










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.2 Piracicaba Abr./Jun. 2012
ORIGINAL ARTICLE
Measurements of the mandibular canal by multidetector computed tomography
Frederico Sampaio NevesI; Daniel Fernandes TourinhoII; Manoela CarreraIII; Iêda Crusoé-RebelloIV; Thereza BittencourtV; Miguel SetúbalII
IDepartment of Oral Diagnosis, Piracicaba Dental School, State University of Campinas, Piracicaba, SP, Brazil
IIDepartment of Oral and Maxillofacial Surgery, School of Dentistry, Bahiana Foundation for the Development of Sciences, Salvador, BA, Brazil
IIIDepartment of Oral Pathology, Piracicaba Dental School, State University of Campinas, Piracicaba, SP, Brazil
IVDepartment of Oral Radiology, School of Dentistry, Federal University of Bahia, Salvador, BA, Brazil
VDepartment of Animal Development, Veterinary School, Federal University of Bahia, Salvador, BA, Brazil
ABSTRACT
AIM: The aim of this study was to investigate the measurements of the mandibular canal in different patterns of reabsorbed alveolar ridges, using multidetector computed tomography in order to evaluate the relationship of the mandibular canal with the cortex of the mandible remains.
METHODS: Central cross-sectional slice of 30 edentulous alveolar ridges in the mandibular first molar region of otherwise healthy patients using multidetector computed tomography were analyzed. Horizontal and vertical lines were performed tangent to the corticals of the mandible and mandibular canal. Fisher's exact test, Spearman test and linear regression were used for statistical analysis. Significance level for all statistical tests was 95%.
RESULTS: The height of the mandible and the distance of mandibular canal to superior cortical in males were significantly higher when compared with females (p<0.05). When the height of the mandibular bone was correlated to the classification of edentulous jaws, significant differences were observed when comparing the three types (III, IV and V) as well as between III and IV type.
CONCLUSIONS: The results of the present study show that the measurements for dental implant placement in the posterior region of the mandible are affected by the different patterns of bone resorptions. It was also demonstrated the importance of the computed tomography in the process of planning dental implant placements.
Keywords: bone, mandibular canal, computed tomography, mandible, measurements.
Introduction
For preoperative planning of mandibular implant placement, precise evaluation of bone size and morphology is important. The size of the selected implant depends on the height and width of available bone and the location of the mandibular canal1. Physiological absorption of the edentulous alveolar ridge will reduce the distance between the bone crest and the cortical of the mandibular canal. The measures obtained in panoramic and periapical radiographs do not accurately correspond to the reality. The mandibular canal could be lateralized and not necessarily in the center of the mandible body, requiring a specific preoperative radiologic examination for better management of the case1-2.
Placement of endosseous implant in the appropriate position to allow creation of an aesthetic prosthesis depends on bone volume, height and density. Bonedensity and height can both be estimated by radiographic evaluation, using conventional tomography and periapical or panoramic radiographs2. Computed tomography (CT) scan by image reconstruction has been used to investigate periapical injuries and its relation to the mandibular canal3 and due to its property to trustily reconstruct bone anatomy, represents an excellent adjunct to the evaluation of the actual position of the mandibular canal within the mandible4.
Multidetector CT (MDCT) is considered one of the most valuable imaging modalities for preoperative procedures because it allows the acquisition of fast, reliable and reproducible images. Each anatomical structure can be viewed in the three orthogonal planes (axial, coronal, sagittal), overlapping of surrounding anatomical structures can be eliminated and a three-dimensional reconstruction of the evaluated structure can be done. In comparison with cone beam computed tomography, the greatest advantage of MDCT is the optimal contrast resolution, allowing differentiation between hard and soft tissues5. CT was considered a highdose technique for a long time, but with the development of MDCT and low-dose protocols tailored for diagnosis, doses below 0.15 mSv are achievable6.
It is important to measure bone volume to avoid injuries in the alveolar inferior nerve resulting from implant surgery. The trajectory of the mandibular canal at the site of implant placement may alter sensation of the lower lip due to inferior alveolar nerve injury and it is one of the most serious complications of mandibular implant surgery7-8.
The aim of this study was to investigate the measurements of the mandibular canal in different patterns of resorbed alveolar ridges, using MDCT in order to evaluate the relationship of the mandibular canal with the cortex of the mandible remains.
Material and methods
Data were collected from the data bank of a radiology center. All patients enrolled at this evaluation were conducting MDCT examination as a procedure of their treatment planning for rehabilitation with titanium implants. Therefore, no radiation was imposed to the patient to obtain the study data. All patients gave written informed consent for the examination and use of data for the research protocols.
A retrospective study was conducted from more central cross-sectional slice of 30 edentulous alveolar ridges in the mandibular first molar region of otherwise healthy patients using MDCT. The mandibles were evaluated using noncontrasted exams performed in high resolution helical CT device (CT Synergy Helicoidal; General Eletric Company, Milwaukee, WI), The examination was performed with the patient in supine position (slice thickness 0.625 mm and increment of 0.625 mm, field of view of 15.8cm, bone filter, 120 kV and 200 mA). Each coronal slice was analyzed on the CT workstation monitor (Advantage Workstation 3.1 Ultra 10sm GE Medical Systems, USA), under dim lighting conditions, by one oral and maxillofacial radiologist with more than 10 years experience in CT.
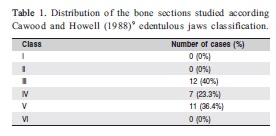
All MDCT images of the bone sections were categorized according the criteria of Cawood and Howell (1988)9 edentulous jaws classification: I - dentate, II - immediately post extraction, III - well-rounded ridge form, adequate in height and width, IV - knife-edge ridge form, adequate in height and inadequate in width, V - flat ridge form, inadequate in height and width and VI - depressed ridge form, with some basilar loss evident.
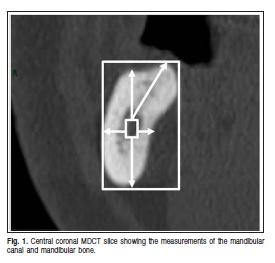
Horizontal and vertical lines were performed tangent to the cortical plates of the mandible and mandibular canal. The outcome variables were the linear distances (cm) between mandible width and height, mandibular canal width and height, distance of the mandibular canal to buccal, lingual, superior and inferior cortical plates of the mandible and the distance of the mandibular canal to the higher point of the alveolar ridge (Figure 1). Images were re-evaluated after a four-month interval and intraobserver agreement was calculated, demonstrating high reproducibility (Kappa index
= 0.95).
Data were analyzed using the SAS 9.1 software (SAS Institute, Cary, NC, USA). Descriptive parameters were given as mean and standard deviation (SD). Significant differences between comparable measurements were tested for gender and classes of the edentulous jaws with Fisher's exact test. Spearman test was used to evaluate the correlation between variables with biological plausibility. Linear regression was used to determinate the best fit between the variables. Significance level for all statistical tests was set at 95%.
Results
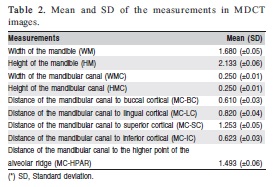
Table 1 shows the classification of the edentulous jaws according to Cawood and Howell (1988)9. The most prevalent classes were III, IV and V. The mean and standard deviation (SD) of the measurements are summarized in the Table 2.
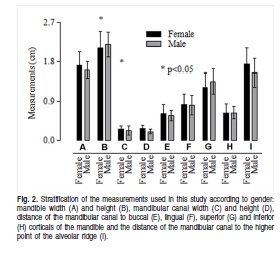
The differences between males and females regarding mandible width and height, mandibular canal width and height, distance of the mandibular canal to buccal, lingual, superior and inferior cortical plates of the mandible and the distance of the mandibular canal to the higher point of the alveolar ridge are presented in Figure 2. The height of the mandible in males was significantly higher when compared to females (p<0.05). However, the mandibular canal width in females was significantly higher when compared to males (p<0.05). The width of the mandible and the distance of the mandibular canal to the higher point of the alveolar ridge were higher in females, but not statistically significant.
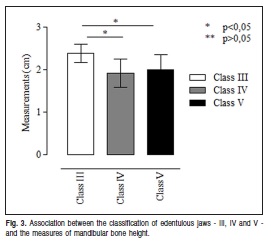
When the height of the mandibular bone was correlated to the classification of edentulous jaws, there were significant differences when comparing the three types (III, IV and V) as well as between III and IV types. There was no significant difference between types IV and V's edges height. Type III mandibular bone height had a higher value (mean = 2.383 cm), followed in a descending order by type V (mean = 2.0 cm) and type IV (mean = 1.914 cm) (Figure 3).
Comparing the three types (III, IV and V) with all measurements performed in this study, statistically significant differences were found in the mandibular bone height and the distance of the mandibular canal to the superior cortical (alveolar ridge). The other measurements and types of edentulous jaws showed no statistical differences (Figure 4). 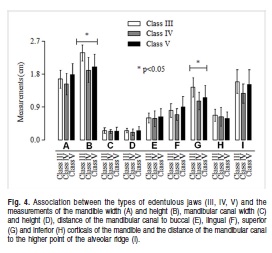
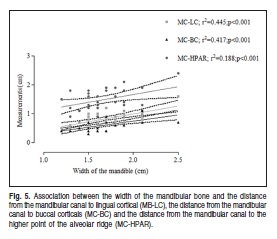
It was found that the greater the horizontal diameter of the mandibular bone, the greater the vestibular (r2=0.646; p<0.05) and lingual (r2=0.675; p<0.05) width. Linear regression analysis also demonstrated that there was a linear interaction between the horizontal diameter and vestibular width (r2=0.417) and lingual ridge width (r2=0.455). Although positive correlation was observed between the mandibular bone horizontal diameter and the distance to the highest point of the ridge (r2=0.188), the interaction between these two variables was weaker (Figure 5).
A positive correlation could be noticed between the increased vertical distance and the increment of the superior (r2=0.821; p<0.05) and inferior heights (r2=0.423; p<0.05), as well as the distance of highest point of the alveolar ridge (r2=0.634; p<0.05). Linear regression between the vertical diameter and the distance to the highest point of the alveolar ridge (r2=0.402) and the superior height (r2=0.673) showed a strong positive association (Figure 6).

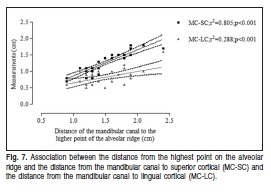
The distance of the highest point on the alveolar ridge is directly correlated with the superior height (r2=0.897; p<0.05) and the lingual weight (r2=0.537; p<0.05). A strong linear interaction was observed between the distance to the highest point of the alveolar ridge and the superior height (r2= 0.804), though, a weak positive association between the first and the last variable (r2=0.288) (Figure 7).
Discussion
An adequate dental treatment is based on comprehensive planning, which includes the use of imaging studies to assist on diagnosis. Imaging examinations have an important role to a successful treatment. The preoperative evaluation for implant therapy should consider the height and width of the bone, degree of corticalization, density of mineralization and amount of cancellous bone. Panoramic radiography is a the supplementary examination initially requested to implant surgery, however, because the two-dimensional image, this does not provide specific diagnostic information about the relationship of anatomical structures, thus, are necessarily a more accurate exam to a provide a higher operative safety2.
The mandibular canal is an anatomical structure used as reference to surgical approaches in the jaws. Extractions of third molars, implant placement, orthognathic surgery, reduction and fixation of fractures in various areas of the mandible are examples of procedures performed in close proximity to this canal, what increases the risk of injury to the inferior alveolar nerve10.
The use of CT for dental implant planning has been strongly advocated over the past decades2,11 due to its superiority to conventional radiographs12 and even when compared with conventional tomography. This can be attributed to three-dimensional visualization of the bone structures in CT scans13. Lindh (1995)14 compared the accuracy of measurements of two panoramic devices and three tomographic techniques. In all image modalities the distance between the superior border of the mandibular canal and the alveolar crest, the height of the mandibular canal and the distance between the mandibular base and the inferior border of the mandibular canal were measured. The values from the tomographic images deviated less from the panoramic images measurements. The observers underestimated the distances related to the mandibular canal, except for hypocycloidal tomography. The mean height of the mandibular canal was 3.0 mm, with a standard deviation of 0.7 mm. Height values of the mandibular canal were similar to those found in the present study.
It has been observed in dentate individuals, using CT, that the mean distance from the mandibular canal to the alveolar crest was 17.4 mm15. In similar and recent studies, Watanabe et al. (2010)16 and de Oliveira-Junior et al. (2010)17 measured the height of the mandible and distance of the mandibular canal to the superior cortical of the mandible in dentate and edentulous MDCT cross-sectional scans in a inferior first molar region. Comparing these studies with our findings, the distances were higher than in the present study, which is justified by the presence of teeth, not occurring the physiological bone resorption.
Paes et al. (2007)18 evaluated the accuracy of relative measurements from the roof of the mandibular canal to the alveolar crest in MDCT and single-slice CT. MDCT has a more accurate method and a higher reproducibility. It helps in the analysis of important anatomical landmarks for the planning of dental implants, namely the mandibular canal pathway and alveolar crest height.
According to the degree of bone resorption, significant changes may occur in relation to facial muscles and facial height, but the distance between the mandibular canal to mandibular cortex remains stable19. In the present research, performed in 30 mandibles, the distance of the mandibular canal to the inferior bone cortical diminished when the level of ridge resorption became more severe. In type III, the mean was 0.68 cm, followed by 0.62 cm in type IV and type V at 0.58 cm.
When anatomic structures and ridge resorption limit the placement of a standard implant, the clinician can use short implants or bone graft augmentation. In edentulous alveolar bone ridges less than 0.5 mm wide bone graft augmentation is required prior to implant placement. Crestal ridge bone augmentation is an alternative bone expansion technique that can be used to augment the atrophic maxilla and mandible prior to implant placement20. Short implants can also be placed to avoid the use of grafts, but it must always be taken into account when using these implants that a minimum bone height of 7-8 mm is needed anyway and that bone quality is a critical factor21.
Inferior alveolar nerve injury can result from traumatic local anesthetic injections, during dental implant site preparation or placement, or poor surgical technique. During implant surgery, damage to the inferior alveolar nerve can occur when the twist drill or implant encroaches, transects, or lacerates the nerve. The insertion of implants close to the canal can compromise the success of the surgery. The contact with the neurovascular bundle can actually cause the nonintegration of the implant or lead to sensory dysfunction. It is essential to obtain, especially in CT images, as much information as possible from the anatomic appearances and variations for a safer surgical procedure22.
MDCT provides an excellent visualization and delineation of mandibular anatomy, which, in turn, allows establishing the buccolingual position and height of neurovascular bundle, as well as, evaluating the amount of bone available for correct placement of implant fixtures.
The results of the present study showed that the measurements for dental implant placement in the posterior region of the mandible are affected by the different patterns of bone resorption. Therefore, the surgeon and radiologist should be aware of the correct bone measurements in the preoperative planning for dental implant placement, being CT extremely important in this process to avoid intra- or postoperative complaints.
Acknowledgements
We are grateful to Delfin Clinic for the support in this study.
References
1. Garg AK, Morales MJ, Navarro I, Duarte F. Autogenous mandibular bone grafts in the treatment of the resorbed maxillary anterior alveolar ridge: rationale and approach. Implant Dent. 1998; 7: 169-76. [ Links ]
2. Schwarz MS, Rothman SL, Chafetz N, Rhodes M. Computed tomography in dental implantation surgery. Dent Clin North Am. 1989; 33: 555-97. [ Links ]
3. Velvart P, Hecker H, Tillinger G. Detection of the apical lesion and the mandibular canal in conventional radiography and computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92: 682-8. [ Links ]
4. Jacobs SG. Radiographic localization of unerupted mandibular anterior teeth. Am J Orthod Dentofacial Orthop. 2000; 118: 432-8. [ Links ]
5. Rydberg J, Liang Y, Teague SD. Fundamentals of multichannel CT. Radiol Clin North Am. 2003; 41: 465-74. [ Links ]
6. Koizumi H, Sur J, Seki K, Nakajima K, Sano T, Okano T. Effects of dose reduction on multi-detector computed tomographic images in evaluating the maxilla and mandible for pre-surgical implant planning: a cadaveric study. Clin Oral Implants Res. 2010; 21: 830-4. [ Links ]
7. Kiyak HA, Beach BH, Worthington P, Taylor T, Bolender C, Evans J. Psychological impact of osseointegrated dental implants. Int J Oral Maxillofac Implants. 1990; 5: 61-9. [ Links ]
8. Bartling R, Freeman K, Kraut RA. The incidence of altered sensation of the mental nerve after mandibular implant placement. J Oral Maxillofac Surg. 1999; 57: 1408-12. [ Links ]
9. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988; 17: 232-6. [ Links ]
10. Xie Q, Wolf J, Soikkonen K, Ainamo A. Height of mandibular basal bone in dentate and edentulous subjects. Acta Odontol Scand. 1996; 54: 379-83. [ Links ]
11. Cavalcanti MG, Yang J, Ruprecht A, Vannier MW. Accurate linear measurements in the anterior maxilla using orthoradially reformatted spiral computed tomography. Dentomaxillofac Radiol. 1999; 28: 137-40. [ Links ]
12. Dantas JA, Montebello Filho A, Campos PSF. Computed tomography for dental implants: the influence of the gantry angle and mandibular positioning on the bone height and width. Dentomaxillofac Radiol. 2005; 34: 9-15. [ Links ]
13. Todd AD, Gher ME, Quintero G, Richardson AC. Interpretation of linear and computed tomograms in the assessment of implant recipient sites. J Periodontol. 1993; 64: 1243-9. [ Links ]
14. Lindh C, Petersson A, Klinge B. Measurements of distances related to the mandibular canal in radiographs. Clin Oral Implants Res. 1995; 6: 96-103. [ Links ]
15. Levine MH, Goddard AL, Dodson TB. Inferior alveolar nerve canal position: a clinical and radiographic study. J Oral Maxillofac Surg. 2007; 65: 470-4. [ Links ]
16. Watanabe H, Mohammad Abdul M, Kurabayashi T, Aoki H. Mandible size and morphology determined with CT on a premise of dental implant operation. Surg Radiol Anat. 2010; 32: 343-9. [ Links ]
17. Oliveira Júnior MR, Saud AL, Fonseca DR, De-Ary-Pires B, Pires-Neto MA, Ary-Pires R. Morphometrical analysis of the human mandibular canal: a CT investigation. Surg Radiol Anat. 2010; 33: 345-52. [ Links ]
18. Paes Ada S, Moreira CR, Sales MA, Cavalcanti MG. Comparative study of single and multislice computed tomography for assessment of the mandibular canal. J Appl Oral Sci. 2007; 15: 220-4. [ Links ]
19. Sutton DN, Lewis BR, Patel M, Cawood JI. Changes in facial form relative to progressive atrophy of the edentulous jaws. Int J Oral Maxillofac Surg. 2004; 33: 676-8. [ Links ]
20. Demetriades N, Park JI, Laskarides C. Alternative bone expansion technique for implant placement in atrophic edentulous maxilla and mandible. J Oral Implantol. 2011; 37: 463-71. [ Links ]
21. Romeo E, Bivio A, Mosca D, Scanferla M, Ghisolfi M, Storelli S. The use of short dental implants in clinical practice: literature review. Minerva Stomatol. 2010; 59: 23-31. [ Links ]
22. Juodzbalys G, Wang HL, Sabalys G, Sidlauskas A, Galindo-Moreno P. Inferior alveolar nerve injury associated with implant surgery. Clin Oral Implants Res. 2012. doi: 10.1111/j.1600-0501.2011.02314.x. [ Links ]
 Correspondence:
Correspondence:
Frederico Sampaio Neves
Departamento de Diagnóstico Oral
Faculdade de Odontologia de Piracicaba – UNICAMP
Av. Limeira, 901, Cx Postal 52, CEP: 13414-903
Piracicaba - SP - Brazil
E-mail: fredsampaio@yahoo.com.br
Received for publication: January 12, 2012
Accepted: April 18, 2012
