income level is characterized by executed treatment10-11.
The association between social and economic conditions (especially family income and level of education of household head) and caries prevalence has been observed in several studies, and children from families with high socioeconomic status often have less decayed teeth than children from families with lower socioeconomic status12, pointing to the pointing the need for comprehensive measures to address other common childhood health problems13.
This study evaluated dental caries experience and prevalence associated with social and preventive factors in 3 to 6 year-old children in Limeira, SP, Brazil.
Material and methods
A cross-sectional study of prevalence with a convenient sample was undertaken with 110 children aged 3 to 6 years old, with complete primary dentition, who were registered at the Children's Pastoral of the city of Limeira from August 2007 to December 2009, from a total of approximately 1,000 children distributed in 24 communities.
The research started after approval by the Research Ethics Committee of the School of Dentistry of Piracicaba, University of Campinas (protocol no. 144/2007).
After the establishment of protocol activities, authorization from the Coordinator of the Children's Pastoral of the city of Limeira was required. Contact with the leaders of communities was made, explaining the study proposes and also requesting their support for development of the study. The parents were asked to sign an informed consent form.
Children between 3 and 6 years old (both genders) were selected from the list of presence obtained from the Celebration of Life Day (a monthly event, when all children are weighed). Children that refused to participate, even with parental permission, as well as children who were not present in this event were not examined. In order to outline the children's profile with respect to gender, parental education and oral health prevention, data were collected by means of questionnaire that was filled out the children's parents/caregivers.
Intraoral clinical examination of each child was done by a single dentist. This examination was conducted under natural light, through visual inspection, with the child sitting in a chair facing the examiner. Gloves, head covers, masks, wooden spatulas, disposable gauze, as well as properly sterilized dental mirrors and periodontal probes (Community Periodontal Index – CPI) were used. Dental caries experience was evaluated by the dmft index according to World Health Organization's diagnosis criteria14.
Descriptive statistical analysis was calculated from measures from oral health and socioeconomic data. The dependent variable dmft was divided in dmft <3 and dmft > = 3, using as a reference descriptive statistics, which pointed this number as higher than average. The independent variables used in this study were: gender, duration and type (breastfeeding and bottle-feeding) of nursing, pacifier use, finger sucking and parental education. The significant association between the dependent and independent variables was tested by bivariate analysis (chi-square), with a significance level of 0.05.
Regarding the strength and direction of association, the odds ratio (OR) was used. In order to find association between the variables supposedly related to caries experience, Fisher's test, with significance level of 0.01, was used to analyze the possible association between: duration and type (breastfeeding and bottle-feeding) of nursing,; the presence and absence of pacifier habit or sucking habits; and the dmft. SAS (SAS/ STAT® Software, Campus Drive Cary, NC, USA) was the program used for the statistical analysis15.
Results
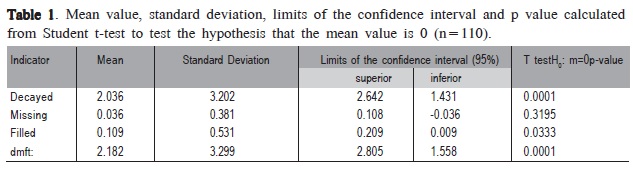
The final sample consisted of 110 children from six communities of the Children's Pastoral of the city of Limeira. Strong evidence was identified (p <0.01) for the existence of average higher than zero for number of cavities and dmft per child, besides the evidence (p <0.05) of the existence of difference between average zero and number of fillings. No evidence was found (p = 0.3195) between average zero and number of extractions (Table 1).
Table 2 provides an analysis of demographic characteristics used as determinants of oral health in this study. No evidence of differences between the children in relation to gender is present (p: 0.3404).
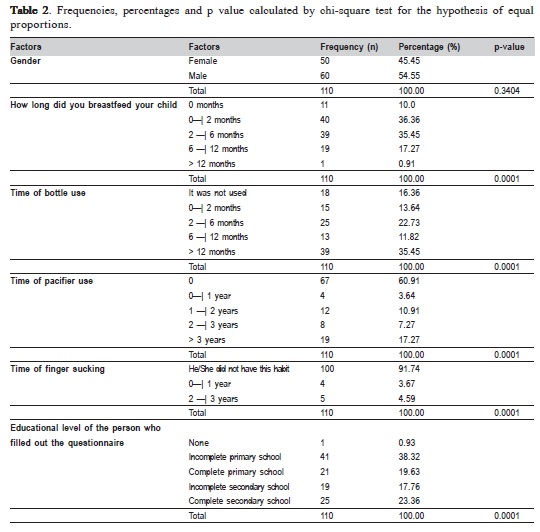
Strong evidence that the differences between the true proportions of children according to all other factors (duration of breastfeeding, bottle feeding time, duration of pacifier use, thumb sucking time and parents' schooling level) was found.
Regarding the duration of breastfeeding, it was observed that the periods of 0 to 2 months (36.36%) and 2 to 6 months (35.45%) are the most frequent, together accounting for 71.81% of the cases. The time of baby bottle use can be divided into two most frequent groups: those who used it for more than 12 months (35.45%) and those who used it for a period lasting between 2 and 6 months (22.63%). The second group showed a lower frequency than the first, but still stands out in relation to others that ranged between 11.82 and 16.63%.
Regarding the duration of pacifier use, most children (60.91%) did not use it, with a relatively even distribution within the periods. In relation to finger sucking, this habit can be considered as a rare practice since only 8.26% of the sample acquired the habit against 91.74% who did not.
Finally, in terms of education of the person that filled out the questionnaire (parent/caregiver), the majority of the sample did not complete primary school (38.32%) while the rest were roughly evenly distributed: 17.76% did not complete secondary school, 19.63% completed the primary school and 23.36% completed secondary school. Only one person did not attend any formal education.
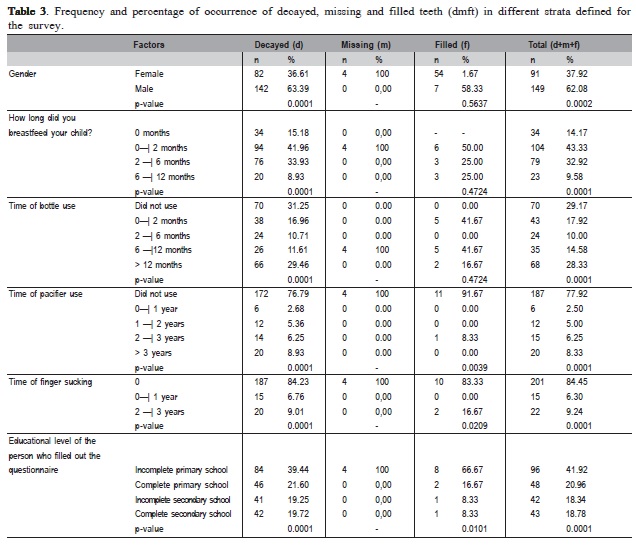
Table 3 presents the comparison of the frequency and proportions of oral health indicators: number of cavities (d), number of missing teeth (m) and number of filled teeth (f), which together comprise the indicator of caries experience in the primary dentition (dmft). It can be initially observed that there were a larger number of decayed teeth in male children (63.39%), a proportion that is significantly higher than in females (36.61%). Interestingly, the quantification of missing teeth according to gender showed that all four extractions happened in girls (100.0%). The proportion of filled teeth did not differ significantly between the genders, while the dmft, influenced by the component number of decayed teeth, is significantly higher in male children.
In relation to breastfeeding, it was observed that caries experience was significantly higher in children who were breastfed up to the age of 2 months 41.96%). Children who did not use baby bottle or who did not carry this habit for more than 1 year had a smaller percentage of dmft: 29.17% and 28.33% respectively.
Pacifier use (76.79%) and finger sucking (84.2%) suggested that they do not interfere in the caries experience, since those with decayed teeth did not have these habits.
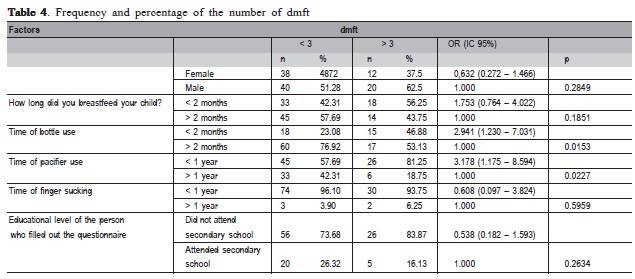
Table 4 shows the results of bivariate analysis for dmft. The duration of bottle feeding and pacifier use showed a significant association (p <0.05). OR (odds ratio) indicated that the bottle use for less than two months is not harmful and that it is associated with a higher probability (rate of 1.753) of having a dmft value lower than 3. Similarly, pacifier use for less than 1 year was not harmful either and increased by 2.941 times the probability of having a dmft value lower than 3.
Discussion
Developing oral health strategies directed to groups of population requires knowledge, which can be obtained from epidemiology. The basic condition for this is the use of various instruments according to the characteristics of each disease or condition, in order to obtain a better approximation to the real conditions of oral health16.
In order to access the prevalence and severity of caries according to WHO recommendations, this study used the dmft index. This index counts the primary teeth somehow affected by caries (decayed, missing or filled). Based on this information, it was possible to evaluate the oral health and particularly caries experience in children from the city of Limeira associating them with oral habits and parental level of education. For evaluations at the individual level, the variable was defined by the involvement of at least one primary tooth with untreated caries (component "d" of the dmft > 3), and evaluations at the collective level, the variable was defined by the proportion of children presenting this condition in each area. This study confirmed the existence of average significantly higher than 0 for the number of caries and dmft per child, not reaching the goals recommended by WHO for the year 2000 or corroborating the last survey sponsored by the Ministry of Health in 20106. Furthermore, this provides information for dental caries prevention and the attention about access to dental treatment, since it can be observed that children who need treatment present few filled teeth16.
In relation to habits associated with caries experience, it was found that pacifier use was not related to caries experience in this study since 60.91% did not use a pacifier. This finding disagree with those of Yonezu and Yakushiji (2008)17 and Vázquez-Nava et al. (2008)18 who found that pacifier use for 18 months of life is a risk factor for caries development and that this risk is two times greater in children who use pacifiers compared to those who do not have this habit. Anyway, considering the aspect of craniofacial growth (open bite, crossbite, inadequate posture of the tongue, articulation alterations), pacifier use can be related to dentofacial changes and depends on the duration, frequency and intensity of habit19-20. In relation to finger sucking, 91.74% of children did not have acquired this habit, which is consistent with Castilho and Rocha (2009)20 who reported that the pacifier is used not just to calm down, but can also be offered in order to prevent the habit of finger sucking.
Regarding breastfeeding, only 35.45% of children were breastfed during the period of 2-6 months of life, emphasizing the importance of encouraging this healthy practice. Breastfeeding favors growth and development of children, not only for their nutritional, immunological and psychological aspects but also because it enables the harmonious growth of the face, promoting the maturation of the stomatognathic system functions21-22. In this study, however, it was found that breastfeeding in a period from 6 to 12 months suggested a protection against caries. Children who used the bottle for a period longer than 12 months presented a higher dmft value. According to the literature the use of the bottle is a very common practice in 62.8% of children under the age of 1 year in Brazil7. Data from the latest research of oral health in Brazil23, which showed that dmft was 2.80, can be compared to the finding of the present study (average of 2.18). It can also be observed an inequality in the distribution of decayed component (2.03), filled (0.109) and missing teeth (0.03). It is suggested that the access to dental services for the population represented by this sample is not satisfactory since a small number of restored teeth were observed, confirming Gomes, et al. (2004)24.
It is important to emphasize that the impact of health services in disease prevention is still controversial. Defenders of the role of services argue that access to effective treatments can reduce the level of disease25. However, the effectiveness of preventive interventions, even when proven in controlled clinical trials under ideal conditions, is not always confirmed in the day-to-day services, under realistic conditions26-27. Only 3% of the decline of caries between the 1970s and 1980s in developed countries can be attributed to dental services, while 65% were explained by large improvements in socioeconomic conditions28. This study shows that children assisted by the Children's Pastoral of Limeira belong to poor families, being educated by parents with incomplete schooling. Considering that oral health education should begin early in life, it an integrated approach is important including social communication improvement and professionals of general and oral health training, aiming to educate families, especially mothers13,29-30.
Dental caries experience in communities of the Pastoral of the city of Limeira emphasizes the importance of maintenance and continuity of the potential capacity of local agents. In general, the obtained results suggest an association of social issues with inequities in oral health, as indicated actions integrating public health care policies. In addition, this study reflects the importance of referral of the most vulnerable and/or more exposed groups to risk factors to services focused on oral health promotion.
Acknowledgments
The authors thank the Childrens Pastoral of the city of Limeira for their support in developing this study.
References
1. Roncalli AG, Frazão P, Pattussi MP, Araújo IC, Ely HC, Batista SM. Projeto SB2000: uma perspectiva para a consolidação da Epidemiologia em Saúde Bucal Coletiva. Rev Bras Odontol Saude Coletiva. 2000; 1: 9-25. [ Links ]
2. Emmerich A, Castiel LD. Jesus tem dentes metal-free no país dos banguelas? Odontologia dos desejos e das vaidades. Hist Cienc Saude- Manguinhos. 2009; 16: 95-107.
3. Noro LRA, Roncalli AG, Mendes Júnior FIR, Lima KC. A utilização de serviços odontológicos entre crianças e fatores associados em Sobral, Ceará, Brasil. Cad Saude Publica. 2008; 24: 1509-16.
4. McGrath C, Broder H, Wilson-Genderson M. Assessing the impact of oral health on the life quality of children: implications for research and practice. Community Dent Oral Epidemiol. 2004; 32: 81-5.
5. Antunes JLF, Peres MA, Mello TRC. Determinantes individuais e contextuais da necessidade de tratamento odontológico na dentição decídua no Brasil. Cienc Saude Coletiva. 2006; 11: 79-87.
6. Ministério da Saúde. Projeto SB Brasil 2010: pesquisa nacional de saúde bucal 2010. Brasília: Ministério da Saúde; 2010. Available from: http:// www.sbbrasil2010.org.
7. Lucas SD, Portela MC, Mendonça LL. Variações no nível de cárie dentária entre crianças de 5 e 12 anos em Minas Gerais, Brasil. Cad Saude Publica. 2005; 21: 55-63.
8. Peres KG, Bastos JR, Latorre MR. Severidade de cárie em criançase relação com aspectos sociais e comportamentais. Rev Saude Publica. 2000; 34: 402-8.
9. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007; 369: 51-9.
10. Pinto VG. Saúde bucal coletiva. 4.ed. São Paulo: Santos; 2000.
11. Maltz M, Silva BB. Relação entre cárie, gengivite, fluorose e nível socioeconômico em escolares. Rev Saude Publica. 2001; 35: 170-6.
12. Galindo EMV, Pereira JAC, Feliciano KVO, Kovacs MH. Prevalência de cárie e fatores associados em crianças da comunidade do Vietnã, Recife. Rev Bras Saude Mater Infant. 2005; 5: 199-208.
13. Melo MMDC, Souza WV, Lima MLC. Fatores associados à cárie dentária em pré-escolares do Recife, Pernambuco, Brasil. Cad. Saude Publica. 2011; 27: 471-85.
14. World Health Organization. Oral health surveys, basic methods. 4th ed. Geneve: WHO; 1997.
15. SAS. Institute Inc. The SAS System, release 9.2 TS Level 2M0. SAS Institute Inc., Cary: NC; 2008.
16. Narvai PC, Biazevic MGH, Junqueira SR, Pontes ERCJ. Diagnóstico da cárie dentária: comparação dos resultados de três levantamentos epidemiológicos numa mesma população. Rev Bras Epidemiol. 2001; 4: 72-80.
17. Yonezu T, Yakushiji M. Longitudinal study on influence of prolonged nonnutritive sucking habits on dental caries in Japanese children from 1.5 to 3 years of age. Bull Tokyo Dent Coll. 2008; 49: 59-63.
18. Vázquez-Nava F, Vázquez RE, Saldivar GA, Beltrán GF, Almeida AV, Vázquez RC. Allergic rhinitis, feeding and oral habits, toothbrushing and socioeconomic status. Effects on development of dental caries in primary dentition. Caries Res. 2008; 42: 141-7.
19. Silva EL. Hábitos bucais deletérios. Rev Para Med. 2006; 20: 47 50.
20. Castilho SD; Rocha MAM. Uso de chupeta: história e visão multidisciplinar. J Pediatr. 2009; 85: 480-9.
21. Palmer B. Influence of breastfeeding on the development of the oral cavity. J Hum Lact. 1998; 14: 93-8.
22. Coelho Ferraz MJP. Respirador Bucal - uma visão multidisciplinar. São Paulo: Lovise; 2004.
23. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação Nacional de Saúde Bucal. Projeto SB Brasil 2003. Condições de Saúde Bucal da População Brasileira 2002- 2003. Resultados principais. Brasília: Ministério da Saúde; 2004.
24. Gomes PR, Costa SC, Cypriano S, Sousa MLR. Dental caries in Paulínia, São Paulo State, Brazil, and WHO goals for 2000 e 2010. Cad Saude Publica. 2004; 20: 866-70.
25. Andrulis DP. Access to care is the centerpiece in the elimination of socioeconomic disparities in health. Ann Intern Med. 1998; 129: 412-6. 26. Rychetnik L, Frommer M, Hawe P, Shiell A. Criteria for evaluating evidence on public health interventions. J Epidemiol Community Health. 2002; 56: 119-27.
27. Victora CG, Habicht JP, Bryce J. Evidence-based public health: moving beyond randomized trials. Am J Public Health. 2004; 94: 400-5.
28. Nadanovsky P, Sheiham A. Relative contribution of dental services to the changes in caries levels of 12-year-old children in 18 industrialized countries in the 1970s and early 1980s. Community Dent Oral Epidemiol. 1995; 23: 331-9.
29. Sheiham A. The role of the dental team in promoting dental health and general health through oral health. Int Dent J. 1992; 42: 223-8.
30. Freire MCM; Macedo RA.; Silva WH. Conhecimentos, atitudes e práticas dos médicos pediatras em relação à saúde bucal. Pesq Odont Bras. 2000; 14: 39-45.
 Correspondence:
Correspondence:
Dagmar de Paula Queluz
Departamento de Odontologia Social
Faculdade de Odontologia de Piracicaba
UNICAMP Avenida Limeira, 901 CEP 13414-900 Piracicaba SP BR
Phone: +55 19 21065277 Fax: +55 19 21065218
E-mail: dagmar@fop.unicamp.br
Received for publication: February 03, 2011
Accepted: June 16, 2011
