










 Inglés
Inglés




 Permalink
PermalinkBrazilian Journal of Oral Sciences
ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.1 Piracicaba ene./mar. 2012
ORIGINAL ARTICLE
Influence of viscosity and polymerization mode on bond strength of dual-cure resin luting agent to dentin
Marina Di FrancescantonioI; Thaiane Rodrigues AguiarI; Marcelo Tavares de OliveiraII; Marcelo GianninIII
IDDS, MS, PhD student, Department of Restorative Dentistry, Piracicaba School of Dentistry, Campinas State University, Piracicaba, SP, Brazil
IIDDS, MS, PhD, Assistant Professor, Department of Operative Dentistry, University Nove de Julho, São Paulo, SP, Brazil
IIIDDS, MS, PhD, Associate Professor, Department of Restorative Dentistry, Piracicaba School of Dentistry, Campinas State University, Piracicaba, SP, Brazil
ABSTRACT
AIM: To evaluate the influence of the viscosity and curing mode on the bond strength of two resin cements to dentin.
METHODS: Eight experimental groups were formed (n = 7) according to the dual-cure resin cements (Nexus 2 - Kerr Corp. and Variolink II - Ivoclar Vivadent), curing modes (dual-cure or self-cure) and viscosities (low and high). Resin cements were applied to pre-cured composite resin discs (2 mm thick, Sinfony -3M ESPE), which were fixed to bonded dentin surfaces. The restored teeth were either light-activated (XL3000 - 3M ESPE) or allowed to self curing only. After 24 h, the teeth were both mesiodistally and buccolingually sectioned to obtain bonded beam specimens (0.8 mm2 cross-sectional area). Each specimen was tested in microtensile strength at a crosshead speed of 0.5 mm/min until failure.
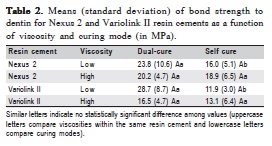
RESULTS: Data (in MPa) were analyzed statistically by three-way ANOVA and Tukey’s post-hoc test (pre-set á = 0.05). No significant difference was observed between resin cements (p=0.26) and viscosities (p=0.13), however, the curing mode affected the BS within the viscosities (p=0.01). Statistically significant difference was observed for low viscosity: Nexus 2: 23.8(10.6) (dual-cure) and 16.0(5.1) (self-cure); Variolink II: 28.7(8.7) (dual-cure) and 11.9(3.0) (self-cure).
CONCLUSIONS: Light activation yielded higher bond strength for the low-viscosity versions of the resin cements.
Keywords: dentin bonding agents, resin cement, bond strength, dentin.
Introduction
The adhesive cementation techniques for indirect metal-free restorations use dual-cure resin luting agent, and the clinical success of these restorations depends on the quality of the restorative material and its bonding to the mineralized dental tissues, among other factors. The luting agents are a combination of dual-cure resin cement and a bonding agent, which is responsible by the adhesion between the tooth and the resin cement1-5.
Resin cements can be dual-cure, only self-cure or only light-cure materials. Dual-cure resin cements are indicated in clinical situations when no light is available to polymerize the material and the self-curing component should compensate for the absence of light. In other situations, there is a loss of light because of either the distance between the light-curing tip and the luting agent or light attenuation through the thickness of the indirect restoration6-10.
The resin cements present different viscosities, which can produce cementlayers with different thicknesses. These differences on thickness may affect some properties of the material, such as strength, modulus of elasticity and rheology, which can interfere in restoration longevity. Resin cements provide a correct seating of the indirect restoration and are also responsible for the tooth-restoration interfacial sealing, which prevents the marginal leakage11-14. Viscosity variation for resin cements is obtained by modifying the proportion between monomer composition and filler particle content15. Nothing is known about the viscosities of resin cements and their influence when used with different polymerization modes (dual-cure or self-cure) on bond strength to dentin. Thus, the purpose of this study was to measure the bond strength of prepolymerized composite discs to underlying tooth structure using dual-cure resin luting agents with two viscosities (high and low), which either were allowed to self curing in the absence of light or were exposed to light through the composite disc. In addition, the failure site morphology was analyzed and compared by material types and polymerization modes. The research hypothesis tested was that bond strength values would be significantly higher when the resin cement was subjected to light-activation (dual cure) than when they were only allowed to self curing. It was also hypothesized that the bond strength of low-viscosity dual-cure resin cement would be significantly lower than that of high-viscosity resin cement.
Material and methods
Specimen Preparation and Experimental Groups
The research protocol was approved by the Ethics Committee of the School of Dentistry of Piracicaba, University of Campinas, SP, Brazil (176/2006). Fifty-six freshly extracted, erupted, human third molars were used. The teeth were stored in a saturated thymol solution at 5 °C for no longer than 3 months16. They were then sectioned transversally in the middle third of the crown, using a diamond blade saw (Series 15HC Diamond, Buehler Ltd, Lake Bluff, IL, USA) on an automated sectioning device (Isomet 2000, Buehler Ltd) under water cooling, exposing areas of midcrown dentin.
The exposed dentin surfaces were wet polished (APL-4, Arotec, Cotia, SP, Brazil) using 600-grit SiC paper in order to create a flat surface with standardized smear layer before application of the bonding agents. The prepared teeth were then randomly divided into 8 groups (n = 7).
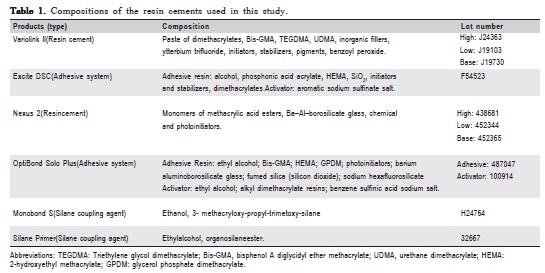
Two dual-cure resin cements that present commercial versions in high and low viscosity, Nexus 2 (Kerr Corp., Orange, CA, USA) and Variolink II (Ivoclar Vivadent, Schaan, Liechtenstein), and their respective adhesive systems and silane primers (OptiBond Solo Plus and Silane Primer - Kerr Corp.; Excite DSC and Monobond S - Ivoclar Vivadent) were used (Table 1). Fifty-six pre-polymerized, light-cure composite resin discs, 2 mm thick and 10 mm in diameter (B2D shade, Sinfony, 3M ESPE, St. Paul, MN, USA), were prepared to simulate overlying laboratory-processed composite resin restorations. The surface of each disc was sandblasted with 50 μm aluminum oxide (Danville Engineering Inc, San Ramon, CA, USA) for 10 s (air pressure = 0.552 MPa; distance from the tip = 1.5 cm) and silanated with coupling agents according to manufacturers’ instructions (Monobond-S or Silane Primer).
The adhesive systems and the resin cements were applied and used according to manufacturers’ instructions. The resin cements were mixed previously in the proportion of 1:1 (catalyst and base paste) and were applied to the sandblasted surface of the pre-polymerized composite resin disc, which was placed on the dentin surface. The resin cements were light-cured for 40 s (XL 3000; 3M ESPE) through the composite resin disc or were allowed to self curing only with a load of 0.5 kg applied horizontally for 5 min. In order to facilitate specimen gripping during bond testing, a 3-mmthick block of self-cure composite resin (Concise, 3M of Brazil, Sumaré, SP, Brazil) was added to the untreated, prepolymerized composite resin surface.
Microtensile bond strength
Restored teeth were stored in distilled and deionized water at 37° C for 24 h and were then vertically serially sectioned into several 1.0-mm-thick slabs. Each slab was further sectioned perpendicularly to produce bonded beam specimens with 0,8mm2 in cross-section. Each bonded beam was attached to the grips of a microtensile testing device with cyanoacrylate glue (Super Bonder; Henkel/Loctite, Diadema, SP, Brazil) and tensioned in an universal testing machine (4411; Instron Co., Canton, MA, USA) at a crosshead speed of 0.5 mm/min until failure. After testing, the specimens were carefully removed and the cross-sectional area at the site of fracture was measured to the nearest 0.01 mm with a digital caliper (mod. 727-6/150, Starret Ind. e Com. Ltda., Itu, SP, Brazil). The specimen cross-sectional area was divided by the peak tensile load at failure to calculate stress at fracture (in MPa). A single failure stress value was then calculated for each tooth by averaging the values of 5 tested beams from that tooth.
A three-way ANOVA (two resin cements, two polymerization modes and two viscosities) was performed to determine the effect of these major factors on tensile strength. Tukey’s post-hoc test was used to detect pair-wise differences among the experimental groups. All statistical testing was performed at a preset α of 0.05.
Failure pattern analysis
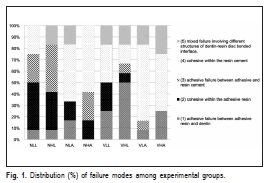
TFractured surfaces of tested specimens were sputter coated with gold (MED 010, Balzers, Balzer, Liechtenstein) and examined by a single individual using a scanning electron microscope (VP 435, Leo, Cambridge, England). Failure patterns were classified as: (1) adhesive failure between adhesive resin and dentin; (2) cohesive within the adhesive resin, (3) adhesive failure between adhesive and resin cement (4) cohesive within the resin cement, (5) mixed failure involving different structures of dentin-resin disc bonded interface. Representative areas of the failure patterns were photographed (85× to 1,900×).
Results
Summary statistics for the different experimental groups are shown in Table 2. Three-way ANOVA indicated that the curing mode factor significantly influenced tensile strength results (p = 0.0005). The statistical analysis revealed difference only for curing mode (p= 0.0004), no significant differences for the triple interaction (resin cement × curing mode × viscosity, p = 0.4303) or for interaction between cement × viscosity (p = 0.1710) and cement × curingmode (p = 0.1312). The analysis only indicated an interaction between the viscosity x curing mode (p = 0.0127).
When looking at data with respect to differences in curing mode, the bond strength of the low viscosity version of the resin cements was affected by curing mode (p< 0.05), while light-activation did not increase the bond strength of high viscosity versions (p> 0.05). The type of resin cement and the viscosity did not affect the bond strength (p> 0.05).
Figure 1 shows the proportional prevalence (%) of the failure patterns in all experimental groups, and representative images depicting failure modes are presented in Figures 2 and 3. Adhesive failures along the dentin surface were observed for all groups, except for Nexus 2 in low-viscosity and self cure mode. For Variolink II in high viscosity and dual-cure mode, half of the specimens had adhesive failures (type 1) (Figures 2A and 2B). High- or low-viscosity dualcure Nexus 2 exhibited high incidence of cohesive failures within the adhesive resin and adhesive failures between adhesive and resin cement (Figures 3A and 3B, respectively). Except for high-viscosity dual-cure Nexus 2, cohesive failures within the resin cement was observed for all groups; however, it occurred mainly for self-cure groups (Figure 3C). Mixed failures involved two or more types of failures (adhesive and cohesive failures) in the same fractured end of specimens and all groups with Variolink II showed mixed failures (Figures 2C, 2D, and 2E).


Discussion
A more effective bonding to dentin can increase the strength of remaining dental structures and reduce microleakage between the tooth and restoration, which are important to tooth longevity17,18. For supporting use of these materials, we tested the research hypothesis that bond strength values would be significantly higher when the resin cements were light-activated, which was confirmed only for lowviscosity versions. The hypotheses that the bond strength of resin cements in low-viscosity versions would be significantly lower than those in high-viscosity cements was rejected, since no statistical difference was noted between low- and highviscosity materials. The low and high versions of resin cements are indicated for different purposes15,19, but the compositions that form both viscosities did not influence the bond strength. Since the resin cements reach high monomer conversion after light curing, only the low-viscosity resin cements were able to produce higher bond strength.
The high-viscosity version of both resin cements showed no significant difference on bond strength irrespectively of being light activated or not, since the increased amount of fillers improves the mechanical properties of the cement. The bond between the monomer components and filler particles by treatment of these particles, such as silanization, and the higher amount of fillers promote the increase of the cohesive strength of the resin cement19. However, the low-viscosity formulation of the resin cements did not maintain the bond strength mean value when the materials were allowed to self curing only. Light activation of low-viscosity resin cements produced higher bond strength to dentin than self curing alone20. Cohesive failures within the resin cement occurred predominantly in those specimens in which the resin cements were allowed to self curing only (Figure 1).
Since the self curing reaction alone does not reach the monomer conversion promoted by light6,10, the resin cement layer may be the weak point at the resin-dentin interface. Thus, in the present in vitro study, when the resin-dentin interface was under tension, the resin cement layer tended to fracture more easily than other parts of this interface. Depending on the resin cement and its viscosity, light-curing caused different types of failure (Figures 1 to 3). For the selfcure resin cements, the predominant failure pattern was the cohesive failure in resin cement, indicating that the lack of light activation reduced the cohesive strength of the cement (Figures 2C, 2D, 2E and 3C). The dual-cure resin cements presented different failure patterns, depending on the type of adhesive systems used (Figures 2A, 2B, 3A and 3B).
The luting agents tested in this study showed no significant difference when compared by different viscosities and curing modes. These materials showed the same results in terms of bond strength to dentin, corroborating the findings of Hikita et al.21 (2007). Other studies showed that Variolink II presented higher bond strength than Nexus 2, but they did not report viscosity of these resin cements used4,22. Regarding the curing mode, few resin cement systems (Nexus 2, Kerr Co.; Variolink II, Ivoclar Vivadent; Panavia F, Kuraray; RelyXARC and RelyX Unicem, 3M ESPE) seem able to produce proper degree of conversion and high bond strength to dentin6,13-15,17.
The bonding agents (OptiBond Solo Plus and Excite DSC) used with resin cements are etch-and-rinse, two-step systems. They are simplified single-bottle adhesive systems that present a low pH value and might jeopardize resin cement conversion reducing the bond strength, if only autopolimerized23. As adhesive systems are spread into a thin layer, an incompletely polymerized resin monomer layer is formed on the adhesive surface. The oxygen inhibition layer formed by uncured acidic simplified etch-and-rinse systems impairs the adhesion between bonding agents and chemical-, light- or dual-cured resin-based restorative materials. The adverse reaction involves the uncured acidic adhesive layer and the tertiary amine catalytic component of the resin cement23,24.
Both adhesives contain an aromatic sodium sulfinate salt as a co-initiator to develop dual-cure reaction. Excite DSC uses the co-initiator impregnated in the microbrush tip as a white salt powder, while OptiBond Solo Plus has an activator bottle that contains the benzene sulfinic acid sodium salt in an alcoholic solution4,20. In this study, the addition of these co-initiators to the bonding agents contributed to preserve the bond strength of the high-viscosity cements without light exposure (self curing), since the adhesive was not polymerized and the co-initiator could mix with cement, increasing the polymerization of cement. The same, however, did not occur with the low-viscosity version because the mixture of liquid solutions from the adhesive and activator with a hydrophobic flowable resin cement material may be poor and a larger amount of monomers requires a higher formation of free radicals for an efficient polymerization17. These mixtures involve an aqueous solution containing sodium sulfinate salt and a hydrophobic material, which resulted in lesser polymerization and lower bond strength for the self-cure cements.
It may be concluded that light activation yielded higher bond strength for the low-viscosity versions of the resin cements.
Acknowledgements
This study was supported by grants 06/57998-0 from FAPESP and CAPES, Brazil. The authors are indebted to the Dental Materials Division (FOP-UNICAMP) for providing use of the universal testing machine.
References
1. Arrais CA, Giannini M, Rueggeberg FA, Pashley DH. Microtensile bond strength of dual-polymerizing cementing systems to dentin using different polymerizing modes. J Prosthet Dent. 2007;97:99-106. [ Links ]
2. Inokoshi S, Willems G, Van Meerbeek B, Lambrechts P, Braem M, Vanherle G. Dual-cure luting composites: Part I: ûller particle distribution. J Oral Rehabil. 1993;20:133-46. [ Links ]
3. Milleding P, Ortengren V, Karlsson S. Ceramic Inlay Systems: Some Clinical Aspects. J Oral Rehabil. 1995;22:571-80. [ Links ]
4. Piwowarczyk A, Bender R, Ottl P, Lauer HC. Long-term bond between dual-polymerizing cementing agents and human hard dental tissue. Dent Mater. 2007;23:211-7. [ Links ]
5. Sjogren G, Molin M, van Dijken J, Bergman M. Ceramic inlays (Cerec) cemented with either a dual-cured or a chemically cured composite resin luting agent. A 2-year clinical study. Acta Odontol Scand. 1995;53:325-30. [ Links ]
6. Arrais CA, Rueggeberg FA, Waller JL, de Goes MF, Giannini M. Effect of curing mode on the polymerization characteristics of dual-cured resin cement systems. J Dent. 2008;36:418-26. [ Links ]
7. Dagostin A, Ferrari M. In vivo bonding mechanism of an experimental dual-curing enamel-dentin bonding system. Am J Dent. 2001;14:105-8. [ Links ]
8. Foxton RM, Nakajima M, Tagami J, Miura H. Bonding of photo and dual cure adhesives to root canal dentin. Oper Dent. 2003;28:543-51. [ Links ]
9. Rasetto FH, Driscoll CF, Prestipino V, Masri R, von Fraunhofer JA. Light transmission through all-ceramic dental materials: a pilot study. J Prosthet Dent. 2004;91:441-6. [ Links ]
10. Rueggeberg FA, Caughman WF. The influence of light exposure on polymerization of dual-cure resin cements. Oper Dent. 1993;18:48-55. [ Links ]
11. Díaz-Arnold AM, Vargas MA, Haselton DR. Current status of luting agents for fixed prosthodontics. J Prosthet Dent. 1999;81:135-41. [ Links ]
12. Wilson PR. Low force cementation. J Dent. 1996;24:269-73. [ Links ]
13. De la Macorra JC, Pradíes G. Conventional and adhesive luting cements. Clin Oral Investig. 2002;6:198-204. [ Links ]
14. Osman SA, McCabe JF, Walls AW. Film thickness and rheological properties of luting agents for crown cementation. Eur J Prosthodont Restor Dent. 2006;14:23-7. [ Links ]
15. Neves AD, Discacciati JA, Orêfice RL, Jansen WC. Correlation between degree of conversion, microhardness and inorganic content in composites. Pesqui Odontol Bras. 2002;16:349-54. [ Links ]
16. Humel MMC, Oliveira MT, Cavalli V, Giannini M. Effect of storage and disinfection methods of extracted bovine teeth on bond strength to dentin. Braz J Oral Sci. 2007;22:1402-6. [ Links ]
17. Kumbuloglu O, Lassila LV, User A, Vallittu PK. A study of the physical and chemical properties of fourresin composite luting cements. Int J Prosthodont. 2004;17:357-63. [ Links ]
18. Soares CJ, Giannini M, Oliveira MT, Paulillo LAMS, Martins LRM. Effect of surface treatments of laboratory-fabricated composites on the microtensile bond strength to a luting resin cement. J Appl Oral Sci. 2004;12:45-50. [ Links ]
19. Hahn P, Attin T, Gröfke M, Hellwing E. Influence of resin cement viscosity on microleakage of ceramic inlays. Dent Mater. 2001;17:191-6. [ Links ]
20. Arrais CA, Giannini M, Rueggeberg FA, Pashley DH. Effect of curing mode on microtensile bond strength to dentin of two dual-cured adhesive systems in combination with resin luting cements for indirect restorations. Oper Dent. 2007;32:37-44. [ Links ]
21. Hikita K, Van Meerbeek B, De Munck J, Ikeda T, Van Landuyt K, Maida T et al. Bonding effectiveness of adhesive luting agents to enamel and dentin. Dent Mater. 2007;23:71-80. [ Links ]
22. Pekkan G, Hekimoglu C. Evaluation of shear and tensile bond strength between dentin and ceramics using dual-polymerizing resin cements. J Prosthet Dent. 2009;102:242-52. [ Links ]
23. Sanares AME, Itthagarun A, King NM, Tay FR, Pashley DH. Adverse surface interactions between one-bottle light-cured adhesives and chemicalcured composites. Dent Mater. 2001;17:542-56. [ Links ]
24. Giannini M, de Goes MF, Nikaido T, Shimada Y, Tagami J. Influence of activation mode of dual-cured resin composite cores and low-viscosity composite liners on bond strength to dentin treated with self-etching adhesives. J Adhes Dent. 2004;6:301-6. [ Links ]
 Correspondence:
Correspondence:
Marcelo Giannini
Department of Restorative Dentistry,
Operative Dentistry Section
Piracicaba School of Dentistry -
State University of Campinas
Av. Limeira, 901, Piracicaba, SP, Brasi
E-mail: giannini@fop.unicamp.br
Received for publication: December 06, 2011
Accepted: March 21, 2012
