










 Inglés
Inglés




 Permalink
PermalinkBrazilian Journal of Oral Sciences
ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.1 Piracicaba ene./mar. 2012
ORIGINAL ARTICLE
Atraumatic Restorative Treatment used for caries control at public schools in Piracicaba, SP, Brazil
Cristina GibiliniI; Janice Simpson de PaulaI; Regina MarquesII; Maria da Luz Rosário SousaIII
IPhD Student, Graduate Program in Dentistry, sub-area Dental Public Health, Department of Community Dentistry, Piracicaba Dental School, University of Campinas, Brazil
IIPhD in Public Health and Oral Health Coordinator of the Municipality of São Paulo, Brazil
IIIProfessor, Department of Community Dentistry, Piracicaba Dental School, University of Campinas, Brazil
ABSTRACT
AIM: The aims of this study were (1) to evaluate the Atraumatic Restorative Treatment (ART) as a measure to control caries at public schools in Piracicaba, SP, Brazil, discussing the importance of the promotion of individual and collective health and (2) to evaluate the longevity of ART restorations in the first six months after placement.
METHODS: The sample consisted of 173 schoolchildren aged 5 to 10 years from public schools in Piracicaba, treated according to ART approach and reassessed after six months.
RESULTS:It could be observed that after ART, a large part of the students initially fitted into risk E classification (high caries risk) were reclassified into risk B classification (moderate caries), characterized by the presence of restored teeth only (caries free teeth; c = 0). In addition, 81.78% success rate was obtained after six months of ART.
CONCLUSIONS: ART was considered effective in health promotion programs, given its importance as a measure to control caries in schoolchildren.
Keywords: dental atraumatic restorative treatment, dental caries, public health.
Introduction
Although dental caries prevalence has declined significantly over the last few years, it is still considered a public health problem in Brazil and worldwide. This fact is confirmed when the data of the last national epidemiologic survey are analyzed, indicating that among 5-year-old children approximately 60% presented at least one primary tooth with caries experience, and 70% of the 12-year-olds presented caries in their permanent dentition1.
In view of this situation, dental control and follow-up are necessary during childhood and adolescence for preventing or attenuating the affections caused by caries disease. With the goal of encouraging health promotion measures required for caries control and prevention, the World Health Organization (WHO) proposed the program of Atraumatic Restorative Treatment (ART) for countries with economically underprivileged or marginalized communities2. ART has been considered a feasible treatment option, as it is based on the contemporary philosophy of minimum intervention and maximum preservation of the tooth,and can be applied to the entire population. ART consists of a simplified, low-cost technique that uses only hand instruments in the removal of carious tissues to reduce contamination and viability of microorganisms3, and requires immediate restoration of the cavity with and adhesive restorative material, namely glass ionomer. Moreover, the ART approach causes less anxiety in children than the traditional restorative approach2,4.
It is worth mentioning that the use of high-viscosity glass ionomer cements has been outstanding, as it facilitates the technique and reduces the technical difficulties, especially in public services5. In this context, studies have pointed out the clinical performance of the glass ionomer cement Ketac Molar® (3M ESPE)6-7. Other studies have found better results for glass ionomer over conventional amalgam in restorations in primary teeth8-10.
Because of properties such as continuous fluoride release and fluoride ion recharging capacity, glass ionomer cements act as a constant reservoir of fluoride in the oral cavity, and participate in the de- and remineralization processes, contributing to the good clinical performance of the restorations8.
Various longitudinal studies have been conducted to assess the efficacy of ART. Frencken et al.11 (1996) and Holmgren et al.12 (2000) evaluated the longevity of restorations in Class I and II cavities for a period of 3 years with satisfactory results in 88.3% and 92% of them, respectively, in primary and permanent teeth. Other longitudinal studies using ART have shown various long-term success rates using Ketac Molar® (3M ESPE), with results that reach up to 21% of success within 36 months in permanent teeth12. Van Germert-Schriks et al.13 (2007) found 43.4% success for oneface restorations and 12.2% for two-face restorations, using the same restorative material and same period of evaluation.
Research studies have indicated ART as an effective method in the control of caries disease, with low operating costs, but further studies are necessary to evaluate its application in public health, including a more comprehensive assessment of the participants' oral health. It should be noted that collective environments such as schools are ideal spaces for oral health promotion actions, as they allow the development of group activities and contribute to the control and evaluation of interventions. In this context, the verification of caries activity is emphasized. The early diagnosis of incipient caries lesions at a reversible stage not only permits evaluating the determinant factors, but also helps determining the caries risk, which makes the treatment simpler, less invasive and less expensive based on the use of fluoride and changes in the patient's behavior with respect to diet and oral hygiene14. Thus, careful determination of caries risk is necessary so that preventive actions and specific control may be directed towards high-risk individuals even before the lesions develop15. Caries risk assessment can be made both in the clinical environment and in other collective spaces16.
The use of ART in schoolchildren may help fulfilling the demand in public services as this approach allies a faster treatment outcome compared with conventional treatment17-19 with caries control, which is of particular interest for children at higher risk for developing caries. Thus, the aim of the present study was to evaluate ART as a measure to control caries in public schools in Piracicaba, São Paulo, considering the longevity of restorations in the first six months after treatment, as well as discussing the importance of promoting public health.
Material and methods
The present study was first sent to the Research Ethics committee of the Piracicaba School of Dentistry (University of Campinas) for appreciation, and was approved under Protocol No. 106/2009. The children's and parents'/guardians' consent was obtained.
The convenience sample analyzed 1,167 children in the age range between 5 and 10 years old. A total of 173 schoolchildren with indication for ART were included, totalizing 330 teeth. The children came from six public schools (Olívia Caprânico, José Pousa de Toledo, Benedito de Andrade, Francisco A. Kronka, Antônio Rodrigues Domingues and Melita L. Brasiliense) in the municipality of Piracicaba, São Paulo, which participate in prevention programs.
The Municipality of Piracicaba is located 160 km from São Paulo, in the southwestern region of the state, and has 368,029 inhabitants20. It has had fluoridated public water supplies since 197121 and at present 99.38% of residents are favored with water supply20. The Human Development Index (HDI) of the municipality was 0.836 in 200019-20. The mean dmft index ("d"-decayed; "m"-missing;"f"-filled; "t"-teeth) among preschool children was 1.30 in 200622 and 1.32 in 201023.
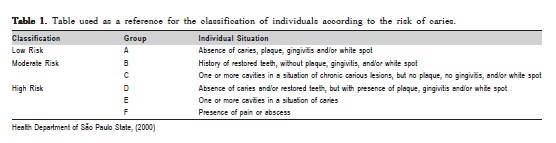
Before treatment, an epidemiologic survey of dental caries was conducted to obtain the children's dmft and caries risk classification, as well as to verify the caries cavities with indication for ART. The dmft index was determined in accordance with the WHO criteria24 and the caries risk evaluation was obtained in accordance with the criteria of the State Secretariat of Health16, according to which the schoolchildren are classified into five different categories: A (healthy teeth), B (presence of restoration), C (presence of chronic caries), D (presence of plaque, gingivitis or white spot lesion), E (presence of acute caries) and F (urgency)
(Table 1).
The criterion used for the indication of ART followed the criteria described by Frencken et al.2 (1996), with evaluation of primary teeth only. Thus, teeth with cavited dentin caries lesion that could be accessed with a 0.9-mmdiameter excavator were included. Teeth with evident pulp involvement or painful symptomatology were excluded from the sample. A trained dentist performed ART in accordance with the protocol proposed by Frencken et al.2 (1996). The treated caries cavities were restored with glass ionomer Ketac Molar® (3M ESPE), in accordance with the manufacturer's instructions.
The longevity of ART restorations at 6 months wasevaluated according to the criteria proposed by Taifour et al.8 (2002), with the use of a flat oral mirror and CPI probe by a single calibrated examiner, with intra-examiner agreement of 84.2%. The criteria used for evaluating the restorations were described and grouped into 3 categories8,25: a) success (restorations present with a maximum of 0.5 mm marginal defect); b) failure (restorations with a marginal defect >0.5mm, fracture of the restoration or tooth, restoration completely lost); and c) not evaluated (absent due to natural exfoliation of the tooth or replacement of the glass ionomer restoration by another type of restorative material) or excluded (children who missed the evaluation visit, moved to another school or completed primary schooling in the period between baseline and reevaluation).
The data were tabulated and analyzed by descriptive statistics, using the SPSS software (SPSS Inc., Shicago, IL, USA) version 17.0.
Results
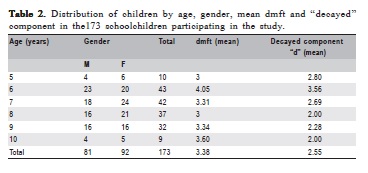
It could be observed that among the 173 schoolchildren subjected to ART, 81 (46.82%) were boys and 92 (53.18%) were girls. The mean age was 7.36 years (SD 1.36), ranging between 5 and 10 years. The descriptive data are presented in Table 2.
At the time of the epidemiologic survey (baseline) the children selected for treatment according to ART presented a dmft equal to 3.38, with mean number of decayed teeth equal to 2.55. After treatment, the children were re-evaluated and presented a mean of the ‘decayed' component of dmft equal to 0.72.
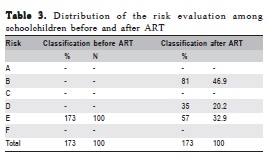
In addition, in the previous survey, the schoolchildren were classified with regard to the criterion of risk16 and reclassified after ART had been performed. In the first evaluation, all participants fitted into the risk E classification, due to the presence of carious teeth. After ART, a large part of the schoolchildren were re-classified into risk B, characterized by the presence of restored teeth only (no caries lesions). Nevertheless, it is worth pointing out that even with the reclassification, 53.1% of the schoolchildren presented teeth without indication for ART, but with the need for curative and/or preventive treatment. Thus, 20.2% of the participants still presented white spot lesions, plaque or gingivitis in some teeth, fitting into risk D classification. The remainder of the schoolchildren (32.9%) still presented carious teeth with contra-indication for ART, keeping them in risk E (presence of acute cries), as demonstrated by the distribution in Table 3.
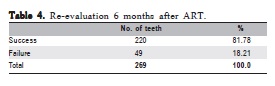
Six months after the initial treatment, a new evaluation/follow-up was performed (Table 4). Thus, 36 (10.9%) of theteeth re-evaluated presented another type of restorative material, or had exfoliated naturally, and 25 teeth (7.6%) were not evaluated because the children had moved to another school, making longitudinal evaluation of the restoration impossible. Therefore, 269 (81.51%) of the 330 teeth initially treated were re-evaluated 6 months after treatment with a success rate of 81.78%.
Discussion
From the 173 schoolchildren subjected to ART, 67% shifted from caries risk classification E (acute caries) to risk classification B (restoration) or D (white spot lesion, plaque and/or gingivitis). These data demonstrate that ART per se improved the oral status of a large percentage of the children treated, as described by Frencken et al.5 (2010). Nevertheless, among the schoolchildren that shifted from risk E to risk D (20.2%), implementation of educational measures allied with motivation to perform oral hygiene is still necessary to decrease the prevalence of biofilm, white spot lesions and gingivitis. Thus, the children fitted into risk D could, by means of simpler actions than ART, shift into risk B with improved oral health, and consequently, quality of life. Therefore, ART must be considered a measure for promoting public health and should be performed in conjunction with practices in health education and preventive programs to be effective in controlling the etiologic factors of caries26-27. Furthermore, in spite of ART, 32.95% of the schoolchildren remained in the risk E classification, that is, continued to have caries, which could be justified by two situations: 1) teeth with cavities with pulp involvement or painful symptomatology (contraindicated for ART); 2) presence of carious permanent teeth, not included in the indications for ART in this study.
In spite of the mentioned factors, an improvement in the schoolchildren's oral health was observed by the reduction in the mean of the ‘decayed' component of dmft from 2.55 to 0.72, proving the effectiveness of this type of treatment.
ART improves the oral status, preventing caries progression to more complex levels, such as the need for endodontic treatment and extractions. This occurs because ART fits into the concept based on the prevention and early interception of the caries process, with the goal of performing interventions that are as conservative as possible2,11,28. In addition, the treatment allows a reduction in the level of Streptococcus mutans in the oral cavity, and consequently, the risk of new carious lesions3.
Considering the large number of children that wait for treatment at the Family Health Units or Basic Health Units, ART can collaborate significantly in fulfilling the demand of these pediatric patients, being an important form of caries control and prevention in the Family Health Program5,29-30.
It is also worth emphasizing that as a low-cost, simple and fast (mean of 6 min per restoration) technique ART may optimize the time and human resources that would be required, for example, to transport these children to a location outside the school environment during treatment, as has been described by Figueiredo et al.29 (2004); Schriks and Amerongen17 (2003) and Pellegrinetti et al.18 (2005). However, a limiting factor as far as minimal dental intervention is concerned, is the overall difficulty of acceptance by dentists. Rios et al.31 (2006) evaluated professionals from the public service in Goiânia and found that less than half of the professionals (42.8%) believed in the efficacy of the technique, and that more information would be required about the technique, its efficiency and its use in public service.
In spite of the difficulties encountered, mainly in following up the restorations, ART continues to provide an important scope for covering schoolchildren as well as the community in general, taking into account the shorter time for performing restorations and its low cost5. In this context, Mickenautsch et al.32 (2002) reported that the introduction of ART into a mobile dental assistance program led to a significant reduction in the percentages of amalgam restorations and extractions.
According to the results of the present study, ART appeared as a feasible alternative for caries treatment, particularly in collective health, with proven efficacy, low cost and broad improvement in covering dental care to schoolchildren. These factors may be observed by the technique simplicity and speed of the procedures and contribution to the problem of the huge repressed demand by patients with treatment needs. It could therefore be concluded from this six-month evaluation that ART was effective within health promotion programs as an important measure to control caries disease in schoolchildren.
Acknowledgements
The authors thank the "Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – CAPES" for granting scholarships and for constantly supporting research in Graduation programs at the Piracicaba School of Dentistry (FOP/Unicamp).
References
1. Brazil. Ministry of Health. Secretary of Health Care. Department of Primary Care. Project "SB Brasil" 2003. Oral health status of the Brazilian population 2002-2003: principal results. Brasília: Ministry of Health, 2004. [ Links ]
2. Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic restorative treatment (ART): rationale, technique and development. J Public Health Dent 1996; 56:135-40. [ Links ]
3. Roshan NM, Anand LS, Deshpande SD. Microbiological evaluation of salivary Streptococcus mutans from children of age 5-7 years, pre- and post-atraumatic restorative treatment. Contemporary Clinical Dentistry 2010; 1(2): 94-7. [ Links ]
4. Almeida Neves A, Cutinho E, Cardoso MV, Lembrechts P, Van Meerbeek B. Current concepts and techniques for caries excavation and adhesion to residual dentin. J Adhes Dent 2011 Feb; 13(1): 7-22. [ Links ]
5. Frencken JE. The ART approach using glass ionomers in relation to global oral health care. Dental Materials, 2010, 26: 1-6. [ Links ] 6. Menezes JPL, Rosenblatt A, Medeiros E. Clinical evaluation of atraumatic restorations in primary molars: A Comparison Between 2 glass ionomer cements. Journal of Dentistry for Children 2006; 73:2: 91-7. [ Links ]
7. Silva RC, Zuanon ACC, Spolidorio DMP, Campos JADB. Antibacterial activity of four ionomer cements used in atraumatic restorative treatment. J Mater Sci: Mater Med, 2007; 18: 1859-1862. [ Links ]
8. Taifour D, Francken JE, Beiruti N, van´t Hof MA, Truin GJ. Effectiveness of glass ionomer (ART) and amalgam restorations in the deciduous dentition: results after 3 years. Caries Res 2002;36:437–444.
9. Frencken JE, van't Hof MA, Taifour D, Al-Zaher I. Effectiveness of ART and traditional amalgam approach in restoring single-surface cavities in posterior teeth of permanent dentitions in school children after 6.3 years. Community Dent Oral Epidemiol 2007; 35: 207–214.
10. Yu C, Gao XJ, Deng DM et al. Survival of glass ionomer restorations placed in primary molars using atraumatic restorative treatment (ART) and conventional cavity preparations: 2- year results. Int Dent J 2004; 54:42-46. [ Links ]
11. Frencken JE, Makoni F, Sithole WD. ART restorations and glass ionomer sealants in Zimbabwe: survival after 3 years. Community Dent Oral Epidemiol 1998; 26: 372-81. [ Links ]
12. Holmgren CJ, Lo ECM, Hu DY, Wan HC: ART restorations and sealants placed in Chinese school children – results after three years. Community Dent Oral Epidemiol 2000; 28: 314–20
13. van Gemert-Schriks MCM, van Amerongen WE, ten Cate JM, Aartman IHA. Three-year survival of single- and two-surface ART restorations in a high-caries child population. Clin Oral Invest 2007; 11:337–343.
14. Couto GBL, Vasconcelos MMVB, Melo MMC, Camelo CAC, Valença PAM. Prevalence of caries, white spot and visible plaque in children 0-36 months, assisted by the Family Health Program in the City of Camaragibe - PE. Odontol Clín-Cient 2005; 4:19-28. [ Links ]
15. Sant´anna, G.R.; Bonecker, M.J.S.; Diarte, D.A.; Suga, S.N. Book of Pediatric Dentistry; Sonetos Ed. 2002 apud Martins, A.A., Santos, A.A.; Barreto, M.A.C.; Oliveira, C.C.C. Table of risk factors for decay applicable in public health.Odontologic . Clín. Científ., Recife, 2003; 2(1): 37-42, Jan/Abr. [ Links ]
16. Ministry of health. SS-95 resolution, 27/06/2000. Recommendations about the use of fluoride products in the "SUS" / SP according to the risk of dental caries. [on line] Available in URL: http://www.saude.sp.gov.br/fr_sbucal.html. [ Links ]
17. Schriks MCM, van Amerongen WE. Atraumatic perspective of ART: psychological and physiological aspects of treatment with and without rotary instruments. Community Dent Oral Epidemiol 2003; 31: 15–20.
18. Pellegrinetti MB, Imparato JCP, Bressan MC, Pinheiro SL, Echeverria S. Evaluation of the glass ionomer cement retention in cavities restored by atypical atraumatic restorative technique. Pesq Bras Odontoped Clin Integr 2005; 5(3): 209-13. [ Links ]
19. IBGE. Brazilian Institute of Geography and Statistics. Data de Piracicaba. Available in: http://www.ibge.gov.br. [ Links ]
20. São Paulo (State). Ministry of Economy and Planning. Foundation State System of Data Analysis. Municipality of Piracicaba Profile [cited in 2011 Nov, 21]. Available em: http://www.seade.sp.gov.br/produtos/perfil/perfil.php. [ Links ]
21. Basting RT, Pereira AC, Meneghim MC. Evaluation of the dental caries prevalence in schoolchildren from Piracicaba SP, Brasil, after 25 years of fluoridation of public water supply. Rev Odontol Univ São Paulo 1997; 11(4):287-92. [ Links ]
22. Cortellazzi, KL, Tagliaferro EPS, Assaf AV, Ambrosano GMB, Bittar TO, Meneghim MC, Pereira AC. Influence of socioeconomic, demographic and clinical experience of dental caries in preschool children in Piracicaba, SP. Rev Bras Epidemil 2009; 12 (3): 490-500. [ Links ]
23. Guerra LM, Pereira AC, Pereira SM, Meneghim MC. Assessment of socioeconomic variables in the caries and fluorosis prevalence in cities with and without water supply fluoridation. Rev Odontol UNESP. 2010; 39(5): 255-262. [ Links ]
24. Word Health Organization. Oral health surveys, basics methods. Geneva: Word Health Organization; 1997. [ Links ]
25. Sacramento PA, Borges AFS, Puppin Rontani RM. Actuarial analysis in a comparative study of two glass ionomer cements used in the technique of ART: direct and indirect assessment after 3 and 6 months. Tev odontol UNESP 2009; 38(5):291-300. [ Links ]
26. Lima DC, Saliba NA, Moimaz SAS. Atraumatic restorative treatment and it aplication in public health. RGO 2008; 56:71-9. [ Links ]
27. Navarro MFL, Modena KCS, Freitas MCCA, Fagundes TC. Transfering ART research into education in Brazil. J Appl Oral Sci. 2009; 17(sp issue): 99-106. [ Links ]
28. Smales RJ, Yip HK. The atraumatic restorative treatment (ART) approach for primary teeth; review of literature. Pediatric Dentistry 2000; 22(4):294-8. [ Links ]
29. Figueiredo CH, Lima FA, Moura KS. Atraumatic Restorative Treatment: assessment of their suitability as a strategy for controlling dental caries in public health. RBPS 2003; 17(3);109-18. [ Links ]
30. Bresciani E. Clinical trials with atraumatic restorative treatment (ART) in deciduous and permanent teeth. J Appl Oral Sci 2006; 14: 14-9. [ Links ]
31. Rios LE, Essado REP, Freire MCM. Tratamento restaurador atraumático: knowledge and attitudes of dentists in the public service of Goiânia-GO. Rev Odontol UNESP 2006; 35(1): 75-80. [ Links ]
32. Mickenautsch S, Munshi I, Grossman ES. Comparative cost of ART and conventional treatment within a dental school clinic. SADJ. 2002; 57(2): 52-8. [ Links ]
 Correspondence:
Correspondence:
Maria da Luz Rosário Sousa
Faculdade de Odontologia de Piracicaba
Avenida Limeira 901, Bairro Areão.
CEP 13414-903, Piracicaba, SP, Brazil
E-mail: luzsousa@fop.unicamp.br
Received for publication: July 12, 2011
Accepted: January 03, 2012
